
Abstract
Study design:
A complex set-up was used to investigate kinematics and ground reaction forces.
Setting:
Motor Control and Physical Therapy Research Laboratory, Neurotec Department, Karolinska Institutet, Huddinge, Sweden.
Objective:
To investigate how men and women with spinal cord injury (SCI) perform transfers from table to wheelchair with regard to timing and magnitude of force generation beneath the hands and associated body movements.
Methods:
A total of 13 subjects (seven men, six women) with thoracic SCI. Kinematics of body movement were recorded (Elite 2000 system) simultaneously with the signals from three force plates (AMTI) placed beneath the buttocks and hands. Temporal and spatial parameters regarding head, trunk and trailing arm displacement, loading amplitudes and loading torque directions of both hands were analyzed for each trial and subject and compared between genders.
Results:
Men and women used similar amplitudes of head bending and forward displacement of the trailing shoulder, while female subjects had significantly larger trunk rotation. Both genders applied significantly more weight on the trailing hand. Differences between genders were seen in direction and timing of peak torque beneath the hands.
Conclusions:
The forces beneath the trailing hand were larger than those in the leading, if there is weakness or pain in one arm, this arm should be selected as the leading. To avoid excessive load on the arms, technical aids and environmental factors should be very well adapted.
Sponsorship:
This project was funded by the Swedish Research Council and the Health Care Science Committee of Karolinska Institutet.
Similar content being viewed by others

Introduction
Pain is often experienced by people with paraplegia due to spinal cord injury (SCI).1, 2, 3 The prevalence increases with the number of years from onset of SCI and with increasing age.1, 4, 5 Pain in the upper extremities is often evoked by transfers1, 6, 7, 8 and wheelchair propulsion,1, 3, 4, 7, 8 and is sometimes so severe that it disturbs sleep1, 4 and diminishes independence.1, 7, 9 Owing to increased longevity in this population,10 it is becoming increasingly important to prevent long-term musculo-skeletal morbidity related to, among other things, repetitive strain of the locomotor system.
Activities of daily living (ADL) typically become severely restricted by SCI and have to be relearned using new techniques. One such core activity is to move oneself to and from the wheelchair.11 In the early rehabilitation phase, persons with paraplegia depend on sliding boards, lifts, or assistance from another person, but independence in daily transfers is a realistic goal if the patient is given adequate rehabilitation.
Comparatively few studies on transfer technique for people with paraplegia have been performed and all are based on men.12, 13, 14 Perry et al13 studied transfers between wheelchair and table by measuring the activity of shoulder muscles by electromyography (EMG) and through clinical observations. Wang et al14 studied able-bodied subjects, with legs strapped together, during sitting transfers from chair to table at different heights while measuring EMG and reaction forces beneath the leading arm. However, able-bodied subjects with strapped legs are hardly suited for drawing conclusions as regards paraplegic wheelchair users. Allison et al12 recorded kinematic and kinetic data of a long-sitting transfer on a table. Kinetic and kinematic techniques have also been used while studying postural stability15 and wheelchair propulsion16 for this population. No study has been performed with simultaneous registration of kinetics and kinematics during a transfer between wheelchair and table with a height difference. This type of transfer is frequently used in daily life situations where height differences are common.
The population of SCI subjects comprises 80–85% men17 making it perhaps understandable that research has essentially been based on men. In an American multicenter study of more than 1000 patients with SCI, no differences were found between men and women as regards motor function (ASIA motor score) at admission and discharge from hospital, achieved functional independence (Functional Independence Measure) or length of rehabilitation between men and women.18 Clinical experience from our SCI unit indicates that women seem to have more difficulties than men in achieving independence in transfers. Men seem to perform the transfers in a smoother way and to be able to manage more complicated transfers such as getting up from the floor.
The objective of this study was to investigate how subjects with SCI perform transfers from table to wheelchair as regards timing and magnitude of the force generation beneath the hands as well as that of associated body movements, and to investigate whether transfer parameters differed between men and women.
