
Abstract
Study design:
Retrospective analysis of in-patient stay and prospective follow-up.
Objectives:
To study neurological and functional outcomes after traumatic central cord syndrome (TCCS).
Setting:
Regional Spinal Unit of Florence, Italy.
Methods:
In total, 82 patients, admitted for acute rehabilitation to our Centre (1996–2002) with a diagnosis of TCCS entered the study. Data on admission and discharge were collected for assessments performed at 18 months of injury or later. Data included: cause of injury, gender, type of vertebral lesion, treatment, time of hospitalisation (LoS), ASIA/ISCOS Impairment Scale, neurological examination, functional independence measure (FIM) on admission and discharge. Additional measures included the walking index for spinal cord injuries (WISCI), bladder management, FIM, spasticity on discharge/follow-up and neuropathic pain at follow-up. Correlations were performed on outcome measures in relation to age, treatment, LoS, spasticity and neuropathic pain.
Results:
Average age was 52 (16–82) years. Causes included falls (47%), road traffic accidents (36%) and sport (7%). Of patients, 45% were treated surgically and 55% conservatively. LoS was 120 days (24–390), but less for those treated without surgery. Patients under 65 years had better outcomes with less neuropathic pain. Neurological and functional recovery was observed on discharge from rehabilitation, which continued in the period following discharge. Spasticity was equally present in all age groups. No difference in outcome was found as a result of spine surgery.
Conclusions:
Patients with TCCS are older than other spinal cord injured patients, but often show improvement after discharge. Improvement in subjects under 65 years was significantly better than for those over 65 years.
Similar content being viewed by others


Introduction
Central cord syndrome (CCS) is characterised by motor weakness greater in the upper extremities than in the lower limbs and is associated with sacral sparing. This incomplete spinal cord lesion applies almost exclusively to the cervical spine trauma generally following a hypertension injury in elderly patients, with pre-existing cervical spondylosis. The presumed mechanism of injury is pinching of the spinal cord between a thickened ligamentum flavum and an anterior osteophyte or an intervertebral disc.1 Schneider et al1 in the original description of CCS, attributed the clinical features to damaged central grey matter and to lamination of the fibres of the corticospinal tract. The cervical fibres are assumed to be located more centrally than the thoracic, lumbar and sacral ones.
Nowadays both the lamination of the corticospinal fibres in humans and the necrosis of the central grey matter as the principle pathological feature of the centromedullary syndrome, have been questioned by several authors.2, 3 Levi et al2 at magnetic resonance imaging (MRI) and autopsy findings, failed to find haemorrhagic necrosis of the central grey matter and demonstrated disruption of the axons in the lateral white matter instead. This study has been confirmed by Martin et al:13 the damage of the spinal cord seems to be located in the white matter, mainly in the corticospinal tract bilaterally, moderately in the dorsal and ventral white columns and not exclusively in the central grey matter. As stated by Collignon et al3 ‘the possible explanation of the greater arm and hand dysfunction could be due to the fact that the role of the corticospinal tract in humans may be more important for hand and arm function than for lower extremity use’. Owing to changes in our understanding of pathophysiology, it is important to examine long-term functional outcomes. Recovery of a certain degree of ambulation, activities of daily life (ADL), bowel and bladder function is initially reported as favourable. Patients younger than 50 years of age at the time of injury have been reported to have a better neurological outcome in comparison to older ones. In particular, independent ambulation was achieved in 87–97% in younger patients compared to 31–41% in the elderly (over 50 years of age at the time of injury).5, 6, 7 With regards to independent bladder function the differences are similar (84 versus 29%),8 when younger are compared to older patients. Newey et al,4 in a study concerning 32 patients affected by traumatic central cord syndrome (TCCS) who were treated conservatively for their vertebral lesion, found that patients over 70 had a particularly bad outcomes both at discharge from hospital and at follow-up (mean 8.6 years) with regard to motor and bladder function, whereas spasticity did not cause significant problems. In all, 77% of those patients between 50 and 70 years of age at the time of injury could walk independently. Very little has been reported, however, in follow-up longer than 1 year. The purpose of our study, therefore, is to examine neurological and functional outcomes.
