
Abstract
Switzerland, with a population of slightly over 7 million, has about 83,000 births per year. There is no comprehensive national registry for prenatal diagnosis (PND) or congenital malformations. Health care is largely organised within each of the 23 counties. Whereas ultrasound screening is available to all pregnant women, the availability of other types of PND is largely determined by proximity to the university medical centres or specialised clinics. Maternal biochemical serum screening is offered by some 15–20 laboratories, and cytogenetic analyses are performed in 8. DNA-based diagnosis is essentially limited to the medical genetics departments/divisions of the 5 university medical schools. It can be estimated that slightly over 10% of gestations are monitored by invasive prenatal diagnostic techniques. The greatest challenge for the future will be the training of the medical and paramedical personnel necessary for the current and future pre- and postnatal diagnostic testing.
Similar content being viewed by others

National Organisation of Prenatal Diagnosis
Switzerland, with a population of 7,019,000, had 82,890 births in 1994 (Bevölkerungsbewegung in der Schweiz 1994, Bundesamt für Statistik, Bern, 1995), a figure which has varied little over the past 3–5 years. Switzerland is a federalistic democracy, in which primary obstetrical care is provided on an extremely decentralised basis; the majority of hospitals with obstetrics divisions deliver fever than 500 babies annually and at least 25 hospitals perform less than 100 deliveries annually [1]. There are 23 counties (‘cantons’), which vary considerably in geographical availability of specialised medical services such as prenatal diagnosis (PND). The interpretation and application of regulations concerning assisted procreation, PND and abortion also differ between counties.
In this paper we consider three categories of prenatal diagnostic techniques: ultrasound screening, biochemical analysis and invasive procedures; amniocentesis, chorionic villus sampling (CVS) and cordocentesis. Whereas the majority of pregnancies are evaluated at least once by ultrasound, the exact proportion of pregnancies monitored and the median number of scans per pregnancy cannot be calculated, since echography is performed by doctors in private practice, in regional public or private clinics and in tertiary-referral university hospitals. The proportion of pregnancies monitored by biochemical screening (maternal serum α-fetoprotein, AFP, for example), although on the rise, varies from a few percent to over 50%, depending mainly on the geographical situation and the organisation of services in that county. Currently, 15–20 private and university-linked laboratories perform biochemical screening of maternal serum with the goal of identifying pregnancies at risk for chromosomal disorders and other malformations.
The use of invasive prenatal diagnostic techniques (amniocentesis, CVS and cordocentesis) is largely limited to areas with access to genetics laboratories, of which Switzerland has 8. Whereas amniocentesis and more rarely CVS are offered by obstetricians in private practice, cordocentesis is practiced almost exclusively in the university medical centres. Figure 1 shows the location of the 5 university medical genetics centres and the 3 commercial cytogenetics laboratories operating in Switzerland. All 8 offer cytogenetic analysis but DNA diagnostic testing is as yet limited to the university departments.

Map of Switzerland showing location of the 5 university (*) and 3 commercial (•) cytogenetics laboratories.
Sources of Information
Federal Level
Although most regional and/or university hospitals maintain their own registries of congenital anomalies and of PND, no comprehensive national registry appropriate for epidemiological studies exists. The two principal sources of information in these areas are the federal Invalidity Insurance (AI) system and the Swiss EUROCAT (European Registry of Congenital Anomalies and Twins) malformation registry [2, 3].
The federal AI system covers medical expenses occasioned by congenital malformations; most infants with serious birth defects are thus registered with the AI at birth (or time of diagnosis). Although only limited data from the AI are accessible to the public, some published statistics from this source will be cited in the section on the impact of PND. Switzerland has participated in EUROCAT since 1987, when the country joined thanks to a joint initiative of the Swiss Academic Medical Society and the Swiss Society of Paediatrics [2–4]. The registry is centralised in Lausanne (county of Vaud), and this county has had the most complete coverage. In 1988, it was estimated that 40% of all deliveries (on a national scale) were monitored under the system. Participation grew progressively so that since 1991 over 85% of births have been included in EUROCAT coverage. As of 1994, only three counties (representing less than 10% of births) did not yet have a EUROCAT neonatologist. Participation and coverage are, however, quite variable from one county to the other, depending on the type of population (e.g. rural or urban), the organisation of the registry and the source of funding. The proportion of births monitored can be estimated by comparing the reported rate of malformation in Switzerland to the overall EUROCAT rates. For all EUROCAT registries (1980–1992), the malformations prevalence was 23.1 per thousand births; Switzerland reported 13.8 malformations per 1,000 births between 1988 and 1992 [2–5].
