
Abstract
This is one of the few studies that have explored the value of baseline symptoms and health-related quality of life (HRQOL) in predicting survival in brain cancer patients. Baseline HRQOL scores (from the EORTC QLQ-C30 and the Brain Cancer Module (BN 20)) were examined in 490 newly diagnosed glioblastoma cancer patients for the relationship with overall survival by using Cox proportional hazards regression models. Refined techniques as the bootstrap re-sampling procedure and the computation of C-indexes and R2-coefficients were used to try and validate the model. Classical analysis controlled for major clinical prognostic factors selected cognitive functioning (P=0.0001), global health status (P=0.0055) and social functioning (P<0.0001) as statistically significant prognostic factors of survival. However, several issues question the validity of these findings. C-indexes and R2-coefficients, which are measures of the predictive ability of the models, did not exhibit major improvements when adding selected or all HRQOL scores to clinical factors. While classical techniques lead to positive results, more refined analyses suggest that baseline HRQOL scores add relatively little to clinical factors to predict survival. These results may have implications for future use of HRQOL as a prognostic factor in cancer patients.
Similar content being viewed by others

Main
It has become increasingly accepted that, in addition to the traditional assessment of clinical outcomes, health-related quality-of-life (HRQOL) information can play a key role in cancer research and may help in individual patient care (Detmar et al, 2002; Velikova et al, 2004). Patients' self-assessment of HRQOL is now an established end point for treatment comparisons in many cancer disease sites (Bottomley et al, 2003), particularly in advanced disease (Efficace et al, 2004a; Bottomley et al, 2005).
Theoretically, HRQOL outcomes could have various clinical applications, including supporting clinical decision-making by providing the patient's perspective or providing prognostic information. Recent studies have shown that HRQOL parameters can be independent prognostic factors for survival in cancer patients (Kramer et al, 2000). If HRQOL parameters are independent predictors of survival, they could be used in daily practice to identify patients who will benefit from a specific intervention; further, it could help to avoid over-treatment of patients who will gain no benefit from, often, toxic and aggressive therapies or to set up more tailored psychosocial intervention programmes aimed at improving patients' HRQOL. Furthermore, they could be used to better stratify patients in future cancer clinical trials, hence better interpreting study outcomes or helping identify critical areas that could help in the selection of key end points for future clinical trials.
Health-related quality-of-life prognostic factor analyses have been carried out on several different cancer populations, including, among others, lung (Herndon et al, 1999; Langendijk et al, 2000; Montazeri et al, 2001; Efficace et al, 2006), oesophageal (Blazeby et al, 2001; Fang et al, 2004), advanced breast (Luoma et al, 2003; Efficace et al, 2004a), and head and neck (de Graeff et al, 2001) cancers, highlighting the importance HRQOL scores may have in predicting survival. Only three studies have examined HRQOL and/or cognitive functioning as a prognostic factor in brain cancer (Meyers et al, 2000; Klein et al, 2003; Sehlen et al, 2003). The present study evaluates the prognostic value of HRQOL data collected from a prospective, large-scale international randomised controlled trial, by using various statistical techniques in an attempt to provide robust conclusions on the prognostic value of HRQOL in glioblastoma multiforme patients.
Methods
Treatment
In this international, multicentre study (EORTC trial 26981-22981-NCIC CE3), 573 patients with newly diagnosed glioblastoma were randomised to treatment with radiotherapy (RT) only or RT with concomitant temozolomide (TMZ) chemotherapy followed by six cycles of TMZ chemotherapy. Patients were stratified for institution, performance status (WHO performance status 0 or 1 vs 2), age (<50 vs ⩾50 years) and the extent of the resection at surgery (biopsy only vs debulking surgery/resection). The details on trial conduct and clinical outcome have previously been reported (Hegi et al, 2005; Stupp et al, 2005; Mirimanoff et al, 2006). The trial was approved by the EORTC protocol review committee and the ethics committee of each participating centre. All patients provided written informed consent.
