
Abstract
Hodgkin's disease mortality rates steadily declined by about 75% between the late 1960's and the late 1990's in the current European Union countries and the USA, and Japan. Eastern European countries, however, showed only an approximately 40% decline between the late 1960's and the early 1990's, and no further fall thereafter.
Similar content being viewed by others

Main
Effective integrated chemo- and radiotherapy has made Hodgkin's disease (HD) a largely curable disease (Hoppe et al, 1994; La Vecchia et al, 1991). Between 1960 and 1990 mortality from Hodgkin's disease declined by over 60% in western Europe, and even to a greater extent in the USA and Japan. However, in former non-market economy eastern European countries the fall has been only about 30% (Levi et al, 1995). Recent economical and social developments in several eastern European countries have been associated with a fall in total mortality (Zatonski and Boyle, 1996; Zatonski et al, 1998) as well as in mortality from curable neoplasm such as testicular cancer (Becker and Boyle, 1997; Levi et al, 2001).
Methods
We considered, therefore, recent trends in mortality from Hodgkin's disease in the European Union (EU, comprising Austria, Belgium, Denmark, Finland. France, Germany, Greece, Ireland, Italy, Luxembourg, Netherlands, Portugal, Spain, Sweden, UK), six eastern European countries providing data to the WHO mortality database (Bulgaria, the Czech Republic, Hungary, Poland, Romania, Slovakia), and, for comparative purposes, the USA and Japan. We obtained estimates of the resident population and numbers of deaths from the WHO Database, recoding the latter according to the Ninth Revision of the International Classification of Diseases. Age-adjusted rates, by 5-year age groups, were based on the world standard population (Doll and Smith, 1982). The methods have been discussed in detail elsewhere (Levi et al, 1999); however, mortality for HD in European countries has not been comprehensively examined.
Results
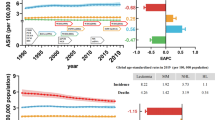
Figure 1 gives trends in mortality from HD in four broad geographic areas. In the late 1960's, mortality rates from Hodgkin's disease were very similar in the EU, eastern European countries and the USA, i.e. around 2/100 000 men and 1.2/100 000 women. Rates were appreciably lower (around 0.7/100 000 men, 0.4 for women) in Japan. In all the areas considered, substantial falls in mortality were observed, which were earlier and greater throughout the 1970's and 1980's in the USA as compared to the EU, and only in the late 1990's did HD mortality in the EU (0.53/100 000 men, 0.33 for women) approach that in the USA (0.47/100 000 men, 0.32 for women). The overall fall in men between 1965 and 1998 was 74% in the EU and 77% in the USA, and 71 and 72%, respectively, for women. Between the late 1980's and the late 1990's, the fall was 40% for males and 34% for females in the EU, 34% for males and 24% for females in the USA. Although Japan had very low rates in the 1960's, a further appreciable fall was observed, to reach rates of 0.08/100 000 men and 0.04 for women in 1995–98.

Trends in age-adjusted (world population) overall death certification rates from Hodgkin's disease per 100 000 men (a) and women (b) in the European Union, selected eastern European countries (Bulgaria, Czech Republic, Hungary, Poland, Romania and Slovakia), USA and Japan, from 1965–69 to 1995–98.
Eastern European countries showed an approximately 40% decline in HD mortality between the late 1960's and the early 1990's, to reach 1.26/100 000 men and 0.68 women. However, no appreciable further fall was observed over more recent years, and the rates were 1.18/100 000 men and 0.62 for women in 1995–98.
Table 1 shows age-adjusted death rates from HD for men and women in 19 European countries besides the EU, USA and Japan in 1965–69 and 1995–98. In most western European countries, rates fell by 70–80% over the last three decades. However, the decline in HD mortality was much less (10 to 30%) in selected eastern European countries. About a third of patients dying from HD are aged 15 to 44 years. The pattern of trends in the young across most countries was similar to that for all ages. For men aged 15 to 44 the fall was 79% (from 1.9 to 0.4/100 000) in the EU, 77% (from 2.1 to 0.5/100 000) in the USA, and 82% (from 0.3 to 0.1/100 000) in Japan. Corresponding values for women were −79% (from 1.3 to 0.3/100 000) in the EU, −75% (from 1.2 to 0.3/100 000) in the USA, and −80% (from 0.2 to 0.04/100 000) in Japan.
