
Abstract
Respiratory physiologists traditionally attribute the increased ventilatory response to hypoxia to increased discharge by the carotid-body chemoreceptor, which is transmitted by sensory processes to neurons in the medullary nucleus of the solitary tract1. However, Lipton et al. propose a radically new model2 in which hypoxia causes haemoglobin to release molecules derived from nitric oxide, which then increase ventilation by directly stimulating solitary-tract neurons. Despite the apparent feasibility of this model3,4,5, we show here that the observations of Lipton et al.2 do not invalidate the classic carotid-body-mediated explanation of the hypoxic ventilatory response. We thus question the justification for a new model to account for hypoxia's effect on breathing.
Similar content being viewed by others

Main
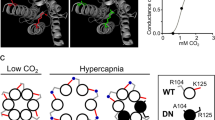
Lipton and colleagues' proposal that molecules derived from nitric oxide, called S-nitrosothiols (SNOs), duplicate the physiological response to hypoxia is based on three observations. First, they observed an equivalent increase in ventilation after separate injections into the rat nucleus tractus solitarius (NTS) of equimolar concentrations of S-nitrosocysteinyl glycine (CGSNO), S-nitroso-l-cysteine (l-CSNO) and S-nitrosoglutathionine (GSNO). Second, injection of an extract of deoxygenated, but not oxygenated, blood reproduced the effect of these agents. Third, the response to 10% O2 mirrored that produced by CGSNO, CSNO and GSNO, and the decay characteristics of the recovery of ventilation were identical in each case. No data are presented to support this final claim, but the authors' Figs 2 and 3 reveal widely different time constants of about 120 seconds after hypoxia, 60 s after CGSNO, and 240 s after blood extract.
If SNOs mediate the hypoxic ventilatory response (HVR), the effect of SNOs and hypoxia should disappear in response to blocking any step between the proposed release of SNOs at the NTS and the increased respiratory motor output. Acivicin, which blocks a step involving γ-glutamyl transpeptidase (γ-GT), abolished the ventilatory response to GSNO in rats, but the HVR persisted, as it did in mice genetically deficient in γ-GT (ref. 2). SNOs thus increase ventilation at the NTS through a γ-GT-dependent mechanism, but the HVR is independent of γ-GT; SNOs are therefore not essential for this response.
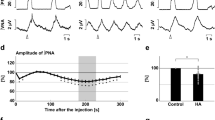
Lipton et al. also propose that SNOs are crucial for the return of ventilation to normal when air replaces hypoxic inspired gas2, with SNOs effecting a residual stimulation of ventilation during this recovery phase. This suggestion is based on their findings that pretreatment with acivicin leads to a marked acceleration of ventilatory decay after hypoxia in rats, and that hypoxic ventilatory recovery is profoundly attenuated in knockout mice that lack γ-GT, which manifests itself as an undershoot in ventilation after 60 s.
We contend that key features of this evidence conflict with earlier work. Ventilation is shown as increasing continuously during 5 min of hypoxia in rats2, whereas the typical response is a rapid increase in ventilation, then a decline as hypoxia continues; this well-known biphasic HVR occurs in many species, including humans6 and, crucially, mice7 and rats8. The slow decline in ventilation after a return to air2 is also unusual because ventilation falls rapidly on termination of hypoxia in humans9, lambs10 and mice7.
We suggest that the 3-litre plethysmograph used by Lipton et al., through which gas passed at 8 litres per min, is likely to have slowed changes in gas concentration2. Consistent with this, the reported ramp-like increase in ventilation in response to hypoxia2 is identical to that seen in lambs exposed to progressive hypoxia10, and the 2-min return to baseline ventilation upon returning to air2 suggests that hypoxia is persisting.
Furthermore, although the ventilatory undershoot after returning to air is considered to be abnormal2, it is in fact well documented7,9,10 and has been explained by the development of hypocapnia during the HVR9. The duration of hypoxic exposure and the associated fall in blood and tissue CO2 levels influence whether undershoot occurs9 — so without information on blood gases2, a chemical-control explanation for the presence or absence of undershoot cannot be discounted.
We suggest that attribution of an important role to SNOs in the HVR is not justified on the basis of Lipton and colleagues' present results, a conclusion that is supported by a wealth of evidence that the response to hypoxaemia is negligible in animals and humans with denervated or resected carotid bodies11.
References
Heymans, C. & Neil, E. Reflexogenic Areas of the Cardiovascular System (Churchill, London, 1958).
Lipton, A. J. et al. Nature 413, 171–174 (2001).
Lipton, S. A. Nature 413, 118–121 (2001).
Butcher, J. Lancet 358, 897 (2001).
Mato, J. M., Avila, M. A. & Corrales, F. J. Nature Med. 7, 1107–1108 (2001).
Easton, P. A., Slykerman, L. J. & Anthonisen, N. R. J. Appl. Physiol. 61, 906–911 (1986).
Robinson, D. M. et al. J. Appl. Physiol. 88, 1907–1914 (2000).
Maxova, H. & Vizek, M. Physiol. Res. 50, 327–331 (2001).
Badr, M. S., Skatrud, J. B. & Dempsey, J. A. J. Appl. Physiol. 73, 1958–1971 (1992).
Bureau, M. A. et al. J. Appl. Physiol. 61, 836–842 (1986).
Honda, Y. J. Appl. Physiol. 73, 1–8 (1992).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Berger, P., Skuza, E., Brodecky, V. et al. The ventilatory response to hypoxia. Nature 419, 686 (2002). https://doi.org/10.1038/419686a
Issue Date:
DOI: https://doi.org/10.1038/419686a
This article is cited by
-
Head-and-neck paragangliomas are associated with sleep-related complaints, especially in the presence of carotid body tumors
Sleep and Breathing (2012)
-
Hypoxic ventilatory decline during the first 7 days of exposure in intermittent mountain altitude between 4400 and 6960 m
Sport Sciences for Health (2009)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