Swiss EUROCAT collaborates closely with the Swiss Teratogen Information System, a Lausanne-based but nationwide service created to benefit counselling and pregnancy management in reproductive toxicology.
A number of national or regional associations are involved in monitoring developments and proposing policy in the domain of PND:
-
— the Swiss Society of Medical Genetics counts paediatricians and obstetricians as well as clinical and laboratory geneticists among its over 700 members. The Society publishes a bi-annual bulletin which includes practical information (e.g., lists of books and conferences, addresses of laboratories and lay associations) as well as scientific articles [6];
-
— the Swiss Society of Gynaecology and Obstetrics has recently proposed a protocol for monitoring spontaneous abortions occurring between 8 and 11 weeks.
Other groups having an impact on PND and which meet at least annually are the Swiss Society of Ultrasound in Medicine and Biology (SGUMB) and the Swiss Perinatal Society.
A number of lay organisations, created principally over the past 10–15 years in Switzerland, are an increasingly important source of information on specific genetic disorders.
No databases or information systems concerning PND or congenital malformations in Switzerland are accessible by Internet.
Local Level
Most university hospitals have registers of congenital anomalies which include those detected prenatally. For example, in 1995 at the University of Zurich, a tertiary-referral centre, malformations were diagnosed prenatally in 175 gestations. Such information is, however, of little epidemiological utility.
Published in Geneva four times a year is the French-language Bulletin de Périnatalogie [4, 7]; the Bulletin, offered free of charge, enjoys a wide distribution among French-speaking health professionals.
Impact of Prenatal Diagnosis
The impact of PND on the prevalence of severe congenital malformations and chromosomal disorders has not been evaluated on a national level, but some trends can be deduced from EUROCAT data or from regional studies. The 1996 EUROCAT-CH information bulletin reports [3] that 25% of the malformations reported to the system are diagnosed prenatally.
The early 1980s saw the beginnings of widespread application of prenatal ultrasound examination and of maternal serum AFP screening. Between 1980 and 1983 the 5 university centres reported a ratio of diagnosed myelomeningocele to anenencephaly of 8:14. For the period 1991–1995, at Zurich University Hospital, the corresponding ratio was 18:12. This indicates that the more serious abnormalities are currently diagnosed more often by the patient’s obstetrician, without help from a tertiary-referral centre. The IA also reported a major decrease in liveborns with certain malformations between 1983 and 1988 [9], again probably due in major part to PND of these anomalies:
Cases reported | ||
|---|---|---|
1983 | 1988 | |
Myelomeningocele | 47 | 24 |
Abdominal wall defects | 13 | 8 |
Down’s syndrome | 34 | 7 |
Another idea of the impact which PND has had on the incidence of chromosomal anomalies can be obtained from a study of the epidemiology and prevention of trisomy 21 in the county of Vaud from 1980 to 1994 [10]. If the prenatal detection rate of trisomy 21 for mothers 35 years and older has remained stable (77–78%), the proportion of prenatally diagnosed fetuses conceived by younger mothers has increased from 9.8% in the period 1980–1989 to 48.0% for the period 1990–1994 [10, and M.C. Addor, pers. commun.].
The EUROCAT subproject on congenital heart disease [2, 3, 5] was coordinated in Switzerland and included data from the 5 Swiss university centres. According to this study, the proportion of cases of congenital heart disease detected prenatally has more than tripled over the past 10 years.
The increasing availability of PND has also had an important psycho-social impact on the population in general and on couples of child-bearing age in particular. If 15 years ago, over 60% of amniocenteses studied at the Geneva University Hospital were done for advanced maternal age and 30% for ‘anxiety’ [7], the proportion of patients presenting today for those reasons is approximately equal, e.g. about 40%. This reflects the higher knowledge level of a population which is confronted with an increasing number of choices abut which they (and their doctors) are not always well informed. One of the greatest challenges for the future will be to provide adequate information and follow-up counselling for pre- and postnatal detection of genetic disease.