Procedures
Health-related quality-of-life evaluations
The primary end point of the clinical trial was survival, with HRQOL being a secondary end point. Two HRQOL measures were selected for the trial: the EORTC Quality of Life Questionnaire C30 (EORTC QLQ-C30, version 2) (Aaronson et al, 1993) and the EORTC QLQ-Brain Cancer Module (QLQ-BN20) (Osoba et al, 1996). Both tools have robust psychometric properties resulting from rigorous testing and development from their use in several international cancer clinical trials (Bottomley et al, 2003). The EORTC QLQ-C30 is a core measure designed to be supplemented with disease-specific questionnaires. The EORTC QLQ-BN20 was developed specifically in patients with brain cancer. Both instruments were available in the language of all participating patients (Cull et al, 2002).
The EORTC QLQ-C30 measure comprises five functioning scales – physical, role, emotional, cognitive and social; three symptom scales – fatigue, nausea/vomiting and pain; six single item scales – dyspnoea, insomnia, appetite loss, constipation, diarrhoea and financial impact; and the overall health/global QOL scale.
The EORTC QLQ-BN20, designed for use with patients undergoing chemotherapy or RT, includes 20 items assessing visual disorders, motor dysfunction, communication deficit, various disease symptoms (e.g. headaches and seizures), treatment toxicities (e.g. hair loss) and future uncertainty.
The items on both measures were scaled and scored using the recommended EORTC procedures (Fayers et al, 2001). Raw scores were transformed to a linear scale ranging from 0 to 100, with a higher score representing a higher level of functioning or higher level of symptoms. Provided at least half of the items in the scale were completed, the scale score was calculated using only those items for which values existed.
Patients were randomised following surgery and before the start of the RT. Radiotherapy started within 6 weeks after surgery. Valid HRQOL assessments were performed at baseline, before the start of therapy, not more than 1 month before randomisation and not more than 2 weeks after randomisation.
Health-related quality of life was a mandatory aspect of this clinical trial protocol. The protocol stipulated that a responsible nurse, clinician or data manager administered the questionnaire, requesting completion and its return to the EORTC Data Centre. The EORTC guidelines for administering questionnaires were provided, ensuring a standard approach and optimal compliance of HRQOL data collection by all personnel.
Statistical analysis
For this analysis, only baseline HRQOL scores were used. To minimise the risk of false-positive results, we excluded a priori several HRQOL scales (seven from the QLQ-C30 and two from the brain module) from the analyses. The variables selected to be excluded were not expected to have any prognostic value or alternatively were known to be highly inter-correlated with other scales, thereby not contributing to the model. The final analysis included 17 HRQOL variables: eight (appetite loss, cognitive functioning, emotional functioning, fatigue, physical functioning, global health status, social functioning, insomnia) from the core questionnaire and nine (bladder control, communication deficit, drowsiness, future uncertainty, headaches, motor dysfunction, seizures, visual disorder, weakness of legs) from the brain module.
The Cox proportional hazards regression model (Cox, 1972) with overall survival measured from the time of randomisation as dependent outcome was used for both univariate and multivariate analyses. A Collett's Model Selection approach (Collett, 1994) was used with a level of significance of 0.15 for the univariate screening and stay and entry criterion of 0.05. The HRQOL scales were included as continuous factors. The model was controlled for the major established prognostic baseline clinical factors (Gorlia et al, in press): age (<50 vs ⩾50 years), performance status (0 vs 1 vs 2), extent of surgery (complete resection vs partial resection vs biopsy only), corticosteroids at entry (yes vs no), mini-mental state examination (<27 vs 27–30), O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation status (yes vs no) as well as randomly assigned therapy. The MGMT status could only be assessed in 36% of the patients and was shown to be predictive of a favourable treatment effect in patients receiving TMZ chemotherapy (Hegi et al, 2005). The MGMT promoter methylation status was included in the analysis as a stratum with three levels (methylated, unmethylated or missing). The treatment assignment was also included as a stratum (because of the interaction between treatment and MGMT methylation). All other factors were included as covariates.