Materials and methods
Subjects
From a regional database comprising 90% of all patients with SCI in the Stockholm region (1036 persons, 701 men and 335 women) a search was performed including men and women with SCI level T1–T6, ASIA A.19 Subjects with congenital lesions, unstable medical condition (eg cardiac diseases, infections, pressure ulcers), and subjects unable to perform independent transfers were excluded. Phone contact was made with potential subjects, including confirmation and specification of criteria (eg ability to perform the transfer with a height difference of 10 cm up to the wheelchair, without the presence of ulcers). Inclusion criteria were adjusted post hoc to also include SCI levels T7–T10 as well as ASIA B, since not enough women were found using the primary criteria. A total of 17 subjects (eight men, nine women) were willing to participate in the study. Four of those were unable to complete the study due to illness etc. Subjects' characteristics are presented in Table 1.
None of the subjects presented had a decreased range of joint motion severe enough to influence the transfer strategy. Three subjects reported being troubled by spasticity during daily transfers (S 8, 9, 10). Eight subjects reported being able to perform independent transfers from floor to the wheelchair (S 1, 2, 3, 5, 7, 8, 9, 11). Six subjects (S 2, 3, 4, 7, 10, 12) reported pain. The highest estimated score on the Borg CR-1020 was 3, corresponding to ‘moderate pain’. This study was approved by the local ethics committee of Karolinska University Hospital, Stockholm.
Experimental set-up and task
The set-up model is shown in Figure 1. Two force plates were placed on the table and the third was placed at the border on the other side of the wheelchair and levelled to the seat height. The transfers were performed from sitting on a force plate placed on a height adjustable-table close to the wheelchair. All subjects used their own wheelchair and seat cushion. The height of the table was adjusted so that the top of the cushion on the wheelchair was 7 cm higher than the level of the force plate where the subject sat. The wheelchair was placed according to the subjects' preference and they could choose to transfer to the right or left side. Subjects were fitted with a protective cushion (JAY protector®) to the buttocks while performing the transfer trials.

Experimental set-up for a transfer from table to wheelchair showing three force plates: one beneath the buttocks and the other two beneath the trailing and leading hands. Arrows indicate the torque direction of vertical force (Mz) beneath the trailing and leading hands as well as the direction of the lower body transfer movement. The 3D room reference coordinates for the kinematics in this set-up are indicated. Abbreviations: SAD indicates a torque direction beneath the hand in same direction as that of the transfer, while OPD indicates the opposite direction
The starting position was sitting on one force-plate with the hands in the lap. When initiating the transfer the subjects placed their feet in a position of preference and the hands on the force plates. The subjects were instructed to start the transfer after a verbal signal, to perform it at their own pace and to place their hands on the thighs again when seated in the chair. Recording time was stopped when the subjects sat in the wheelchair with both hands in the lap. Each trial was observed by the experimenter, while an assistant stood behind the wheelchair to ensure that it would not move. All trials were observed by the same experimenter.
Three force plates were used for the recording of ground reaction forces (AMTI, Advanced Mechanical Technology Incorporation, Watertown, MA, USA; model Mc18-6-1000, size 457 × 203 mm; accuracy 0.25 N). To record the kinematics, spherical reflective markers (diameter of 10 mm) were fastened with adhesive tape to six anatomic landmarks: one on the head, bilaterally on the acromion and the head of ulna and one on the spinous process of T5. In addition, one marker was placed at the back corner of each of the three force plates to provide spatial orientation. An eight-camera opto-electronic system (Elite 2000, BTS, Milan, Italy) was used to record the transfer trials. The cameras were placed in a circle, 8 m in diameter, around the force plates. The explored field was 2 × 2 × 2 m giving an accuracy of 0.78 mm. The Elite system simultaneously recorded force plate signals and the marker positions with a sampling frequency of 100 Hz. Recording time was determined by a keyboard stroke when the subject sat in the wheelchair. Recording time varied between 6 and 40 s. Prior to the onset of the verbal instruction, baseline data were recorded for about 2 s.
Prior to the trials, the experimenter explained the study procedure, the Borg CR10 scale20 and Borg RPE scale20 to the subject. Before the first transfer, the subjects were asked about the presence and location of pain and an estimation of pain on the Borg CR10 scale. Immediately after one, five and ten transfers, respectively, the subject estimated pain on the Borg CR10 and exertion on the Borg RPE.