Subjects and methods
In total, 87 subjects admitted since the acute stage with the diagnosis of TCCS to our Spinal Unit from January 1996 to June 2002 were studied by retrospective data obtained from our electronic database and by a follow-up visit in our outpatient clinic (prospective data). The outpatient clinic assessment on all subjects was performed in the year 2004, at least 18 months (mean 34 months) following discharge from the hospital. Subjects were excluded if they (1) died before follow-up evaluation, (2) had missing data, or (3) were unable to be assessed by FIM/WISCI because of conditions such as mental illness and/or orthopaedic extremity impairment. Of all, five patients were excluded according to the above-mentioned criteria and 82 patients entered in our study.
The following data were collected for all subjects: year of injury, gender, age at the time of injury, cause of injury, associated injuries, vertebral lesion (level and type), treatment of vertebral lesion (conservative or surgical), length of staying in our Centre (LoS), complications during acute rehabilitation, ASIA/ISCOS severity score (A, B, C, D, E) and FIM (functional independence measure) on admission discharge and at follow-up, WISCI (walking index for spinal cord injuries) on discharge from hospital and at follow-up, the presence of neuropathic pain and spasticity at follow-up. Types of bladder and bowel management were studied on discharge from hospital and at follow-up. The assessments of patients were performed by experienced doctors in spinal cord injury.
The causes of injury were divided into three groups: (1) falls, (2) road traffic accident and (3) sports injuries. The types of vertebral injuries were classified according to X-rays and imaging (TC and MRI) as: (1) SCIWORET (Spinal Cord Injury Without Evidence of Trauma), (2) fracture, (3) fracture/dislocation and (4) pure dislocation. The treatment of the vertebral lesion was classified as conservative or surgical. Neurological evaluation was performed according to the American Spinal Cord Injury Association (ASIA) – International Spinal Cord Society (ISCoS) Standards including right and left motor and sensory levels and motor score (0–100).9 The activities of daily living were measured by the FIM scale (score range 18–126).9 We measured the ability to walk by using the WISCI (walking index for spinal cord injury) scale (score range 0–20). The WISCI is new 0–20 level scale, which evaluates walking based on physical assistance, the need of braces and devices. The levels are scored from 0 (unable to walk) to 20 (walking without braces devices or physical assistance at least 10 m).10, 11, 12 We divided the patients in three groups for purposes of analysis according to the WISCI scores:
-
Group 1 (score range 0–2): almost impossible to walk;
-
Group 2 (score range 3–17): walk with different degrees of help and Group 3 (score range 18–20): able to walk independently.
When pain was present it was classified as neuropathic if it presented with symptoms of burning or shooting into the area with sensory disturbances to pinprick and touch and without relation to movements or signs of inflammation. The pain described could be spontaneous or provoked by touch or cold, continuous, and/or with paroxysmal components.
We used the modified Ashworth scale (0–5)14 to assess spasticity, considering spastic those patients whose Ashworth score was more than 2.
Bladder management were divided into two groups: (1) spontaneous voiding, (2) no spontaneous voiding: (a) indwelling catheter (b) intermittent catheter, (c) reflex voiding.
The patients were divided into the following four groups according to age at the time of injury: 1=0–30 years (n=9), 2=31–50 years (n=26), 3=51–65 years (n=25) and 4=over 65 years (n=22).
Statistical analysis
Categorical variables (presented as absolute values and percentages) were compared by χ2 test. The differences of FIM and WISCI scores across the clinical-demographic explanatory variables were assessed through the one-way analysis of variance and the corresponding F-statistic. Statistical significance was defined as P<0.05.
Results
Demographic characteristics
The sample consisted of 72 male (88%) and 10 female subjects (12%) with a mean age of 52 years that ranged from 16 to 82 years. The causes of injury were due to road traffic accident in 47 cases (57%), falls in 30 (36%) and sport-related accidents in five cases (7%). The mean age for falls was 58 (range 27–82) years, for road traffic accidents it was 50 (range 19–71) years and for sport-related accidents it was 23 (range 16–44) years (Figure 1).

