
Abstract
Aims
To determine the incidence of angiographic cystoid macular oedema (CMO) following pneumatic retinopexy (PR) and scleral buckling (SB) in consecutive case series.
Methods
Patients who had successful anatomical attachment following PR and SB were included in our study; 132 patients had PR and 121 patients had SB. We evaluated the demographic characteristics, visual acuity, lens status, macular status, and previous ocular history in all patients. CMO was evaluated by fluorescein angiography (FA) in a masked pattern, 6 and 12 weeks after surgery in all cases. We analysed the CMO incidence and its correlation with preoperative ocular status and visual outcome. χ2 and Fisher's exact tests were used in statistical analysis.
Results
CMO was present in 15 of 132 (11%) PR, and 35 of 121 (29%) SB patients at 6 weeks (P=0.0005); the oedema was persistent in eight of 132 (6%) PR and 21 of 121 (17%) SB patients at 12 weeks (P=0.0005). Eight of 106 (8%) phakic and seven of 26 (27%) pseudophakic patients developed CMO following PR (P=0.02). In the SB group, 26 of 72 (36%) patients who had preoperative macular detachment developed CMO (P=0.03). Visual improvement was limited in patients who developed angiographic CMO despite anatomical re-attachment of the retina.
Conclusions
CMO may occur following both PR and SB and deteriorate the visual outcome. Previous cataract surgery and macular detachment may increase the CMO rates following PR and SB, respectively.
Similar content being viewed by others


Introduction
Pneumatic retinopexy (PR) and scleral buckling (SB) are two methods of treatment for primary rhegmatogenous retinal detachment (RD). Clinical reports indicate that final anatomic success rates are favourable following both PR and SB.1, 2, 3, 4, 5, 6, 7 There are several factors that may contribute to the visual outcome. Cystoid macular oedema (CMO) is one of these factors that has been defined following SB in previous reports.8, 9, 10 In these series, the angiographic CMO incidence was reported between 5 and 29% in phakic, 27 and 50% in pseudophakic, and 40 and 60% in aphakic patients following SB.8, 9, 10 Although angiographic CMO has been reported to be as incidental cases following PR, the real CMO frequency is not clear, as most of the previous studies2, 3, 4, 5, 6, 7 lack routine postoperative fluorescein angiography (FA) to evaluate CMO. In this study, we aimed to evaluate the incidence of angiographic CMO early after PR in comparison with SB.
Materials and methods
Two hundred and fifty-three consecutive patients with primary rhegmatogenous RD who had successful re-attachment of the retina following surgery were included in our analysis. Our study design was approved by local institutional review board. All patients signed informed consent forms before participating in our study.
One hundred and thirty-two patients had PR and 121 patients had SB during the study period. Patients with breaks involving the superior quadrants of the retina received either PR or SB after informed consent of the patient. Patients with inferior retinal tears where a PR was not suitable received a SB. We noted the demographic characteristics, preoperative ocular findings, and ocular history for each treatment cohort. Our preoperative evaluation included age, gender, eye involved, previous ocular surgery, status of the macula (attached vs detached), and the lens (phakic vs pseudophakic). Postoperative findings were noted in each postoperative visit during the follow-up. Patients who had diabetes, giant retinal tears, proliferative vitreoretinopathy, and who required additional surgery for re-detachment of the retina were excluded from our study. Surgical procedures were performed by two retinal surgeons (JML and JJK) with equivalent volume for PR and SB.
All SB patients received an encircling band with a local implant over the break(s). According to our treatment protocol, we drained subretinal fluid when necessary and applied intraoperative trans-scleral cryotherapy limited to the breaks at the time of the SB. We did not pull up the bands to any significant degree that none of our patients had a significant increase in axial length.
PR was performed by pars plana injection of 0.3–0.6 cm3 100% SF6 inside the vitreous cavity using a 27 G needle. A paracentesis was performed before and in some cases after the injection to keep the eye normotensive after the gas bubble was injected. We then gave the patient an appropriate head position (if necessary by a steam roller manoeuvre) to have the retinal breaks covered by the gas bubble. Indirect laser photocoagulation was performed in PR patients. All patients received the same postoperative medications (topical antibiotics q.i.d., 1% prednisolone acetate q.i.d., and mydriatics).