Data analysis
After data processing for 3D position of the markers, kinematic and force plate data were transformed into ASCII files and analyzed in Axograph (Axon Instruments), a Macintosh-based software package. Before analysis, all the signals were digitally filtered for signal smoothing.
Figure 2 shows time traces of force parameters and kinematics selected for the temporal and spatial analysis. All temporal events were defined relative to the instant when the force signal beneath the buttocks fell to zero and was termed as seat-off equal to time zero.

Time traces of a single trial of one subject illustrating the different parameters analyzed. The vertical force signals Fz (expressed in %BW) generated beneath buttocks and hands as well as the torque of vertical force Mz (expressed as %BWmm) of vertical displacement of head and anterior/posterior displacement of trailing hand and trunk rotation. Arrows indicate direction of traces moving in a positive direction. One trial for one subject illustrates the different parameters analyzed. Vertical line indicates seat-off and is defined as time zero
Vertical force application
The amplitudes of the force signals were normalized by body mass and were expressed as percentage change of body weight (%BW). The mean amplitude of loading (Fz) beneath the trailing and the leading hand was calculated from the instant the subject placed the hand on the force plate (onset of vertical force) until the hand lifted from the force plate (Figure 2). Throughout this paper the moment of vertical force (Mz) is termed torque. Peak torque amplitude, occurrence relative to seat-off, and torque direction were analyzed for the trailing and the leading hand (Figure 2). The torque direction was defined either as ‘the same direction to transfer direction’ (SAD) or ‘the opposite direction as transfer direction’ (OPD) during the transfer (Figure 1).
Trunk and head movement
Linear and angular displacements were computed as changes relative to the mean of baseline data (when the subject was sitting with his/her hands in the lap). All amplitudes were measured at seat-off (Figure 2). Head displacement (mm) was measured in the vertical direction (y). The shoulder displacement was measured as the forward displacement of the shoulder (z) at seat-off. The hand-shoulder distance (mm) in the anterior/posterior direction (z) was calculated as the distance between the displacement of the trailing shoulder and the trailing hand at seat-off. This distance corresponds to the triangular base of Bergström et al.21 Trunk segment rotation in space was defined by joining the markers on the left and right acromion versus the anterior/posterior axis (z). A positive-directed trace reflected a forward rotation of the trailing shoulder.
Owing to obscured body markers and misplacement of the hands relative to the force plates during transfers, some trials were invalidated. The invalidated trials were not systematically distributed and did not, therefore, influence the statistical analyses.
Statistics
All statistical analyses were performed in STATISTICA for Windows (StatSoft Inc., 2000). As the data were not normally distributed, nonparametric statistics were selected for analysis. For both kinetic and kinematic data the group median of the means of all trials of each subject was calculated and used for descriptive analysis (median and interquartile range). The significance level was set at P<0.05 and Wilcoxons matched pairs test was used to compare the median of dependent variables. The Mann Whitney U-test was used to compare the male female groups.
Results
Head and shoulder movement amplitudes at seat-off
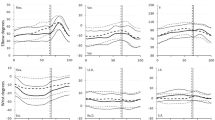
Figure 3a–d illustrates the head and shoulder movement amplitudes. The median amplitude of the head's downward bending was 255 mm for the male subjects and somewhat less (218 mm) for the women (Figure 3a). The shoulder of the trailing arm was displaced forward 265 and 238 mm, respectively (Figure 3b). The forward bending of the body increased the hand – shoulder distance of the trailing arm to 279 mm for the male and 180 mm for the female subjects (Figure 3d). None of the amplitudes of head and shoulder movements were significantly different between the male and female subjects. However, trunk rotation as reflected in the backward rotation of the trailing shoulder was significantly less marked in the male subjects (32°) as compared with that of the female subjects (41°, P=0.02, Figure 3c).

