
Abstract
Study design:
Case report and literature review.
Setting:
Outpatient review in the UK on a young male from the USA.
Objectives:
To report on a healthy young male who developed an incomplete paraplegia following flexion of the cervical spine after surgery to relieve tracheal stenosis.
Conclusion:
Spinal cord injury following prolonged flexion of the cervical spine after surgery to relieve tracheal stenosis can cause paraplegia. The postulated mechanism is traction upon the thoracic cord.
Similar content being viewed by others


Introduction
Paraplegia after tracheal resection is a rare but recognised complication of this procedure. This study presents such a case, reviews the literature and discusses the possible mechanism of its causation.
Case report
An American male was born on 18 February 1982 with tracheal stenosis. An immediate tracheostomy was performed. Despite a series of operations this persisted. During adolescence, he was breathless when participating in sport and had difficulty in playing the clarinet. A tracheal resection was carried out on 19 May 1999. There was minimal blood loss and he was not shocked. At the end of the operation, to relieve the tension on the tracheal suture line, his neck was flexed and his chin was sutured to his chest. He was maintained under anaesthesia for 2 days. When he recovered from the anaesthetic he was found to be paraplegic, incontinent, wheelchair bound, totally helpless. There was no recovery. He was discharged from hospital.
There was some weakness of his left upper limb and virtually no power in his lower limbs, which were spastic. He had dense sensory impairment below D8.
An MRI was carried out on 23 June 1999 with gandolinium enhancement.
There was a small annular disc prolapse at C6–7. Normal spine from T1 to T12. No significant abnormality detected. No enhancement after the gadolinium administration.
He was referred to a national centre. There had been improvement in his upper limbs, which were normal in power. The paraplegia persisted.
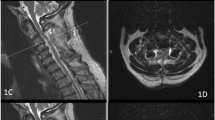
A further MRI was performed on 30 August 2001 (see Figures 1 and 2).

This is a T2 weighted sagittal image of the thoracic spine. The spinal cord is normal. There is no narrowing of the spinal canal. Note the Scheuermann's disease, which is well removed from the area of cord damage and there is no evidence of cord compression