FA were taken 6 and 12 weeks after surgery. Angiograms were evaluated in a masked pattern by the same surgeon (MT). Angiographic CMO was defined with a classical perifoveal petelloid leakage of fluid and optic nerve staining at the late phase of the FA and graded between (1+) and (4+) according to the amount of leakage. In differential diagnosis, we paid particular attention to differentiate the patients who had persistent submacular fluid or epiretinal membrane (ERM) from CMO. We repeated the FA in cases who had previous CMO.
Functional outcome was evaluated by best-corrected visual acuities throughout the study period.
We used the analysis of variance (ANOVA) to determine the age and gender distribution of the patients in two treatment cohorts. χ2 test and Fisher's exact test were used to compare the CMO frequency in statistical analysis; P⩽0.05 was considered for statistical significance.
Results
The mean age was 60 (30–78) years in PR and 56 (28–82) years in SB patients. Eighty-three patients in PR group were male and 49 patients were female. In SB group, 80 patients were male and 41 were female. There was no significant difference in age and gender distribution of the patients between PR and SB by ANOVA (P>0.05).
One hundred and six of 132 PR patients were phakic and the remaining 26 patients were pseudophakic. The tear location was superior (superiotemporal or superionasal) in all patients. In 67 (51%) patients, the macula was attached before PR and 65 (49%) patients had preoperative macular detachment.
Eighty of 121 SB patients were phakic and the remaining 41 patients were pseudophakic at the time of surgery. The tear location was superior (superotemporal or superonasal) in 31 (26%), temporal in 15 (12%) and inferior in 75 (62%) patients. The macula was detached in 68 (56%), and attached in 53 (44%) SB patients.
Fifteen of 132 (11%) PR patients, and 35 of 121 (29%) SB patients developed angiographic CMO 6 weeks after surgery (P=0.005). CMO was persistent at 12 weeks in eight of 132 (6%) PR, and in 21 of 121 (17%) SB patients (P=0.005).
The mean age of PR patients who developed CMO was 58 years. Nine of 83 (11%) men and six of 49 (12%) women developed CMO following PR (P=0.78). In the SB group, 21 of 80 (26%) men and 14 of 41 (34%) women developed CMO following SB (P=0.29). There was no significant difference in age and gender distribution of the patients who developed CMO in PR and SB groups.
Regarding the lens status, eight of 106 (8%) phakic and seven of 26 (27%) pseudophakic patients developed angiographic CMO following PR (P=0.02). In the SB patients, 20 of 80 (25%) phakic and 15 of 41 (37%) pseudophakic patients developed CMO (P=0.18). Considering all patients who had RD repair, 28 of 186 (15%) phakic and 22 of 67 (33%) pseudophakic patients developed CMO (P=0.002).
Seven of 65 (11%) patients with preoperative macular detachment and eight of 67 (12%) patients without macular detachment developed CMO following PR (P=0.83). In the SB group, 26 of 72 (36%) patients with preoperative macular detachment and nine of 49 (18%) patients without macular detachment developed angiographic CMO (P=0.03).
Postoperative CMO rates in PR and SB patients in relation to preoperative ocular findings are summarized in Table 1.
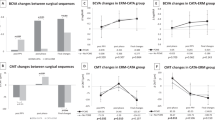
The visual improvement was limited in both PR and SB patients who had angiographic CMO early after surgery. The visual outcome of PR and SB patients in relation with the CMO status is summarized in Table 2.
Discussion
Previous reports1, 2, 3, 4, 5, 6 indicate that final anatomic success rates of PR and SB are comparable. Postoperative CMO has been reported in 14–42% of the patients following SB with an encircling band.8, 9, 10 CMO has also been reported following local scleral sponge implants without an encircling band.8 In some retrospective case series,11, 12 CMO has been reported as incidental cases following PR.