Increasing awareness of PND and of genetics in general has certainly also played a role in the increasing number of lay organisations available to serve individuals and families with genetic disorders.
A public increasingly aware (and wary) of genetic diagnosis and research has also placed legislative restrictions on PND (see below).
Availability of Diagnostic Procedures
In Switzerland routine ultrasound screening is offered to all pregnant women at 10 and at 20 weeks of gestation, the costs being covered by their health insurance. Additional scans are covered if the pregnancy is classified as high risk on the basis of history, clinical or ultrasound examination. Goals of the initial ultrasound exam are dating and detection of multiple pregnancies. The 20-week ultrasound is a detailed screening for malformations, placenta praevia and other pathologies.
Second-trimester maternal serum screening is not performed routinely but is available on request in all regions of the country. The proportion of pregnancies screened is variable, being about 16% in the Zurich region (large county, with numerous physicians and laboratories involved in PND) [11, 12] and nearly 60% in Geneva (small, urban county with established collaboration between private and university laboratories) [P. Bischof, pers. commun.]. Biochemical serum screening is offered to most pregnant women, depending on the policy of their obstetricians. Laboratory testing for AFP, β-hCG and free oestriol levels is performed in 15–20 university and commercial laboratories. The costs are generally defrayed by the expectant mother’s health insurance.
Amniocentesis, performed by numerous obstetricians both in private practice and in specialised clinics, is the most readily available of the invasive techniques. Chorionic villus sampling (CVS) is done mainly in the university obstetrics departments, although some practitioners, particularly in the German-speaking part of the country, do the sampling in their offices. Cordocentesis is available only in university medical centres, none of which are located in the Italian-speaking part of Switzerland. The laboratories which carry out the analysis of these three types of fetal samples are located in the 5 counties shown in figure 1.
Health insurance plans are required to cover the costs of an invasive procedure in the following situations:
-
— maternal age of 35 or older;
-
— parent or previous child with a chromosomal anomaly, neural tube defect or genetic disorder for which diagnostic testing is available;
-
— increased risk of chromosomal anomaly or malformation following maternal serum screening.
Current Methods in use
At least 75% of the obstetricians and general practitioners who care for pregnant women are involved in PND, as they perform level 1 ultrasound examinations. For all doctors, backup level 2 ultrasound is available, mostly in regional hospitals (where it may be performed by obstetricians, radiologists or experienced ultrasound technicians) or by specialists in private practice. In general, obstetricians are well trained to detect sonographic markers and well equipped to perform this ultrasound screening. In Switzerland there are 5 level 3 referral centres at the 5 university hospitals, with highly experienced examiners and high-standard technical equipment for sonomorphological diagnosis.
There exists no nationwide programme on quality control of prenatal sonographic diagnosis in Switzerland. A monitoring system to evaluate the diagnostic efficiency of prenatal ultrasound examinations at the main referral centres was initiated by the gynaecology subgroup of the Swiss Society of Ultrasound in Medicine and Biology (SGUMB) in August 1996. Currently, 1995 data have been collected from referring centres and are being analysed.
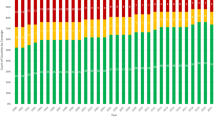
As stated earlier and shown in figures 1 and 2, cytogenetic analyses are performed in 5 university and 3 commercial laboratories. Commercial laboratories generally handle fewer cordocentesis samples than do university centres, since the latter technique is usually performed in hospital obstetric and gynaecology departments.

Comparison of utilisation of the three invasive techniques of PND in counties with diagnostic laboratories. The population of each county is given below the respective bar graph, which compares the numbers of the three procedure types performed each year. Counties marked with an asterisk have two cytogenetics laboratories.
In 1994, one can estimate the number of amniocenteses analysed nationwide at about 7,900, CVS at 2,500 and fetal blood sampling at less than 100. The total and the proportion of tests done in each of the 5 counties reflects various factors such as total population accommodated and policy of referring obstetricians. In general, CVS is currently more popular among the German-speaking population than it is in Romandy (French-speaking).