Main causes of CCS distributed in different age groups
More than half of the subjects, 44/82 (53%), had associated injuries and the most common was traumatic brain injury (TBI) in 28/44 (64%), followed by fractures in 12/44 (27%). Complications occurred in 23/82 (28%) patients and they included deep vein thrombosis (DVT) in 6/23 (26%), respiratory problems in 7/23 (30%), cardiac arrhythmias in 3/23 (13%) and pyelonephritis, gastric ulcer or pressure sores in 5/23 (22%).
Of the 82 patients, 48 (58%) sustained hyperextension injury without evidence of fractures/dislocation (SCIWORET) by imaging/X-ray, but showed evidence of canal stenosis (considered if the diameter was less than 13 mm) due to degenerative spondylosis or congenital factors.
Fracture of the spine occurred in 21/82 (26%), fracture-dislocation in 11 (13%), or pure dislocations in two (3%) patients. Mean age for patients without any radiological evidence of fracture and/or dislocation was higher, (56 years, range 22–81 years) than for those with fracture/dislocation (44 years of age, range 16–71 years).
Management of vertebral lesions (surgical versus conservative) and LoS (Figure 2)

LoS in hospital for different age classes and for surgically and conservatively treated: surgical=155 days; conservative=90 days; 0–31 years=131 days; 31–50 years=140 days; 51–65 years=119 days; 66–82 years=87 days
All 38 (45%) patients who were surgically treated, underwent anterior decompression and fusion. In cases of acute disc herniation with encroachment of the spinal canal or compression of the spinal cord and in cases of pure dislocation, the patients underwent discectomy and autograft with tricortical iliac bone fixed by plate and screws. Those patients who had either fracture or fracture/dislocation underwent corpectomy, bone autograft and fixation by plate.
Of the 44 (55%) patients treated conservatively, all patients suffered from hyperextension trauma in a stenotic cervical spine without acute protrusion of disc material compressing the spinal cord. All of these patients were immobilised by using a rigid collar (Philadelphia or Miami J).
The mean LoS was 120 days (range 24–390 days) for all 82 patients, but it was longer for surgically treated patients than conservatively treated ones (155 versus 90 days) due to the fact that those patients who had surgical treatment had worse vertebral conditions following trauma. Patients in age Group 2 (31–50 years of age at time of injury) had the longest hospitalisation (average 140 days), while patients aged 66 years or more at time of injury had a shorter stay in hospital (average 87 days) as shown in Figure 2, because older patients were usually sent to other rehabilitation Centres to continue the treatment as in-patients, and then early transferred, while the younger ones were usually discharged at home to continue rehabilitation in outpatient clinics.
ASIA impairment scale, neurological level and FIM/WISCI assessments
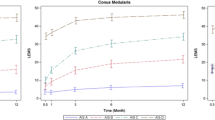
On admission, two patients were classified as ASIA A, 12 as ASIA B, 37 as ASIA C and 31 as ASIA D. On discharge no patient was classified as ASIA A or B, while eleven scored ASIA C, seventy ASIA D and one was ASIA E. At follow-up eight patients, who were discharged as ASIA D, became ASIA E (Table 1). The C6 level was found to be the most common neurological level on admission, discharge and at follow-up. The mean WISCI score on discharge was 11, while at follow-up it was 16. The FIM score increased during the same period. For FIM and WISCI scores in the different age groups on admission, discharge and at follow-up, see Figures 3 and 4.

Distribution of FIM scores on admission, discharge and follow-up

Distribution of WISCI scores at discharge and follow-up
Neuropathic pain at follow-up was recorded in 39 patients (47%)
Patients at age 50 or more at the time of the lesion had more frequent pain than patients under 50 years of age. For neuropathic pain in the different age groups, see Figure 5. Spasticity at follow-up was present in 54 patients (66%). Of these patients, 39 (72%) claimed their spasticity to be a serious problem in their activities of daily living. Spontaneous voiding with emptying of the bladder was achieved in 45 patients (55%) on discharge, which increased to 68% at follow-up.