Discussion
The present data indicate that HD mortality in the EU, the USA and Japan has continued to decline, though to a smaller degree, over more recent calendar periods, and hence confirms the persistence of advancements in the integrated treatment of HD. Rates are exceedingly low in Japan, whose HD mortality was already a third than those of North America and Europe in the 1960's, and is now less than a fifth than in other developed areas of the world. It is unlikely that differences in death certification validity and accuracy can explain such large differences.
The decline in HD mortality was similar in the older age groups, while for leukaemias the falls tend to be greater at younger age (Levi et al, 2000). This suggests that advancements in treatment for HD had a favourable impact also in the elderly.
In eastern Europe, there has been not only a substantial delay in the fall of HD mortality, but no progress has been observed during the 1990's, although efficacious chemotherapy schemes for HD (Hoppe et al, 1994), as well as radiotherapy, should, in principle, now be available in those countries, too. These unfavourable trends contrast with the declines in mortality from cardiovascular diseases and total mortality observed from the early 1990's onwards in Poland, Hungary, the Czech Republic and other major eastern European countries (Zatonski and Boyle, 1996; Zatonski et al, 1998). Thus, over a thousand potentially avoidable deaths per year from HD, largely at younger ages, with an associated loss of many decades of life expectancy, are still taking place in these countries every year.
As already observed for childhood leukaemia (La Vecchia et al, 1998; Levi et al, 2000) and testicular cancer (Levi et al, 2001), the fall in mortality for HD has been earlier and greater in North America than in western Europe. Even to a more dramatic extent than for childhood leukaemias or testicular cancer, the present data indicate that substantial inadequacies are persistent in the management of curable neoplasms in eastern European countries, pointing to the need for a rational organization of cancer control and treatment in those countries.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Becker N, Boyle P (1997) Decline in mortality from testicular cancer in West Germany after reunification. Lancet 350: 744
Doll R, Smith PG (1982) Comparison between registries: age-standardized rates. In Cancer Incidence in Five Continents Vol. IV: (Waterhouse JAH, Muir CS, Shanmugaratnam K, Powell J, Peacham D, Whelan S (eds) pp 671–675, IARC Scientific Publication No 42 Lyon IARC
Hoppe RT, Hanton AL, Hanks GE, Owen BO (1994) Progress in the treatment of Hodgkin's disease in the United States, 1973 versus 1983. Cancer 74: 3198–3203
La Vecchia C, Levi F, Lucchini F, Kaye SB, Boyle P (1991) Hodgkin's mortality in Europe. Br J Cancer 64: 723–734
La Vecchia C, Levi F, Lucchini F, Lagiou P, Trichopoulos D, Negri E (1998) Trends in childhood cancer mortality as indicators of quality of medical care in the developed world. Cancer 83: 2223–2227
Levi F, La Vecchia C, Lucchini F, Te VC, Franceschi S (1995) Mortality from Hodgkin's disease and other lymphomas in Europe, 1960-1990. Oncology 52: 93–96
Levi F, Lucchini F, Negri E, Boyle P, La Vecchia C (1999) Cancer mortality in Europe, 1990–94, and an overview of trends 1955 to 1994. Eur J Cancer 35: 1477–1516
Levi F, Lucchini F, Negri E, Barbui T, La Vecchia C (2000) Trends in mortality from leukemia in subsequent age groups. Leukemia 14: 1980–1985
Levi F, La Vecchia C, Boyle P, Lucchini F, Negri E (2001) Western and eastern European trends in testicular cancer mortality. Lancet 357: 1853–1854
Zatonski WA, Boyle P (1996) Health transformations in Poland after 1988. J Epidemiol Biostat 4: 185–193
Zatonski WA, McMichael AJ, Powles JW (1998) Ecological study of reasons for sharp decline in mortality from ischaemic disease in Poland in 1991. Br Med J 316: 1047–1051
Acknowledgements
This work was supported by the Swiss League against Cancer and the Italian Association for Cancer Research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Levi, F., Lucchini, F., Negri, E. et al. Trends in mortality from Hodgkin's disease in western and eastern Europe. Br J Cancer 87, 291–293 (2002). https://doi.org/10.1038/sj.bjc.6600452
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6600452
Keywords
This article is cited by
-
The prevalence of opportunistic infections and malignancies in autopsied patients with human immunodeficiency virus infection in Japan
BMC Infectious Diseases (2014)
-
Changes in period and cohort effects on haematological cancer mortality in Spain, 1952-2006
BMC Cancer (2014)
-
Innovations in health care and mortality trends from five cancers in seven European countries between 1970 and 2005
International Journal of Public Health (2014)
-
Epidemiology of Hodgkin's disease and non-Hodgkin's lymphoma
European Journal of Nuclear Medicine and Molecular Imaging (2003)