It is important to distinguish CMO from an ERM and residual submacular fluid. ERM is characterized by distortion of the vessels at the macular region and staining of the membrane without optic disc leakage. Submacular residual fluid shows diffuse staining at the macular region without optic disc leakage. The petelloid pattern of the perifoveal capillary leakage and optic disc leakage at the late phase of the FA are two important features of CMO in differential diagnosis.12, 13, 14 Optic coherence tomography (OCT) is also useful to demonstrate CMO but our study had started at a period when the OCT was not widely available; so we did not include the OCT findings in our analysis. Our results showed that the angiographic CMO incidence is 11% following PR and 29% following SB at 6 weeks.
Older age was reported to be a risk factor for CMO after ocular surgery in several reports.8, 9, 14 In contrast, our study showed no significant difference in mean age of the patients who developed CMO and those who did not.
The method of retinopexy may play a role in the difference of the CMO frequency between the SB and PR patients. Cryotherapy may induce more inflammation than laser retinopexy but previous reports15, 16 failed to demonstrate any significant increase in CMO following prophylactic cryotherapy. In a randomized clinical study comparing cryotherapy and laser retinopexy, Veckeneer et al15 showed that postoperative flare, as a measure of blood–ocular barrier breakdown, was significantly higher following cryotherapy in SB patients. Although their study15 lacks postoperative FA to detect the CMO incidence, laser retinopexy has the advantage of less inflammatory reaction that may induce postoperative CMO.
Previous reports8, 9, 10 indicate high CMO rates in aphakic and pseudophakic patients following SB. The visual outcome has also been reported to be poorer in pseudophakic patients compared to the phakic patients following PR.1, 6, 12 In parallel to these reports,1, 6, 12 our results suggest that previous cataract surgery might be a risk factor for development of CMO following PR. As previous reports2, 3, 4, 6 indicate higher single procedure retinal re-attachment rates in pseudophakic patients following SB compared to PR, in clinical practice we are more reluctant to perform PR than SB in pseudophakes, but if they meet reasonable criteria (superior retinal tears, ability to position) we offer PR but consent the patient in such a way that they are aware that the success rate is about 5–10% less than that in phakic patients.
Macular detachment has been reported with poor final vision following SB in previous series.8, 9, 17, 18, 19, 20 In SB patients, we observed higher rates of CMO if the macula was detached preoperatively compared to the patients without macular involvement. In contrast, there was no significant difference in the incidence of angiographic CMO in the PR group regarding the macular status. Recently, Ross et al21 evaluated the role of macular detachment on visual outcome of RD surgery and found a significant correlation of the height of the macular detachment with visual outcome. In our study, we did not evaluate the height of macular detachments, which could have a role in higher rates of CMO in macula-off SB patients compared to the macula-off PR patients.21 Other series1, 2, 3, 4, 5, 6, 7, 20 does not provide informative data about preoperative macular status and development of CMO.
There are certain indications for PR and it can be used as an alternative to SB in carefully selected patients. In SB procedures, intraoperative manipulations such as drainage of the subretinal fluid, intraoperative hypotony, and extensive application of cryotherapy may precipitate early postoperative inflammation and may increase CMO development.8, 9, 10 PR offers the advantages of reduced tissue trauma and a shorter surgical time.12
Our results show that CMO may develop following both PR and SB, even if the patient had successful anatomic re-attachment of the retina. Postoperative CMO may play a role in poor visual outcome. Therefore, we suggest that patients who require PR or SB should be informed about the possibility of CMO as a postoperative complication. These patients may benefit from postoperative FA and—if present—appropriate treatment of CMO.
References
Abecia E, Pinilla I, Olivan JM, Larosso JM, Polo V, Honrubia FM . Anatomic results and complications in a long-term follow-up of pneumatic retinopexy cases. Retina 2000; 20: 156–161.
Han DP, Mohsin NC, Guse CE, Hartz A, Tarkanian CN . Comparison of pneumatic retinopexy and scleral buckling in the management of primary rhegmatogenous retinal detachment. Am J Ophthalmol 1998; 126: 658–668.
Tornambe PE . Pneumatic retinopexy: the evolution of case selection and surgical technique. A twelve-year study of 302 eyes. Trans Am Ophthalmol Soc 1997; 95: 551–578.