Percentage of patients suffering from neuropathic pain at follow-up, in different age groups
The age of the subjects was compared to complications during hospitalisation, neurological improvement, FIM and WISCI assessments, neuropathic pain, spasticity and bladder emptying.
There was no significant difference between the group of patients aged less than 65 years, while patients over 65 years had more respiratory complications.
A highly significant correlation was found between age and neurological improvement (P<0.01): neurological improvement according to the ASIA impairment scale, both from admission to discharge and from discharge to follow-up, was higher for younger age groups. Even the age group from 51 to 65 years resulted in good neurological improvement, while the oldest age group (over 65 years) had the worst statistically significant neurological outcome.
FIM and WISCI scores highly correlated with the younger to older age groups (P<0.001). The oldest age group (over 65 years) had the worst FIM and WISCI scores on discharge and at follow-up. At follow-up 44/60 patients (73%) aged 50 years or under could walk without devices as compared to the oldest patient group (over 65 years), where only 50% (11/22) could walk without devices.
No statistical correlation has been found between age and the presence of spasticity, while neuropathic pain was mainly present in people over 65 years, which interfered with their quality of life. The type of bladder management was not influenced by age or gender.
Comparisons were also made between FIM/WISCI assessments and neuropathic pain, spasticity, spontaneous bladder emptying and surgical/conservative management of vertebral lesions. It was found that patients with moderate or severe spasticity had statistically significant lower FIM and WISCI scores (P<0.05) than patients without spasticity, both on discharge and at follow-up. We found no difference in FIM and WISCI scores, however, between patients affected by neuropathic pain (mean WISCI score=15.5; mean FIM score 105) and patients without neuropathic pain (mean WISCI score=16; mean FIM score 110).
The ability to spontaneously empty the bladder was not influenced by age or sex, but it was correlated with the FIM score, and was almost always managed by catheterisation when FIM score was less than 80. Spontaneous voiding was present in 64% of cases with FIM over 81. Those patients with ASIA grade C on discharge never had a spontaneous voiding, while it was possible in 63% of those discharged as ASIA D. The same correlation was found between bladder management and WISCI score at follow-up. The voiding was spontaneous in 35% of those who had a WISCI score between 3 and 17, while it became 70% in the group between 18 and 20. Nevertheless, the improvement in bladder function in the period between discharge and follow-up was neither influenced by age or gender, nor by FIM score, ASIA grade and WISCI score.
No statistically significant difference in WISCI scores was found between groups of patients treated both conservatively or surgically. The different management of vertebral lesions, however, did not influence the functional outcome with regards to FIM.
We did not find any significant difference in FIM or WISCI scores between the different vertebral injury groups.
Discussion and conclusions
Our study confirmed that younger subjects had better neurological and walking function outcomes than older subjects as reported in other case series.4, 8 As the period of follow-up in our study was longer (18 months or longer) than most previous studies, we were able to demonstrate that walking function increased significantly during the period time between discharge and follow-up. This may become very important to those individuals, who are unable to participate in outpatient programs of continued training, because of limited access to treatment after discharge from the rehabilitation hospital.
For this reason it results to be necessary to provide a sufficiently long period of intensive rehabilitation exercises to those patients affected by motor incomplete spinal cord lesions.
Such an intensive training should continue at least for a period of 18 months after injury.
Previous studies reported neurological deterioration and poorer walking function in subjects older than 50 years, which was similar to our group of subjects 65 years of age or older. Those subjects in the group 50–65 years of age, however, performed a level of walking function measured by the WISCI comparable to the younger group of subjects under age 50 years, but it took a longer period to achieve this level. This suggests that we may need to further differentiate the prognosis for walking function based on time from discharge and more discrete age groups.
The study by Penrod et al5 speculated that older subjects may do poorer than younger subjects, because of the reported higher incidence of (1) cervical spondylosis and associated deformation of the anterior horn cells, grey matter, lateral columns, (2) ischaemia of the cord due to arteriosclerosis and (3) higher incidence of medical complications, but gave no data.