This is T1 weighted sagittal image of the whole spine. The minimal cervical disc is so small as not to be visible. There is no narrowing of the cervical canal and no evidence of damage within the canal. The Scheuermann's disease can be seen well removed from the area of cord damage and none of the images show any evidence of cord damage
This was unchanged. There was a single small white matter lesion in the mid-ventral thoracic region.
The diagnosis was a vascular myelopathy. He was examined in the UK on the 8 February 2005.
There was still a little clumsiness in his left upper limb. The lower limbs were spastic with pyramidal distribution of weakness. The reflexes were pathologically increased with an extensor plantar response on the right. There was no sensory change in the upper limbs, he had an incomplete sensory loss below D5.
The X-rays were reviewed. Additionally, he had extensive Scheuermann's Disease on the thoraco-lumbar spine but it was not impinging upon the spinal cord.
Discussion
Infarction of the cord was discounted. He was not hypotensive throughout the operation, he was young, there was no evidence of vascular disease elsewhere in his body, and there was no evidence of cerebral involvement or of any other organs being involved. This bore no resemblance to previous cases of cord infarction described in the literature.1, 2, 3, 4
Injury to the spinal cord without bony injury is well recognised. Usually it is an extension injury in an elderly person with pre-existing cervical spondylosis. Acute flexion of the head can produce damage by a transient dislocation of the vertebrae but this is of acute onset and the major neurological damage falls on the cervical cord. In his case, the damage was on the mid-thoracic spine.
As time passes, further manifestations of vertebral misalignment or fusion become apparent. Repeat studies of his spine have been normal.
In children there can be undue hyper mobility of the spine and this can be the cause of SCIRA (spinal cord injury without bony damage). However in these cases, the damage to the cord is closely related to the site of the injury. The cervical spine was flexed and the left hand was involved at the outset, but the predominant damage fell on the mid-thoracic cord.
Scheuermann's disease is visible on the X-ray. Paraplegia only results in extreme cases where there is kyphosis and the cord is stretched across the kyphos. In his case, the Scheuermann's disease was not distorting the cord.
There had been previous reports: Borrelly et al5 described a patient who had a tumour obstructing 4/5th of the tracheal space. A tracheal resection was performed and the neck was maintained in flexion by means of a steel line postoperatively. The patient presented postoperatively with paraplegia. These symptoms disappeared spontaneously within 48 h. Subsequently, a further operation resulted in a further episode of paraplegia, which regressed when the patient removed the neck brace.
Levy et al6 described a 48-year-old man who developed paraplegia following an attack by bandits. His hands were tied behind his back and he was placed into a position of extreme flexion with his head forced down between his knees. He was bound in this position for 12 h, but for the first 2 or 3 h struggled repeatedly to release himself. When finally freed, he was aware only of generalised stiffness and was carried to bed. On awakening, he noted a dull headache and marked weakness and numbness of both arms. These problems did not abate, he had an incomplete tetraplegia. There was no blood loss and there was no shock.
Pitz et al7 also described tetraplegia after a tracheal resection procedure.
The spinal cord damage, which the boy sustained, can be directly related to the manipulation of his spinal column. There was no previous history of spinal cord involvement. There was no obvious narrowing of the spinal canal or protrusion of the cervical disc.
In the cases described,5, 6, 7 the paralysis was related to flexion of the spine. The boy was anaesthetised, it is impossible to tell whether the paralysis came on immediately or if several hours of flexion were necessary to produce the paralysis.8, 9, 10
The mechanism of injury in this and the cases in the literature is believed to be traction upon the cord. Traction can produce damage to the axons, which has been documented by Brieg.11
It is hoped that dangers of this manoeuvre will be recognised and appropriate precautions taken.
References
Silver JR, Buxton PH . Spinal stroke. Brain 1974; 97: 539–550.
Jamous MA, Silver JR, Baker JHF . Paraplegia and traumatic rupture of the aorta: a disease process or surgical complication? Injury 1992; 23: 475–478.
Singh U, Silver JR, Welply NC . Hypotensive infarction of the spinal cord. Paraplegia 1994; 32: 314–322.
Silver JR . History of infarction of the spinal cord. J History Neurosci 2003; 12: 144–153.
Borrelly J et al. Paraplegies régressives après résection iterative de la trachée. Annales de chirurgie 1981; 35: 618–619 (and translation).
Levy LM . An unusual case of flexion injury of the cervical spine. Surg Neurol 1982; 17: 255–259.
Pitz M et al. Tetraplegia after a tracheal resection procedure. Chest 1994; 106: 1264–1265.
Wilder B . Hypothesis: The etiology of midcervical quadriplegia after operation with the patient in the sitting position. Neurosurgery 1982; 11: 530–531.
Dominguez J et al. Irreversible tetraplegia after tracheal resection. Ann Thorac Surg 1996; 62: 280–283.
Hitselberger WE et al. A warning regarding the sitting position for acoustic tumor surgery. Arch Otolaryngol 1980; 106: 69.
Brieg A . Adverse Mechanical tension in the Central Nervous System. John Wiley & Sons, Biomechanics of the pons-cord tissue tract, 1977 pp 15–36.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Silver, J. Paraplegia as a result of tracheal resection in a 17-year-old male. Spinal Cord 45, 576–578 (2007). https://doi.org/10.1038/sj.sc.3101985
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101985
Keywords
This article is cited by
-
Is the outcome in acute spinal cord ischaemia different from that in traumatic spinal cord injury? A cross-sectional analysis of the neurological and functional outcome in a cohort of 93 paraplegics
Spinal Cord (2011)
-
Paralysis as a result of traction for the treatment of scoliosis: a forgotten lesson from history
Spinal Cord (2009)