Molecular diagnostic testing in PND is offered only by the university medical centres. National regulations for quality control of laboratories are currently being formulated by the Swiss Society of Medical Genetics. Table 1 is a list of disorders for which prenatal DNA analysis is available in Switzerland, although it is not meant to be exhaustive since it is constantly evolving. In general, the 5 university laboratories provide direct mutation analysis for the more common monogenic disorders and linkage analysis for almost any Mendelian disorder mapped, in carefully selected and counselled families. Molecular cytogenetics (fluorescence in situ hybridisation, FISH) is also applied (in both university and private laboratories) for the diagnosis of the better-defined microdeletion/duplication syndromes (Williams, 22q-, Smith-Magenis), as well as for the characterisation of unusual aneuploidies.
Biochemical analyses for a number of genetic disorders, including lysosomal storage disorders, haemoglobinopathies and collagen (connective tissue) diseases are available in some of the university hospitals.
Areas under Development
The following areas of PND are currently under development:
-
(1)
First-trimester biochemical screening: research protocols, in some centres as part of an international collaboration, are underway in all 5 university hospitals to evaluate the utility of biochemical markers such as PAPP-A and free β-hCG in screening for chromosomal disorders.
-
(2)
Early amniocentesis: all 5 university centres are evaluating cytogenetic and clinical aspects of amniocentesis performed between 10 and 14 weeks.
-
(3)
Interphase cytogenetics: FISH is being applied to uncultured amniotic fluid cells under a research protocol in several university centres, with the goal of detecting aneuploidies for selected chromosomes (13),18,21, X and Y).
-
(4)
Separation of fetal cells from the maternal circulation is done only on a research basis, as part of an international collaboration in which the Basel University Hospital participates. Data concerning the efficiency of the method became available in late 1996.
Funding Arrangements for Prenatal Diagnosis
On a clinical level, health insurance (compulsory in Switzerland) pays for at least two ultrasound examinations per pregnancy and generally covers maternal biochemical serum screening. When invasive prenatal techniques are warranted on medical grounds (e.g. maternal age of at least 35, previous child with a chromosomal anomaly, increased risk on maternal serum screening), the costs of the procedure, including counselling and genetic testing, are equally covered by most health insurance companies. In most other situations invasive prenatal diagnosis is not reimbursed.
A few research projects related to prenatal diagnosis are supported by grants from the Swiss National Research Fund (FNSRS) and by the Federal Office for Education and Health (OFES):
-
— Longitudinal Measurements of Pregnancy-Associated Proteins and Hormones (University of Zurich, FNSRS 32-40391.94);
-
— Nature and Role of Cytogenetic Anomalies in Fetoplacental Interactions (University of Geneva; FNSRS 32-40864.94);
-
— European Collaborative Study on Mosaicism in Chorionic Villus Sampling (EUCROMIC), EU Concerted Action BMH1-CT93-1673 (OFES grant 93.0337, University of Geneva).
Other projects are partially subsidised by university funding as some costs for technical development and improvement are absorbed in the operating budget of the university centres. Some private subsidies (from pharmaceutical companies, for example) are equally available, but none, to our knowledge, currently funds research in the area of PND.
Current Legislation Surrounding Prenatal Diagnosis
According to Swiss law, termination of pregnancy is allowed (e.g. goes unprosecuted) if maternal health is endangered. The majority of regions practice a liberal interpretation of this law (fig. 3) [9], according to which ‘endangering maternal health’ can also include potential psychological trauma. The interpretation and the right to legally sanction the request for an abortion differ from county to county. For example, in the Zurich area psychiatrists are allowed to provide the ‘second opinion’ required by law before a pregnancy can be terminated, whereas in Bern all licensed medical doctors have this power. Prior to 12 weeks, dilation and curetage is the standard method of termination, whereas abortion after 12 weeks (and until about 22) is almost always performed by induction of labor.

Interpretations of the Swiss National Abortion Law (Art. 120 StGB) in 1970 (a) and 1996 (b). The map shows counties with a liberal (white), intermediate (shaded) and strict (black) interpretation of the law. From Dondénaz et al. [9], with permission.
Pre-implantation Diagnosis
A law limiting assisted procreation, voted by a majority of the Swiss people in 1992 (article 24 novies) specifically forbids pre-implantation diagnosis in either clinical or research settings.
In early 1995, a federally commissioned study group on human gene research recommended that research directly related to PND and treatment be permitted on unimplanted human embryos (resulting from in vitro fertilisation) throughout the blastocyst stage (14-day equivalent) [13].