The literature reveals disagreement in regard to the effect of surgery versus conservative management of subjects with TCCS and incomplete neurological lesion. Tzu-Yung Chen et al15 found no statistical difference between patients who received surgical treatment or conservative treatment after incomplete cervical spinal cord injury but stated that surgical decompression was associated with an earlier neurological improvement, faster recovery of neurological function, earlier mobilisation, better long-term neurological outcome, shorter hospitalisation and fewer complications. Guest et al16 compared clinical outcomes in patients with TCCS who underwent early surgical treatment (<24 h) or late (>24 h) after injury and found that early surgery was safe but failed to improve motor outcome in comparison to late surgery. Chen et al15 showed better results both in motor and sensory improvement in short- and long-term following surgical decompression. Maroon et al17 recommended early surgical intervention to remove offending lesions due to bone bars and/or disc herniation. Duh et al18 reported that early decompression allows an earlier rehabilitation and prevents late neurological deterioration. In our study, we found that surgery did not influence short- or long-term results both with regard to neurological and functional outcomes. Patients treated surgically had a longer hospitalisation mostly due to the fact that surgically treated patients had a worse vertebral situation on admission.
In our study, the presence of neuropathic pain correlated to age and patients over 65 years had much more neuropathic pain, that likely highly compromises their quality of life. It is well known that age at time of injury has a great influence on the presence of neuropathic pain.19
While neuropathic pain correlated with age we did not find correlations of age with bladder function or spasticity. As reported in previous studies4, 5, 20 the outcome of bladder function in TCCS patients is better than in other incomplete cervical lesions; this event is probably correlated to a minor involvement of sacral fibres. Our study confirms that there is an improvement in bladder management both on discharge and at follow-up.6, 8, 21 We found that 55% of our patients were spontaneously able to empty their bladder on discharge, and 68% at follow-up. Furthermore, we noticed that even though in other studies bladder voiding improvement is strongly correlated to age,4, 5 our data did not confirm this. In fact, patients who had a spontaneous voiding of the bladder, were equally distributed among the different age groups. A strong correlation occurred between spontaneous bladder voiding and ASIA, FIM and WISCI scores, but, by analysing the improvement in bladder management occurring in the period from the discharge to follow-up, we did not find the same correlation.
Spasticity influenced in a significant way functional outcome, but its presence was not dependent on age at time of injury. Perkash et al22 found that 48% of the patients suffered from severe spasticity 3–6 month after their injury, while in our study 54% suffered from spasticity and 72% of these patients rated spasticity as a problem in daily life. Tow and Kong in 199820 reported that 20% of their patients needed antispasticity drugs, but the neurological recovery assessed by motor score at discharge did not differ significantly if compared to patients not affected by spasticity. According to these authors the effects of spasticity on functional outcome are likely to depend on three main reasons: (1) decreased motor control secondary to cocontraction of muscles, (2) impaired coordination and (3) excessive spasm/mass movements impairing both balance and ambulation. In our study, we found that spasticity influences in a significant way functional outcome, with regard to FIM and WISCI scores. This is in accordance with the study by Perkash22 who found that 48% of their patients failed to walk because of severe spasticity.
References
Schneider RC, Cherry G, Pantek H . The syndrome of acute central cervical spinal cord injury, with special reference to the mechanics involved in hyperextension injuries of the cervical spine. J Neurosurg 1954; 11: 546–577.
Levi AD, Tator CH, Bunge RP . Clinical syndromes associated with disproportionate weakness of the upper versus the lower extremities after cervical spinal cord injury. Neurosurgery 1996; 38: 179–183; discussion 183–185.
Collignon F, Martin D, Lenelle J, Stevenaert A . Acute traumatic central cord syndrome: magnetic resonance imaging and clinical observations. J Neurosurg 2002; 96 (Suppl 1): 29–33.
Newey ML, Sen PK, Fraser RD . The long-term outcome after central cord syndrome: a study of the natural history. J Bone Joint Surg Br 2000; 82: 851–855.
Penrod LE, Hedge SK, Ditunno Jr JF . Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehabil 1990; 71: 963–968.
Merriam WF, Taylor TK, Ruff SJ, McPhail MJ . A reappraisal of acute traumatic central cord syndrome. J Bone Joint Surg Br 1986; 68: 708–713.