(a–d) Box and Whisker plots of group median of men (n=7) and women (n=6) of head and shoulder displacement, trunk rotation and a/p distance between hand and shoulder at the instant of seat-off. Significant group differences are marked with *(P<0.05)
Loading forces and peak torque amplitude beneath trailing and leading hand
Both male and female subjects applied significantly more weight on the trailing hand compared to that of the leading hand (P=0.017, 0.02) (Figure 4a). The median amplitude beneath the trailing hand was 32% BW for men and 27% BW for women; and 24.5 and 23% BW, respectively, beneath the leading hand. The median amplitude of weight-bearing on the trailing hand was, in the male group, significantly larger than that of the female group (P=0.045) but this was not the case regarding the leading hand. Men applied a higher median peak torque amplitude in both the trailing (446.7% BWmm) and leading (491.5% BWmm) hands compared to the women (332.4% BWmm, 449.6% BWmm) but the differences were not statistically significant (Figure 4b).

Box and Whisker plots of group median of the mean amplitude of individual means of loading on the trailing and leading hand (a) and peak torque amplitude (b)
Direction and timing of peak torque amplitude beneath the trailing and the leading hand
There were four possible strategies of coordination regarding torque direction between the trailing and the leading hand. Men applied an OPD torque in the trailing hand and a SAD torque in the leading hand in 67% of the trials, while the women applied that pattern in 30% of the trials. In 46% of the trials the women applied the torque in the OPD in both hands and this pattern was observed in 15% of the trials for the men. The other two strategies of torque direction in the hands were SAD in the trailing hand and OPD in the leading hand (men 11%, women 16%), and SAD in both hands (men 7%, women 8%).
Regarding the timing of the peak torque, the women showed a striking pattern, since peak torque occurred after seat-off in both hands in 81% of the trials, for men in 31% (Figure 5). In 52% of the trials, the men applied the peak torque before seat-off in the trailing hand and after seat-off in the leading hand, which was true even for 14% of the trials involving the women. The other strategies of timing were less frequently used.

Time of peak torque relative to seat-off in trailing and leading hand are presented for all subjects and trials
Clinical measurements
The lowest estimated exertion score on Borg RPE after 10 trials was 7, which corresponds to ‘extremely light 7–8’, and the highest estimated score here was 13, which corresponds to a ‘somewhat hard’ exertion. The men rated 7–13 and women 7–12. The estimated pain score on Borg CR 10 was 0–3, where 3 corresponds to ‘moderate’ pain. The men rated 0–3, and women 0–2.5. None of the subjects interrupted the trials because of pain.
Discussion
The model set-up of the subjects: sitting on a force plate on a table, was chosen to make it possible to register seat-off. When comparing the results with those of Perry et al13 the preparation of the transfer was similar, starting with a weight shift from the buttocks to the hands by trunk flexion and trunk rotation towards the trailing side. These two studies complement each other by measuring the same type of transfer using different methods. In other studies,12, 14 the methods differed too much to make a comparison possible.
Allison et al12 used a two-camera system to record kinematics from the lateral and posterior view. The eight-camera ELITE-system made it possible to analyze the transfer in three dimensions. In this study, several trials were performed by each subject, which made analysis possible even though certain markers were sometimes obscured when the head was bending forward and downward. To avoid this problem in future, we suggest that additional cameras should be placed on the ceiling.
The hand–shoulder distance for the men was longer than that of the women, but not significantly so, that is, the men placed the trailing hand further back relative to the shoulder. The women, on the other hand, used a larger trunk rotation. By placing the hand further back the men seemed to use the body as a lever more efficiently. The shoulder–hand distance has been regarded as a key factor in influencing the ability to transfer oneself; here the independent subjects showed the largest distance.21 Bergström et al21 also showed that anthropometric measures such as body stature, trunk length, arm length, and bitrochanteric width did not influence the ability to transfer oneself independently, although it should be emphasized that the gender distribution in their study was three women and 33 men. Despite the small sample, we found some gender differences concerning movement strategy, suggesting that anthropometric measures may have influenced the results. Our set-up model with force plates under the hands may have influenced the normal transfer strategy, especially in those subjects with short arms or trunk length, however, the position of the force plate beneath the leading hand directly to the wheelchair was made to minimize this effect. In future studies involving both men and women, antropometric factors such as bitrochanteric width, arm, and trunk length should be taken into consideration.