McAllistar IL, Meyers SM, Zegarra H, Gutman FA, Zakov ZN, Beck GJ . Comparison of pneumatic retinopexy with alternative surgical techniques. Ophthalmology 1988; 95: 877–883.
Hilton GF, Kelly NE, Salzano TC, Tornambe PE, Wells JW, Wendel RT . Pneumatic retinopexy: a collaborative report of the first 100 cases. Ophthalmology 1987; 94: 307–314.
Ranta P, Kivela T . Functional and anatomic outcome of retinal detachment surgery in pseudophakic eyes. Ophthalmology 2002; 109: 1432–1440.
Wirostko WJ, Han DP, Perkins SL . Complications of pneumatic retinopexy. Curr Opin Ophthalmol 2000; 11: 195–200.
Sabates NR, Sabates FN, Sabates R, Lee KY, Ziemianski MC . Macular changes after retinal detachment surgery. Am J Ophthalmol 1989; 108: 22–29.
Meredith TA, Reeser FH, Topping TM, Aaberg TM . Cystoid macular edema after retinal detachment surgery. Ophthalmology 1980; 87: 1090–1095.
Ackerman AL, Topilow HW . A reduced incidence of cystoid macular edema following retinal detachment surgery using diathermy. Ophthalmology 1985; 92: 1092–1095.
Lisle C, Mortensen KK, Sjolie AK . Pneumatic retinopexy. A long term follow-up study. Acta Ophthalmol Scand 1998; 76: 486–490.
Holz ER, Mieler WF . View 3: the case for pneumatic retinopexy. Br J Ophthalmol 2003; 87: 787–789.
Hagimura N, Iida T, Suto K, Kishi S . Persistent foveal retinal detachment after successful rhegmatogenous retinal detachment surgery. Am J Ophthalmol 2002; 133: 516–520.
Bonnet M . Prognosis of cystoid macular edema after retinal detachment repair. Graefe's Arch Clin Exp Ophthalmol 1986; 224: 13–17.
Veckeneer M, Van Overdam KV, Bouwens D, Feron E, Mertens D, Peperkamp E et al. Randomized clinical trial of cryotherapy versus laser photocoagulation for retinopexy in conventional retinal detachment surgery. Am J Ophthalmol 2001; 132: 343–347.
Jaccoma EH, Conway BP, Campochiaro PA . Cryotherapy causes extensive breakdown of the blood–retinal barrier: a comparison with argon laser photocoagulation. Arch Ophthalmol 1985; 103: 1728–1730.
Hassan TS, Sarrafizadeh R, Ruby AJ, Garretson BR, Kuczynski B, Williams GA . The effect of duration of macular detachment on results after the scleral buckle repair of primary macula-off retinal detachments. Ophthalmology 2002; 109: 146–152.
Ross WH, Kozy DW . Visual recovery in macula-off rhegmatogenous retinal detachments. Ophthalmology 1998; 105: 2149–2153.
Burton TC . Recovery of visual acuity after retinal detachment involving the macula. Trans Am Ophthalmol Soc 1982; 80: 475–497.
Desatnik H, Alhalel A, Treister G, Moisseiev J . Management of persistent lobulated subretinal fluid after pneumatic retinopexy. Br J Ophthalmol 2001; 85: 189–192.
Ross W, Lavina A, Russel M, MAberley D . The correlation between height of macular detachment and visual outcome in macula-off retinal detachments of < or =7 days' duration. Ophthalmology 2005; 112: 1213–1217.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tunc, M., Lahey, J., Kearney, J. et al. Cystoid macular oedema following pneumatic retinopexy vs scleral buckling. Eye 21, 831–834 (2007). https://doi.org/10.1038/sj.eye.6702431
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702431
Keywords
This article is cited by
-
Postoperative complications after successful primary rhegmatogenous retinal detachment repair
BMC Ophthalmology (2023)
-
Macular edema after rhegmatogenous retinal detachment repair: risk factors, OCT analysis, and treatment responses
International Journal of Retina and Vitreous (2021)
-
Incidence and risk factors for cystoid macular edema following scleral buckling
Eye (2017)
