
Abstract
Study design:
Prospective, cross-sectional, case–control study.
Setting:
Outpatient department in Seoul, Korea.
Objectives:
To assess prostate volume and serum prostate-specific antigen (PSA) levels in Korean men with spinal cord injury (SCI).
Methods:
A total of 31 SCI patients with ages ranging between 45 and 81 years old (median age, 58 years) were studied. Thirty-one age-matched individuals without SCI were enrolled in the study as controls. We tested PSA levels and performed transrectal ultrasonographies on all enrolled patients. Of the patients with SCI, 20 were evaluated for testosterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH) levels.
Results:
Serum PSA levels and prostate volume parameters in the two groups had similar values: the median (5th–95th percentiles) serum PSA level was 1.56 ng/ml (0.12–9.77) for SCI patients and 1.04 ng/ml (0.50–2.98) for controls (P=0.481), whereas the median (5th–95th percentiles) prostate volume was 18.33 ml (10.16–76.78) for SCI patients and 20.80 ml (14.23–41.22) for controls (P=0.072). No significant differences were found when serum PSA levels and prostate volumes were compared according to SCI patient injury characteristics. Testosterone levels were lower than the normal range in 7 SCI patients (35%), LH was higher than the normal range in 10 SCI patients (20%), and FSH was higher than the normal range in eight SCI patients (40%). We observed an age-related increase in FSH levels (r=0.634, P=0.004), although hormone levels did not correlate with serum PSA levels and prostate volume parameters.
Conclusions:
According to our results, serum PSA levels and prostate volume in Korean SCI patients are not different from those in uninjured men and are not affected by injury characteristics.
Similar content being viewed by others

Introduction
Studies of patients with spinal cord injury (SCI) have shown that prostate cancer incidence is lower in SCI patients than in the general population.1 Theoretically, the low testosterone levels that are typically found in SCI patients may provide some protection against prostate cancer.2, 3, 4 In addition to androgen, the extensive presence of adrenergic and cholinergic receptors in the prostate suggests that autonomic nerves may be involved in prostatic function.5 Although the exact reasons for prostate gland growth are still not completely understood, animal experiments in rats with SCI indicate that neurogenic factors play an important role in prostate growth and function.6 As severe SCI paralysis can protect against cancer of the prostate gland through a neurohormonal effect,7 a similar paralysis might explain a reduced prostate size.
Recent investigations have demonstrated that SCI patients have higher levels of serum prostate-specific antigen (PSA) than healthy men.8 Because PSA can be used as a parameter for the assessment of the degree of prostate secretory dysfunction,9 this elevation has been postulated to be caused by prostatic secretory dysfunction or prostatic infection. In the present study, we compared the results obtained from SCI patients and healthy controls to determine whether SCI causes alterations in prostate volume and serum PSA levels. To date, no data are available about prostate activity in Asian men with SCI. In addition, as there are controversies over the relationship between serum PSA and androgen,1, 8 we evaluated hormone status in some of the SCI patients. The purpose of this study was to assess prostate volume and serum PSA levels in Korean men with SCI.
Materials and methods
Patients
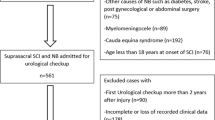
We enrolled a total of 31 SCI patients between 45 and 81 years old (median age, 58 years old), who visited our hospital and were willing to undergo examinations. Patients were excluded from the analysis if they had a history of or had undergone treatment for acute or chronic prostatitis in the last 3 months, had received a diagnosis of prostate cancer, had undergone prostate surgery or radiation treatment, had received 5α-reductase inhibitors, or had signs or symptoms compatible with a current urinary infection. During the SCI patient survey period, we enrolled 31 individuals without SCI as controls for prostate cancer screening, regardless of whether these patient visits were primary or referred. Patients and healthy controls were matched by age. The Institutional Review Board of our hospital approved the protocol and all participants signed an informed consent agreement.