Validation of the final model was undertaken by use of several refined statistical techniques. The stability of the final model was investigated using a bootstrap re-sampling procedure as proposed by Sauerbrei and Schumacher (1992), applied in the context of HRQOL (Van Steen et al, 2002). This technique generates a number of samples (each of the same size as the original data set), by randomly selecting patients and replacing them before selecting the next patient (i.e. bootstrap resampling). The frequency of inclusion of the HRQOL scores in the Cox PH regression models, including all the selected clinical factors and treatment, fitted to each of these data sets using automatic forward stepwise selection (entry level of α=0.05), can be considered to be indicative for the importance of the HRQOL factors. This technique was applied to 1000 bootstrap samples.
Deviance residuals from the model with clinical factors were plotted vs the HRQOL scores to explore the relationship between each HRQOL score and the remaining part of the hazard not already explained by clinical factors. Finally, discrimination C-indexes and Nagelkerke's R2 coefficients were computed to quantify the predictive accuracy of a model. C-index is a measure of how well a model is able to rightly predict which patient among a randomly chosen pair of patients will survive longer. Nagelkerke's R2-coefficient is a generalisation of the R2-coefficient in linear regression, which measures the percentage of variation in the dependent variable accounted for by the predictor variables. It assesses the ability of the model to separate between all patient responses based on the predictor variables.
All data analyses were performed using Statistical Analysis Software (SAS) version 9.
Results
Between June 2000 and March 2002, 573 patients from 85 institutions in 15 countries were randomised to receive either RT alone (286 patients) or RT with TMZ (287 patients). Of these patients, 248 (RT) and 242 (RT plus TMZ) had baseline HRQOL measures completed. In total, 83 (RT) and 86 (RT plus TMZ) had an assessment of their methylation status of the MGMT promoter. The analysis was performed on 490 patients with baseline HRQOL measures that represent 85.5% of the original sample size.
Clinical and quality-of-life results
The clinical results have been published (Hegi et al, 2005; Stupp et al, 2005; Mirimanoff et al, 2006). In brief, the study demonstrated that the addition of TMZ to RT for newly diagnosed glioblastoma resulted in a clinically meaningful and statistically significant survival benefit with minimal additional toxicity (unadjusted hazard ratio of 0.63 with a 95% confidence interval, 0.52–0.75; P<0.001 by the log-rank test). In addition, patients whose tumours had a methylated MGMT gene promoter benefited from TMZ, whereas those who did not have a methylated MGMT promoter derived no or only limited benefit from the addition of chemotherapy. Quality-of-life results have also been published (Taphoorn et al, 2005). Addition of TMZ during and after RT significantly improved survival without a negative effect on HRQOL. Baseline clinical characteristics for patients with a valid baseline HRQOL questionnaire are depicted in Table 1.
The distribution of the baseline clinical characteristics was very similar between patients with a valid baseline HRQOL questionnaire and those without. When comparing patients with and those without available MGMT assessment, imbalances were noticed for the clinical characteristics age, MMSE score, extent of surgery and tumour location. The percentages of patients under 50 years, with an MMSE above 27 or with a unifocal tumour location are higher in patients with a MGMT status. The subgroup of patients with MGMT promoter methylation status assessed was therefore not entirely representative of the whole trial population. A higher proportion of patients with resected tumours had the MGMT status successfully assessed due to the lack of a sufficient amount of tumour tissue in stereotactic biopsies.
Prognostic factor analysis results
Univariate analysis
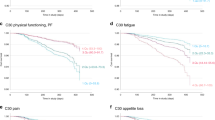
When controlled for the major prognostic clinical factors, the HRQOL scores that passed the 15% significance level were cognitive functioning, fatigue, global health status, social functioning, bladder control, headaches and motor dysfunction. Table 2 shows the results of this analysis.
Multivariate analysis
The Cox multivariate model selected by Collett's Model Selection approach contained cognitive functioning, global health status and social functioning in addition to the selected clinical factors (Table 3). However, the sign of the coefficient related to social functioning was opposite to what was expected, that is, worse social functioning was related to better survival.