Problems Faced in Prenatal Diagnosis in Switzerland
On a short-term basis, a major lack is that of a comprehensive national registry for congenital anomalies and genetic diseases, including those detected prenatally. The absence of such a tool seriously limits attempts at quality control of prenatal diagnostic procedures. Along the same line are the lack of political initiatives and of funding for the development and improvement of prenatal diagnostic techniques.
One of the problems with a decentralised system of hospital care is that of education; only a small number of individuals can be trained in the few existing university centres. There is a need for centralisation in the care of high-risk cases and the development of additional centres for perinatal medicine [1]. In our opinion, the greatest challenge we face — which will become even more critical with the development of additional and more efficient methods of pre- and postnatal diagnosis — is the dearth of trained individuals working in the various fields touching prenatal diagnosis. Specifically, no recognised medical training programme exists in human genetics: clinical genetics is not recognised as a medical subspecialty and those who practice it are either trained on the job or in foreign centres. This is also true for cytogenetic and molecular genetic laboratory personnel; criteria have been recommended by the SSGM for their training and quality control of the services, but have not yet been recognised and implemented.
Just as serious on a long-term basis is the complete lack of paramedical specialists such as genetic counsellors and genetics nurses. Education of the medical public and genetic counselling for the lay public will be such a pervasive need that development of paramedical degrees in medical genetics should have a high priority.
References
Schneider H: Regionalisation in obstetrics: Function of a perinatal center. Bull Périnat 1991;15:9–11.
Pexieder T, Bloch D: Congenital anomalies in Switzerland: Problems and solutions in data collection and their European integration experience by EUROCAT. Soz Präventivmed 1994;39:43–46.
Addor MC: Personal communication and minutes of annual EUROCAT-CH Meeting, May 1996.
Pexieder T, Hernandez T, Sabani E, Devolz M: Surveillance et épidémiologie des anomalies congénitales en Suisse. Bull Périnat 1994; 18: 2–6.
EUROCAT, Report 6, part I. Brussels, Institute of Hygiene and Epidemiology, 1995.
Moser H (ed): Bulletin d’Information de la SSGM: Répartition des members de la SSGM. Génét Méd 1994;33:17.
Dahoun-Hadorn S: Diagnostic prenatal: Expérience genèvoise des dix dernières années. Bull Périnat 1993;18:6–10.
Schweizerisches Strafgesetzbuch, ed 11. Zurich, Orell Füssli, 1986.
Dondenaz M, Gutzwiller F, Rey AM, Stamm H: Schwangerschaftsabbruch in der Schweiz. Schweiz Ärzteztg 1996;77:99–105.
Pescia G, Fokstuen S, Marguerat Ph, Addor M-C: Epidémiologie et prévention de la trisomie 21 dans le canton de Vaud 1980–1994 (abstract). Annual Meeting of the Swiss Medical Genetics Society, Lausanne, June 1995.
Zimmermann R, Vial Y: Ultraschallerfahrung und apparative Ausstattung des Schweizer Gynäkologen. Ergebnisse einer schriftlichen Umfrage. Arch Gynecol Obstet, in press.
Gutzwiller F, Grob PJ, Boppart I, Marguerat Ph: Früherfassung kindlicher Missbildungen des Rückenmarkes und des Gehirns. AFP screening. Ergebnisse einer Studie bei 16,000 schwangeren Frauen in der Schweiz. Schweiz Ärzteztg 1985;66:274–283.
Report of the Study Group for Research Concerning the Human Embryo. Département Fédéral de l’Intérieur, Bern, February 1995.
Acknowledgments
We would like to thank numerous colleagues from the Medical Genetics and Obstetrics and Gynaecology Departments of the University Hospitals for their devotion to developing prenatal diagnostic techniques in Switzerland. Several of these individuals, as well as those from the commercial cytogenetics laboratories, provided information cited in this article. We would like to thank the OFES (grant No. 93-0337 to C.D.B.) for funding our participation in the workshop on PND in Europe, organised by the concerted action project EUCROMIC (BMH1-CT93-1673) and held in Paris in May 1996; this article was written as an extension of that workshop.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
DeLozier-Blanchet, C.D., Wisser, J. Prenatal Diagnosis in Switzerland. Eur J Hum Genet 5 (Suppl 1), 77–83 (1997). https://doi.org/10.1007/BF03405967
Issue Date:
DOI: https://doi.org/10.1007/BF03405967