Methods
All men underwent detailed clinical examinations, including a quantitation of total PSA serum levels by immunoradiometric assay (Izotop, Hungary), a digital rectal examination (DRE), and a transrectal ultrasonography (TRUS). Of the SCI patients, 20 were evaluated for hormone levels, including total testosterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH). To limit the influence of fluctuations in plasma testosterone levels owing to its episodic secretion, blood samples were always drawn at the same time of the day, that is, 0800–1000 h. The patient age, cause of paralysis, duration, level, and grade of paralysis, and method of urinary drainage were also recorded. Blood samples were obtained before patients were examined by a physician. All blood was stored at −70°C for less than 1 week and assayed for serum PSA concentrations.
Transaxial and sagittal scanning of the prostate was performed by a radiologist experienced in this procedure. Scans were performed using a 7.0 MHz transducer (Ultramake 9, ATL Inc., WA, USA). Total prostate volume (TPV) and transition zone volume (TZV) were measured and the transition zone index (TZI) was calculated as the ratio of TZV to TPV. PSA density (PSAD) and PSA adjusted for the TZV (PSAT) were determined by dividing the serum PSA concentration by TPV and TZV, respectively. Men with abnormal DREs and/or serum PSA levels greater than 4.0 ng/ml underwent a TRUS-guided needle biopsy by a radiologist. Biopsies were carried under ultrasound guidance with a biopsy gun and an 18-gauge biopsy needle (three cores from each side: apex, midpoint and base). Hypoechoic lesions found on ultrasonography and areas corresponding to a palpable abnormality on the DRE were also biopsied.
Statistical analysis
Values of continuous variables are presented as the median (5th–95th percentiles) and rates are expressed as numbers (%). Comparisons for serum PSA levels and prostate volume parameters were made between SCI patients and healthy controls. These parameters were compared in SCI patients according to patient characteristics. Patient characteristics included patient age, age at injury, duration of SCI, injury characteristics and type of bladder drainage. The level of injury was divided into two groups that were modified from the description by Frisbie et al.10 T10 or higher and lower than T10. Bladder management methods included spontaneous voiding (Crede maneuver, reflex voiding or condom catheter), intermittent catheter, suprapubic catheter and urethral catheter. Those with an indwelling catheter (suprapubic cystostomy or urethral catheterization) underwent routine catheter exchange monthly.
Comparisons of data for serum PSA levels and prostate volume parameters were made using the Mann–Whitney U-test or the Kruskal–Wallis test. Serum PSA levels and prostate volume parameters were correlated with age, age at injury and SCI duration using the Spearman correlation coefficient. The Spearman correlation test was also used to assess the significance of correlations for hormones and age, serum PSA levels or prostate volume parameters (completed for only the 20 patients who had undergone hormone evaluation). A 5% level of significance was used for all statistical testing and all statistical tests were two-sided. The statistical software package SPSS 11.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
In the 31 SCI patients, the cause of paralysis was traffic accidents for 15 men, a fall for 10 men, gunshot wounds for four men, and other miscellaneous circumstances in two men. Of all 62 subjects, six patients with SCI had serum PSA concentrations greater than 4.0 ng/ml (4.10, 4.25, 6.13, 7.50, 8.29 and 12.00 ng/ml) or abnormal DRE findings (one had both). These men underwent TRUS and TRUS-guided biopsy. No patients were found to have either prostate cancer or histological inflammation of the prostate.
Table 1 characterizes the SCI and control groups. The median (5th–95th percentiles) serum PSA level was 1.56 ng/ml (0.12–9.77) for patients and 1.04 ng/ml (0.50–2.98) for control subjects. Serum PSA levels and prostate volume parameters were similar between the two groups.
When serum PSA levels and prostate volume parameters were compared in SCI patients according to patient characteristics, the PSAT values were higher in patients with complete lesions than in patients with incomplete lesions (P=0.037). No significant differences were found in other parameters (Table 2).