Bootstrap re-sampling procedure
Table 4 presents the results of the bootstrap re-sampling procedure. The inclusion frequencies above 50% were related to cognitive functioning (83.0%), global health status (55.2%) and social functioning (88.9%). The frequencies of selection of each possible set of HRQOL scores were very low. The most frequently selected model (cognitive functioning, global health status, social functioning) was selected only 8.8% of the time. This indicates a high degree of model instability with no single model to be uniformly preferable over all others.
Discrimination index C and Nagelkerke's R2 coefficient
Discrimination C-indexes and Nagelkerke's R2 coefficients were computed for the model with clinical prognostic factors only and for various models with added HRQOL scores. The C-index of the model with only clinical baseline characteristics is C=0.647 and the Nagelkerke's R2-coefficient is R2=0.133. When adding HRQOL scores, C=0.654 and R2=0.177 for the three selected HRQOL scores and C=0.647 and R2=0.189 for all HRQOL scores. For the model without clinical factors but with all HRQOL scores, C=0.604 and R2=0.104.
Discussion
Glioblastoma, like any other malignant brain tumour, have a considerable impact on the patient's HRQOL, and in spite of important progress due to the addition of chemotherapy to RT and surgery, as a rule most glioblastoma patients will eventually suffer from tumour relapse. With such a poor prognosis, evaluation of patients' HRQOL before and during treatments becomes important. In this study, we explored if HRQOL data provide reliable and useful prognostic information. Our study used 490 glioblastoma patients, controlled for major prognostic clinical factors, and attempted to overcome limitations of past studies by using a larger sample size of homogeneously treated patients and sophisticated statistical methodology.
Previous studies in brain tumour patients showed that HRQOL factors and/or cognitive functioning were statistically significant factors in prediction models for groups of patients, comparable to our classical analysis. For example, Sehlen et al (2003) examined HRQOL in 153 patients with either malignant astrocytoma or brain metastases. Using the Functional Assessment of Cancer Therapy General HRQOL measure (Cella et al, 1993), they found two variables, that is, ‘living with a spouse’ and the FACT-G total score to predict survival. Two other studies demonstrated objective cognitive functioning to have prognostic significance, both in newly diagnosed and in recurrent high-grade glioma (Meyers et al, 2000; Klein et al, 2003). Meyers et al (2000) examined HRQOL and cognitive functioning in 80 patients with recurrent malignant glioma or anaplastic astrocytoma, at baseline, before treatment in phase I and II trials. Health-related quality of life was undertaken with the FACT-BR module, along with other neuropsychological tests. Health-related quality-of-life scores did not predict survival, but cognitive functioning was a significant predictor of survival. It is difficult to compare these findings with our results, given the different measures that were used, along with their sample being relatively small. In addition, the Phase I/II setting of Meyers et al is likely to be considerably different (higher expectations and discounting toxicities) to that of a large phase III trial (Cheng et al, 2000). Klein et al (2003) explored cognitive functioning along with activities of daily living in 68 newly diagnosed high-grade glioma patients. Cognitive functioning had prognostic value, but only in a subsample of older patients. However, it is unclear to what extent studies on such small samples can be relied on for providing definitive conclusions. It is also difficult to make comparisons between our trial and Klein et al. due to the different HRQOL measures employed.
There are several issues questioning the validity and the reliability of the results obtained by classical techniques. Some of them are well known, such as the large number of HRQOL scales and the intercorrelation of these HRQOL scales. It makes the selection of a particular set of HRQOL scores quite difficult as various sets of HRQOL scores may predict equally survival when added to clinical factors. It may also lead to models difficult to interpret (with worst HRQOL status associated with longer survival) as some HRQOL factors may enter the model just as corrections for others. In addition, as HRQOL scores are analysed as continuous factors, the results could be influenced by a few ‘outliers’, that is, patients with some very bad HRQOL scores but who actually survived long or vice versa. Furthermore, the residuals plots also suggested a high variability in duration of survival among patients who have a same level of the HRQOL scores.
C-indexes and R2-coefficients are thought to better assess the potential benefit of using baseline HRQOL scores in addition to the clinical factors to predict survival in clinical practice and research. In our study, the calculated coefficients did not exhibit major improvement when adding selected or all HRQOL scores to clinical factors, suggesting that baseline HRQOL scores in the end add relatively little to known clinical factors to predict survival and cannot be used alone in outcome prediction.