Foo D, Subrahamyan TS, Rossier AB . Post-traumatic acute anterior spinal cord syndrome. Paraplegia 1981; 19: 201–205.
Roth EJ, Lawler MH, Yarkony GM . Traumatic central cord syndrome: clinical features and functional outcomes. Arch Phys Med Rehabil 1990; 71: 18–23.
Marino RJ, et al, ASIA Neurological Standards Committee 2002. International standards for neurological classification of spinal cord injury. J Spinal Cord Med 2003 Spring; 26 (Suppl 1): S50–S56.
Dobkin BH, Apple D, Barbeau H, Basso M . Methods for a randomized trial of weight supported treadmill training versus conventional training for walking during inpatient rehabilitation after incomplete traumatic spinal cord injury. Neurorehab Neural Repair 2003; 17: 153–167.
Ditunno JF et al. Walking index for spinal cord injury (WISCI): an international multicenter validity and reliability study. Spinal Cord 2000; 38: 234–243.
Morganti B, Scivoletto G, Ditunno P, Ditunno JF, Molinari M . Walking index for spinal cord injury (WISCI): criterion validation. Spinal Cord 2005; 43: 27–33.
Martin D, Schoenen J, Lenelle J, Reznik M, Moonen G . MRI-pathological correlations in acute traumatic central cord syndrome: case report. Neuroradiology 1992; 34: 262–266.
Haas BM, Bergstrom E, Jamous A, Bennie A . The inter rater reliability of the original and of the modified Ashworth scale for the assessment of spasticity in patients with spinal cord injury. Spinal Cord 1996; 34: 560–564.
Chen TY, Dickman CA, Eleraky M, Sonntag VK . The role of decompression for acute incomplete cervical spinal cord injury in cervical spondylosis. Spine 1998; 23: 2398–2403.
Guest J, Eleraky MA, Apostolides PJ, Dickman CA, Sonntag VK . Traumatic Central cord syndrome: results of surgical management. J Neurosurg 2002; 97 (Suppl 1): 25–32.
Maroon JC et al. Central cord syndrome. Clin Neurosurg 1991; 37: 612–621 Review.
Duh MS, Shepard MJ, Wilberger JE, bracken MB . The effectiveness of surgery on the treatment of acute spinal cord injury and its relation to pharmacological treatment. Neurosurgery 1994; 35: 240–248; discussion 248–249.
Werhagen L, Budh CN, Hultling C, Molander C . Neuropathic pain after traumatic spinal cord injury. Relations to gender, spinal level, completeness and age at the time of injury. Spinal Cord 2004; 42: 665–673.
Tow AM, Kong KH . Central cord syndrome: functional outcome after rehabilitation. Spinal Cord 1998; 36: 156–160.
Nath M, Wheeler Jr JS, Walter JS . Urologic aspects of traumatic central cord syndrome. J Am Paraplegia Soc 1993; 16: 160–164.
Perkash I . Management of neurogenic bladder dysfunctions following acute traumatic cervical central cord syndrome (incomplete tetraplegia). Paraplegia 1977; 15: 21–37.
Acknowledgements
We would like to thank John F Ditunno for his contribution in revising the manuscript and for his precious advises. This is a spontaneous research, not funded or financed by any institution or private company.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Aito, S., D'Andrea, M., Werhagen, L. et al. Neurological and functional outcome in traumatic central cord syndrome. Spinal Cord 45, 292–297 (2007). https://doi.org/10.1038/sj.sc.3101944
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101944
Keywords
This article is cited by
-
Timing of decompression in central cord syndrome: a systematic review and meta-analysis
European Spine Journal (2024)
-
Central cord syndrome definitions, variations and limitations
Spinal Cord (2023)
-
Treatment of acute traumatic central cord syndrome: a score-based approach based on the literature
European Spine Journal (2023)
-
Is it time to redefine or rename the term “Central Cord Syndrome”?
Spinal Cord (2021)
-
Missed bilateral radial head fractures in central cord syndrome
Spinal Cord Series and Cases (2020)