Age at the time of the study enrollment and age at the time of injury did not correlate with serum PSA levels and prostate volume parameters. The duration of the SCI ranged from 5 to 55 years (median 32) and did not show a correlation with TPV (r=0.063, P=0.736), TZV (r=0.072, P=0.702), TZI (r=−0.035, P=0.853), serum PSA levels (r=−0.029, P=0.877), PSAD (r=−0.063, P=0.737) or PSAT (r=0.036, P=0.849) (Table 3).
Of the 31 patients, 20 were evaluated for hormone levels. Median (5th–95th percentiles) total testosterone, LH and FSH levels were 3.58 ng/ml (1.33–7.99; normal range 2.8–8), 8.71 mIU/ml (2.13–39.01; normal range 1.7–8.6 mIU/ml) and 11.39 mIU/ml (2.26–34.37; normal range 1.5–12.4), respectively. Testosterone levels were lower than the normal range in seven patients (35%), whereas LH was higher than the normal range in 10 patients (20%), and FSH was higher than the normal range in eight patients (40%). In fact, we found an age-related increase in FSH (r=0.634, P=0.004) and testosterone was correlated inversely with TZI (r=−0.477, P=0.029). There were no significant correlations among any other parameters (Table 3).
Discussion
The prostate is innervated by branches of the pelvic ganglia, which is composed of pelvic and hypogastric nerves.11 In experimental animals, denervation of the prostate gland results in alterations of growth, cellular morphology and function.12, 13, 14, 15, 16 Thus, SCI may result in the neuropathic dysfunction of pelvic organs, including the prostate. The prostates of rats with SCI were smaller than the prostates of sham-operated control animals.17, 18 These results demonstrate the importance of normal innervation for the maintenance of the structural and functional integrity of the prostate.
Interruption of the neurohormonal supply to the prostate gland might lead to atrophy. However, contrary to animal experiments, human studies assessing prostate volume10, 19, 20and serum PSA levels8, 10, 19, 20, 21, 22, 23in men with SCI have reported conflicting results. In a study by Pannek et al.,20 even though a trend toward a lower TPV in SCI patients was found, the authors found no statistically significant difference in TPVs in any age group when they compared the SCI and uninjured groups. Lynne et al.8 found that serum PSA concentrations were higher in SCI men than in uninjured men and suggested that prostatic secretory dysfunction is present in men with SCI. Furthermore, a study by Pannek et al.20 found a trend toward lower serum PSA levels in patients with SCI. However, subsequent studies have found no statistically significant differences in serum PSA values between the SCI group and the non-SCI control group.8, 21, 22, 23 Indeed, we also found that serum PSA levels and prostate volume parameters were not significantly different in SCI men compared to those in the uninjured men. Variation in serum PSA levels among studies may be attributed to asymptomatic urinary tract infections in patients with a neurogenic bladder. Previous observations have found that subclinical prostatitis may be correlated with high serum PSA levels,24 which may be an explanation for the different results.
Injury characteristics and corresponding neurological deficits may be important variables for prostate activity. Frisbie et al.10 reported that the size of the prostate gland was smaller in severely paralyzed than in less severely paralyzed patients. Furthermore, the PSA levels in the severely paralyzed group tended to be lower than the levels found in the less severely paralyzed group. Some studies have noted that the presence of a catheter was an independent factor that could be correlated with higher serum PSA values in severely paralyzed patients.23 Inconsistent with these observations, serum PSA levels and prostate volume parameters were not vastly related to injury characteristics in our study. Likewise, Pannek et al.20 found no significant difference in prostate size according to the completeness of the lesion, the level of the lesion, or the duration of the SCI. Most groups also have demonstrated that patient characteristics, including a history of urinary tract infection,8 a positive urine culture,21 bladder management techniques,23 the SCI levels,20, 21, 22 the lesion completeness20 or the duration of the lesion20, 22 do not influence the serum PSA values in SCI patients.