Care needs to be taken when interpreting the results of our study, given our study had limitations, particularly as this was an exploratory analysis. Also, while 490 patients represent a considerable sample, other data sets are required to validate these findings.
In summary, while traditional methods of analysis suggest HRQOL data are prognostic, more detailed analysis revealed these findings may not be as reliable as expected. Further research should investigate the use of HRQOL with more sophisticated techniques to obtain reliable results.
The investigation of the prognostic value of HRQOL data is a challenging and ongoing research area. Further research could also investigate the prognostic value of changes from baseline in HRQOL rather than baseline values and should investigate why HRQOL parameters might be of value in one setting but not another. Furthermore, the reason for this association between HRQOL data and survival is unclear. Some hypotheses have been proposed to explain the mechanisms underlying the association. Patients' HRQOL scores might reflect an early perception of the severity of the disease in a more accurate way than conventional prognostic indices. In this case, patients who report worse HRQOL scores are the ones with a worse underlying disease. This hypothesis does not imply a true causative relationship between HRQOL parameters and survival. On the other hand, it is also possible that a better HRQOL score (which reflects a better physical and psychological state) could somehow have a positive effect on the disease process by, for example, slowing tumour progression. This causative explanation could be supported by some intervention studies which have shown that psychosocial support improved both psychological well-being and survival time. Coates et al (2000) assumed that, if the mechanism underlying the association between HRQOL and survival is causative, one should expect to see HRQOL parameters being prognostic of clinical outcomes, not only in patients with metastatic disease, but also at an earlier stage of the disease. Given this assumption, and the fact that their study did not find a correlation between HRQOL parameters and disease-free survival in their nonmetastatic breast cancer population, the authors argued in favour of the explanation that HRQOL scores reflect a more accurate perception of the severity of the underlying illness. The results of Efficace et al (2004a, 2004b) also seem to support this view. Hence, it would be possible to speculate that for early stage disease, clinical examinations (such as performance status or tumour staging) are more likely to supersede patients' self-reported HRQOL scores in predicting survival. However, more studies are required to definitively exclude any possible causative relationship with survival.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85: 365–376
Blazeby JM, Brookes ST, Alderson D (2001) The prognostic value of quality of life scores during treatment for oesophageal cancer. Gut 49: 227–230
Bottomley A, Flechtner H, Efficace F, Vanvoorden V, Coens C, Therasse P, Velikova G, Blazeby J, Greimel E (2005) Health related quality of life outcomes in cancer clinical trials. Eur J Cancer 41: 1697–1709
Bottomley A, Vanvoorden V, Flechtner H, Therasse P (2003) The challenge and achievements of implementation of quality of life research in cancer clinical trials. Eur J Cancer 39: 275–285
Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, Silberman M, Yellen SB, Winicour P, Brannon J (1993) The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol 11 (3): 570–579
Cheng JD, Hitt J, Koczwara B, Schulman KA, Burnett CB, Gaskin DJ, Rowland JH, Meropol NJ (2000) Impact of quality of life on patient expectations regarding phase I clinical trials. J Clin Oncol 18 (2): 421–428
Coates AS, Hurny C, Peterson HF, Bernhard J, Castiglione-Gertsch M, Gelber RD, Goldhirsch A (2000) Quality-of-life scores predict outcome in metastatic but not early breast cancer. International Breast Cancer Study Group. J Clin Oncol 18 (22): 3768–3774