All subjects applied more force beneath the trailing hand than with the leading hand, which seems like a natural strategy since the trailing hand is placed closest to the body and is therefore stronger. The mean amplitude of the vertical forces beneath the hands suggests that transfers cause substantial stress on the upper extremities, which may provoke pain. The finding that the forces beneath the trailing hand were larger than those beneath the leading hand suggests that, from a clinical point of view, if weakness or pain in one arm is present, this arm should be selected as the leading arm. Our findings regarding the force generation beneath the trailing and leading hand support the findings in the EMG-study of Perry et al13 indicating that the stress on shoulder muscles is lower in the leading arm.
The most common strategy for the men was to apply the peak torque before seat-off with OPD in the trailing hand and after seat-off with SAD in the leading hand. This means that they exerted the peak torque in the trailing hand prior to lifting of the lower body. The women timed the peak torque after seat-off in both hands and used the OPD-OPD or OPD-SAD strategy. Thus, they lifted the lower body before the torque reached its peak. The strategy used by the men suggests that they could make use of the propulsive impulse generated by the arms targeted to match the subject's weight and support surface area between the arms for the upward and transfer acceleration of the body prior to seat-off. This means that the men programmed the transfer prior to seat-off while the women adjusted the force generation beneath the arms continuously with the transfer movement. This may explain the higher values of torque production in women (Figure 4b).
All the men and two women (S 11, 13) performed the transfers smoothly and with minimal preparation, while the other women needed more time for adjustments before transferring. This may have been due to a difference in capacity of adjusting their ordinary transfer strategy in a novel environment. When analyzing the kinetic and kinematic data as well as the clinical findings, no clear similarities were found between the two women and the male group as was expected when observing the transfers. No differences were found between subjects 11 and 13 and the other women. Considering both the results of this study and clinical experience from our SCI center, the male strategy seems more efficient and flexible. The question remains whether the women have the physical prerequisites to use the same strategy as the men. In general, it is difficult to say if the transfer strategy is chosen due to physical gender differences, learned habits or personal preference.
Re-establishment of functional human movement is a key goal in rehabilitation.22 Whereas gait strategy is well studied, there is presently a lack of quantitative studies focusing on transfer techniques for wheelchair-using persons. Since this study was performed, transfer strategies have been studied by Nawoczenski et al23 (able-bodied persons moving between wheelchair and table) and Gagnon et al24 (persons with SCI performing a posterior transfer on a level surface) indicating that this is an area of current interest. Hopefully, further research will contribute to the introduction of optimal transfer techniques, allowing for the lowest possible force application and energy consumption and thereby avoiding unnecessary pain due to overextension. The goal is to obtain maximum independence.
Conclusion
As the forces beneath the trailing hand are larger than those of the leading, this should be taken into consideration when the subjects are weaker or experience pain in the arm, which should preferably be chosen as the leading arm. To avoid increased load on the trailing arm, technical aids and environmental factors should be adapted to stimulate more symmetrical weight-bearing on both arms.
References
Pentland WE, Twomey LT . Upper limb function in persons with long term paraplegia and implications for independence: Part 1. Paraplegia 1994; 32: 211–218.
Sie IH, Waters RL, Adkins RH, Gellman H . Upper extremity pain in the postrehabilitation spinal cord injured patient. Arch Phys Med Rehabil 1992; 73: 44–48.
Curtis KA, Drysdale GA, Lanza RD, Kolber M, Vitolo RS, West R . Shoulder pain in wheelchair users with tetraplegia and paraplegia. Arch Phys Med Rehabil 1999; 80: 453–457.
Gellman H, Sie I, Waters RL . Late complications of weight- bearing upper extremity in the paraplegic patient. Clin Orthop Rel Res 1988; 233: 132–135.
Ballinger DA, Rintala DH, Hart KA . The relation of shoulder pain and range of motion problems to functional limitations, disability, and perceived health of men with spinal cord injury: a multifaceted longitudinal study. Arch Phys Med Rehabil 2000; 81: 1575–1581.
Bayley JC, Cochran TP, Sledge CB . The weight- bearing shoulder: The impingement syndrome in paraplegics. J Bone Joint Surg 1987; 69: 676–678.