Low androgen levels are commonly observed in patients with SCI. Theoretically, the low testosterone levels typical of patients with SCI may provide some protection against prostate cancer,19, 25, 26, 27, 28 thus inducing low serum PSA levels. However, prospective cohort studies have not shown a clear association between prostate cancer risk and total testosterone or bioavailable testosterone levels in the plasma.29 In addition, the prostatic inflammation in SCI patients may actually induce these patients to have increased serum PSA levels as several studies have supported a relationship between inflammation and the development of prostate cancer.30, 31 Furthermore, Huang et al.32 reported that in SCI rats, serum testosterone returned to normal levels within 3 weeks of the SCI. Thus, additional research is needed to resolve this controversy and to clarify the underlying hormonal mechanisms involved in SCI.
Our findings should be interpreted with caution. The present study was not population-based, and thus the subjects may not be representative of the general population. Additional studies involving the general population are needed to confirm our findings. Furthermore, our study included only Korean males. Therefore, the results may not be applicable to patients of other races. Further studies in these areas are warranted. Finally, because this was a pilot investigation, the sample size was small. In our study, we observed no statistically significant difference between SCI patients and uninjured men. The lack of statistically significant differences may be a result of the relatively small number of patients (Table 4).
Conclusion
According to our results, serum PSA levels and prostate volume parameters in Korean patients with SCI are not vastly different from those in the uninjured men. In addition, prostate activity in this population is not affected by injury characteristics. Even though these results may be considered preliminary because of the small sample sizes, our findings suggest that more studies are warranted to elucidate the possible impact of neurogenic or hormonal factors in the prostate activity of SCI patients.
References
Frisbie JH, Binard J . Low prevalence of prostatic cancer among myelopathy patients. J Am Paraplegia Soc 1994; 17: 148–149.
Huang TS, Wang YH, Lee SH, Lai JS . Impaired hypothalamus-pituitary-adrenal axis in men with spinal cord injuries. Am J Phys Med Rehabil 1998; 77: 108–112.
Safarinejad MR . Level of injury and hormone profiles in spinal cord-injured men. Urology 2001; 58: 671–676.
Bauman WA, Spungen AM, Adkins RH, Kemp BJ . Metabolic and endocrine changes in persons aging with spinal cord injury. Assist Technol 1999; 11: 88–96.
Vaalasti A, Hervonen A . Autonomic innervation of the human prostate. Invest Urol 1980; 17: 293–297.
McVary KT, McKenna KE, Lee C . Prostate innervation. Prostate 1998; 8 (suppl): 2–13.
Frisbie JH . Cancer of the prostate in myelopathy patients: lower risk with higher levels of paralysis. J Spinal Cord Med 2001; 24: 92–94.
Lynne CM, Aballa TC, Wang TJ, Rittenhouse HG, Ferrell SM, Brackett NL . Serum and semen prostate specific antigen concentrations are different in young spinal cord injured men compared to normal controls. J Urol 1999; 162: 89–91.
Shortliffe LMD, Sellers RG, Schachter J . The characterization of nonbacterial prostatites: search for an etiology. J Urol 1992; 148: 1461–1466.
Frisbie JH, Kumar S, Aguilera EJ, Yalla S . Prostate atrophy and spinal cord lesions. Spinal Cord 2006; 44: 24–27.
Vaalasti A, Hervonen A . Innervation of the ventral prostate of the rat. Am J Anat 1979; 154: 231–243.
Farnsworth WE, Lawrence MH . Regulation of prostate secretion in the rat. Proc Soc Exp Biol Med 1965; 119: 373–376.
Wang JM, McKenna KE, Lee C . Determination of prostatic secretion in rats: effect of neurotransmitters and testosterone. Prostate 1991; 18: 289–301.
Martinez-Pineiro L, Dahiya R, Tanagho EA, Schmidt RA . Pelvic plexus denervation in rats causes morphologic and functional changes of the prostate. J Urol 1993; 150: 215–218.
Wang JM, McKenna KE, McVary KT, Lee C . Requirement of innervation for maintenance of structural and functional integrity in the rat prostate. Biol Reprod 1991; 44: 1171–1176.