Collett D (1994) Modelling Survival Data in Medical Research. Chapman & Hall: London
Cox DR (1972) Regression models and life tables. J Royal Stat Soc 34: 187–220
Cull A, Sprangers M, Bjordal K, Aaronson N (2002) EORTC Quality of Life Group Translation Procedure. EORTC Publications: Brussels, ISBN: 2-930064-28-5
de Graeff A, de Leeuw JR, Ros WJ, Hordijk GJ, Blijham GH, Winnubst JA (2001) Sociodemographic factors and quality of life as prognostic indicators in head and neck cancer. Eur J Cancer 37: 332–339
Detmar SB, Muller MJ, Schornagel JH, Wever LD, Aaronson NK (2002) Health-related quality-of-life assessments and patient–physician communication: a randomized controlled trial. JAMA 288 (23): 3027–3034
Efficace F, Biganzoli L, Piccart M, Coens C, Van Steen K, Cufer T, Coleman RE, Calvert HA, Gamucci T, Twelves C, Fargeot P, Bottomley A (2004a) Baseline health-related quality-of-life data as prognostic factors in a phase III multicentre study of women with metastatic breast cancer. Eur J Cancer 40 (7): 1021–1030
Efficace F, Bottomley A, Smit EF, Lianes P, Legrand C, Debruyne C, Schramel F, Smit HJ, Gaafar R, Biesma B, Manegold C, Coens C, Giaccone G, Van Meerbeeck J (2006) Is a patient's self-reported health-related quality of life a prognostic factor for survival in non-small-cell lung cancer patients? A multivariate analysis of prognostic factors of EORTC study 08975. Ann Oncol 17 (11): 1698–1704
Efficace F, Therasse P, Piccart MJ, Coens C, van Steen K, Welnicka-Jaskiewicz M, Cufer T, Dyczka J, Lichinitser M, Shepherd L, de Haes H, Sprangers MA, Bottomley A (2004b) Health-related quality of life parameters as prognostic factors in a nonmetastatic breast cancer population: an international multicenter study. J Clin Oncol 22 (16): 3381–3388
Fang FM, Tsai WL, Chiu HC, Kuo WR, Hsiung CY (2004) Quality of life as a survival predictor for esophageal squamous cell carcinoma treated with radiotherapy. Int J Radiat Oncol Biol Phys 58: 1394–1404
Fayers P, Aaronson N, Bjordal K, Groenvold M, Curran D, Bottomley A (2001) EORTC QLQ-C30 Scoring Manual. EORTC Publications: Brussels, ISBN: 2-930064-22-6
Gorlia T, van den Bent MJ, Hegi M . Nomograms for predicting survival of patients with newly diagnosed glioblastoma multiforme: a prognostic factor analysis of EORTC/NCIC trial 26981-22981/CE. Clin Oncol (in press)
Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, Kros JM, Hainfellner JA, Mason W, Mariani L, Bromberg JE, Hau P, Mirimanoff RO, Cairncross JG, Janzer RC, Stupp R (2005) MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 352 (10): 997–1003
Herndon JE, Fleishman S, Kornblith AB, Kosty M, Green MR, Holland J (1999) Is quality of life predictive of the survival of patients with advanced non-small cell lung carcinoma? Cancer 5 85 (2): 333–340
Klein M, Postma TJ, Taphoorn MJ, Aaronson NK, Vandertop WP, Muller M, van der Ploeg HM, Heimans JJ (2003) The prognostic value of cognitive functioning in the survival of patients with high-grade glioma. Neurology 61 (12): 1796–1798
Kramer JA, Curran D, Piccart M, de Haes JC, Bruning P, Klijn J, Van Hoorebeeck I, Paridaens R (2000) Identification and interpretation of clinical and quality of life prognostic factors for survival and response to treatment in first-line chemotherapy in advanced breast cancer. Eur J Cancer 36: 1498–1506
Langendijk H, Aaronson NK, de Jong JM, ten Velde GP, Muller MJ, Wouters M (2000) The prognostic impact of quality of life assessed with the EORTC QLQ-C30 in inoperable non-small cell lung carcinoma treated with radiotherapy. Radiother Oncol 55: 19–25
Luoma ML, Hakamies-Blomqvist L, Sjöström J, Pluzanska A, Ottoson S, Mouridsen H, Bengtsson NO, Bergh J, Malmstrom P, Valvere V, Tennvall L, Blomqvist C (2003) Prognostic value of quality of life scores for time to progression (TTP) and overall survival time (OS) in advanced breast cancer. Eur J Cancer 39 (10): 1370–1376
Meyers CA, Hess KR, Yung WK, Levin VA (2000) Cognitive function as a predictor of survival in patients with recurrent malignant glioma. J Clin Oncol 18 (3): 646–650