Dalyan M, Cardeans DD, Gerard B . Upper extremity pain after spinal cord injury. Spinal Cord 1999; 37: 191–195.
Nichols PJR, Norman PA, Ennis RJ . Wheelchair users shoulder? Shoulder pain in patients with spinal cord lesions. Scand J Rehabil Med 1979; 11: 29–32.
Rintala DH, Loubser PG, Castro J, Hart KA, Fuhrer MJ . Chronic pain in a community- based sample of men with spinal cord injury: prevalence, severity, and relationship with impairment, disability, handicap, and subjective well-being. Arch Phys Med Rehabil 1998; 79: 604–614.
Levi R, Hultling C, Nash M, Seiger Å . The Stockholm spinal cord injury study 1: medical problems in a regional SCI population. Paraplegia 1995; 33: 308–315.
Somers MF . Spinal Cord Injury Functional Rehabilitation. Upper Saddle River: Prentice Hall 2001, 169, 240.
Allison GT, Singer KP, Marshall RN . Transfer movement strategies of individuals with spinal cord injuries. Disabil Rehabil 1996; 18: 35–41.
Perry J, Gronley JK, Newsam CJ, Reyes ML, Mulroy SJ . Electromyographic analysis of shoulder muscles during depression transfers in subjects with low-level paraplegia. Arch Phys Med Rehabil 1996; 77: 350–355.
Wang Y, Kim CK, Ford HT, Ford HT . Reaction force and EMG analyses of wheelchair transfers. Percep Mot Skills 1994; 79: 763–766.
Kamper D, Parnianpour M, Barin K, Adams T, Linden M, Hemami H . Postural stability of wheelchair users exposed to sustained, external perturbations. J Rehabil Res Dev 1999; 36: 121–132.
Bednarczyk JH, Sanderson DJ . Limitations of kinematics in the assessment of wheelchair propulsion in adults and children with spinal cord injury. Phys Ther 1995; 75: 281–289.
Burney RE, Maio RF, Maynard F, Karunas R . Incidence, characteristics and outcome of spinal cord injury at trauma centers in North America. Arch Surg 1993; 128: 596–599.
Greenwald BD, Seel RT, Citu DX, Shah AN . Gender-related differences in acute rehabilitation, length of stay, charge and functional outcomes for a matched sample with spinal cord injury: a multi-center investigation. Arch Phys Med Rehabil 2001; 82: 1181–1187.
American Spinal Injury Association. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association: Chicago 1994.
Borg G . Borgs Perceived Exertion and Pain Scales. Hum Kinetics: Champaign 1998 pp 29–43.
Bergström E, Frankel H, Galer I, Haycock E, Jones P, Rose L . Physical ability in relation to anthropometric measurements in persons with complete spinal cord lesion below the sixth cervical segment. Int Rehabil Med 1985; 7: 51–55.
Durward BR, Baer GD, Rowe PJ . Functional Human Movement; Measure and Analysis. Butterworth Heinemann: Oxford 1999, pp 2–33.
Nawoczenski D et al. Three-dimensional shoulder kinematics during a pressure relief technique and wheelchair transfer. Arch Phys Med Rehabil 2003; 84: 1293–1300.
Gagnon D, Nadeau S, Gravel D, Noreau L, Larivière C, Gagnon D . Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low-level spinal cord injuries. Clin Biomech 2003; 18: 319–331.
Acknowledgements
We express our gratitude to Ingmarie Apel for technical assistance, and Lars Holmström for support. This study was supported by a Swedish Research Council grant (Hirschfeld) and an MSc grant to Granström from the Health Care Science Committee of Karolinska Institutet.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Forslund, E., Granström, A., Levi, R. et al. Transfer from table to wheelchair in men and women with spinal cord injury: coordination of body movement and arm forces. Spinal Cord 45, 41–48 (2007). https://doi.org/10.1038/sj.sc.3101935
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101935
Keywords
This article is cited by
-
Musculoskeletal Pain Due to Wheelchair Use: A Systematic Review and Meta-Analysis
Pain and Therapy (2021)