Doggweiler R, Zermann DH, Ishigooka M, Schmidt RA . Botoxinduced prostatic involution. Prostate 1998; 37: 44–50.
Linsenmeyer TA, Pogach LM, Ottenweller JE, Huang HF . Spermatogenesis and the pituitary-testicular hormone axis in rats during the acute phase of spinal cord injury. J Urol 1994; 152: 1302–1307.
Huang HF, Pogach LM, Nathan E, Giglio W, Seebode JJ . Synergistic effects of follicle-stimulating hormone and testosterone on the maintenance of spermiogenesis in hypophysectomized rats: relationship with the androgen-binding protein status. Endocrinology 1991; 128: 3152–3161.
Benaim EA, Montoya JD, Saboorian MH, Litwiller S, Roehrborn CG . Characterization of prostate size, PSA and endocrine profiles in patients with spinal cord injuries. Prostate Cancer Prostatic Dis 1998; 1: 250–255.
Pannek J, Berges RR, Cubick G, Meindl R, Senge T . Prostate size and PSA serum levels in male patients with spinal cord injury. Urology 2003; 62: 845–848.
Konety BR, Nguyen TT, Brenes G, Lewis N, Saul M, Nelson JB et al. Evaluation of the effect of spinal cord injury on serum PSA levels. Urology 2000; 56: 82–86.
Alexandrino AP, Rodrigues MA, Matsuo T . Evaluation of serum and seminal levels of prostate specific antigen in men with spinal cord injury. J Urol 2004; 171: 2230–2232.
Pramudji CK, Mutchnik SE, DeConcini D, Boone TB . Prostate cancer screening with prostate specific antigen in spinal cord injured men. J Urol 2002; 167: 1303–1305.
Hasui Y, Marutsuka K, Asada Y, Ide H, Nishi S, Osada Y . Relationship between serum prostate specific antigen and histological prostatitis in patients with benign prostatic hyperplasia. Prostate 1994; 25: 91–96.
Ito TY, Mehta M . Adenocarcinoma of the prostate in paraplegics. Paraplegia 1976; 14: 101–104.
Huang TS, Wang YH, Lee SH, Lai JS . Impaired hypothalamuspituitary-adrenal axis in men with spinal cord injuries. Am J Phy Med Rehabil 1998; 77: 108–112.
Safarinejad MR . Level of injury and hormone profiles in spinal cord-injured men. Urology 2001; 58: 671–676.
Bauman WA, Spungen AM, Adkins RH, Kemp BJ . Metabolic and endocrine changes in persons aging with spinal cord injury. Assist Technol 1999; 11: 88–96.
Raynaud JP . Prostate cancer risk in testosterone-treated men. J Steroid Biochem Mol Biol 2006; 102: 216–261.
Wilson DW, Harper ME, Jensen HM, Ikeda RM, Richards G, Peeling WB et al. A prognostic index for the clinical management of patients with advanced prostatic cancer: a British Prostate Study Group investigation. Prostate 1985; 7: 131–141.
De Marzo AM, Marchi VL, Epstein JI, Nelson WG . Proliferative inflammatory atrophy of the prostate: implications for prostatic carcinogenesis. Am J Pathol 1992; 155: 1985–1992.
Huang HF, Li MT, Linsenmeyer TA, Ottenweller JE, Pogach LM, Irwin RJ . The effects of spinal cord injury on the status of messenger ribonucleic acid for TRPM 2 and androgen receptor in the prostate of the rat. J Androl 1997; 18: 250–256.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shim, H., Kim, Y., Jung, T. et al. Prostate-specific antigen and prostate volume in Korean men with spinal cord injury: a case–control study. Spinal Cord 46, 11–15 (2008). https://doi.org/10.1038/sj.sc.3102051
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102051
Keywords
This article is cited by
-
An evidence-based review of aging of the body systems following spinal cord injury
Spinal Cord (2011)
-
Effects of stress on male voiding function
Current Bladder Dysfunction Reports (2009)
-
Statistics and the prostate gland
Spinal Cord (2008)