Mirimanoff RO, Gorlia T, Mason W, Van den Bent MJ, Kortmann RD, Fisher B, Reni M, Brandes AA, Curschmann J, Villa S, Cairncross G, Allgeier A, Lacombe D, Stupp R (2006) Radiotherapy and temozolomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. J Clin Oncol 24 (16): 2563–2569
Montazeri A, Milroy R, Hole D, McEwen J, Gillis CR (2001) Quality of life in lung cancer patients: as an important prognostic factor. Lung Cancer 31 (2–3): 233–240
Osoba D, Aaronson NK, Muller M, Sneeuw K, Hsu MA, Yung WK, Brada M, Newlands E (1996) The development and psychometric validation of a brain cancer quality-of-life questionnaire for use in combination with general cancer-specific questionnaires. Qual Life Res 5 (1): 139–150
Sauerbrei W, Schumacher M (1992) A bootstrap resampling procedure for model building: application to the Cox regression model. Stat Med 11: 2093–2109
Sehlen S, Lenk M, Hollenhorst H, Schymura B, Aydemir U, Herschbach P, Duhmke E (2003) Quality of life (QoL) as predictive mediator variable for survival in patients with intracerebral neoplasma during radiotherapy. Onkologie 26 (1): 38–43
Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352 (10): 987–996
Taphoorn MJ, Stupp R, Coens C, Osoba D, Kortmann R, van den Bent MJ, Mason W, Mirimanoff RO, Baumert BG, Eisenhauer E, Forsyth P, Bottomley A (2005) Health-related quality of life in patients with glioblastoma: a randomized controlled trial. Lancet Oncol 6 (12): 937–944
Van Steen K, Curran D, Kramer J, Molenberghs G, Van Vreckem A, Bottomley A, Sylvester R (2002) Multicollinearity in prognostic factor analyses using the EORTC QLQ-C30: identification and impact on model selection. Stat Med 21 (24): 3865–3884
Velikova G, Booth L, Smith AB, Brown PM, Lynch P, Brown JM, Selby PJ (2004) Measuring quality of life in routine oncology practice improves communication and patient well-being: a randomized controlled trial. J Clin Oncol 22 (4): 714–724
Acknowledgements
The data for this analysis were collected by EORTC Brain Tumor Group (BTG), Radiation Oncology Group (ROG) and National Cancer Institute of Canada (NCIC) investigators. This initial clinical trial was conducted by the European Organisation for Research and Treatment of Cancer (EORTC). This research study was supported in part by grants from the National Cancer Institute (5U10CA11488-30 through 5U10CA11488-34) and by the EORTC BTG. We thank all the patients who kindly agreed to participate in this study and all the investigators for their involvement. We kindly thank Dr L Collette at the EORTC for providing support for applying the refined statistical techniques, specifically the computation of C-indexes to our data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Mauer, M., Stupp, R., Taphoorn, M. et al. The prognostic value of health-related quality-of-life data in predicting survival in glioblastoma cancer patients: results from an international randomised phase III EORTC Brain Tumour and Radiation Oncology Groups, and NCIC Clinical Trials Group study. Br J Cancer 97, 302–307 (2007). https://doi.org/10.1038/sj.bjc.6603876
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603876
Keywords
This article is cited by
-
Health-related quality of life and neurocognitive functioning in patients with recurrent glioblastoma treated with intracerebral immune checkpoint inhibition
Journal of Neuro-Oncology (2024)
-
Evaluating patient reported outcomes and experiences in a novel proton beam clinic – challenges, activities, and outcomes of the ProtonCare project
BMC Cancer (2023)
-
Health related quality of life trajectories after stereotactic radiosurgery for brain metastases: a systematic review
Journal of Neuro-Oncology (2022)
-
The major effects of health-related quality of life on 5-year survival prediction among lung cancer survivors: applications of machine learning
Scientific Reports (2020)
-
The patients’ view: impact of the extent of resection, intraoperative imaging, and awake surgery on health-related quality of life in high-grade glioma patients—results of a multicenter cross-sectional study
Neurosurgical Review (2018)
