
Abstract
Study design:
Flexion reflex study in motor complete human spinal cord injury (SCI).
Objectives:
To examine changes in the magnitude of the flexion reflex following functional electrical stimulation (FES) of the rectus femoris (RF) muscle.
Setting:
Bioengineering Unit, University of Strathclyde, Glasgow, Scotland, UK.
Methods:
The flexion reflex was evoked by electrical stimulation of the sural nerve, and was recorded in the tibialis anterior (TA) muscle. RF muscle conditioning stimulation was performed at 0.7, 1, and 2 times motor threshold ( × MT) over a range of conditioning test intervals.
Results:
The incidence of the early component of the flexion reflex (<100 ms) was low, suggesting that this reflex component might be suppressed in SCI. The long latency flexion reflex component (>120 ms) was observed in all subjects during control conditions and following sensorimotor conditioning. FES applied to the RF muscle (above and below MT) in the main induced a significant early and long lasting depression of the long latency flexion reflex.
Conclusion:
The depression of the flexion reflex was a result of multisensory actions on flexion reflex pathways resulting from the direct and indirect (mechanical) consequences of electrically induced muscle contraction on cutaneous and muscle afferents. Our findings emphasize the importance of sensory feedback mechanisms in modulating flexion reflex excitability, and highlight the need for rehabilitation professionals to consider the central actions of FES-induced afferent feedback when incorporating FES into a rehabilitation program.
Sponsorship:
State Scholarships Foundation (IKY) of Hellas.
Similar content being viewed by others

Introduction
Functional electrical stimulation (FES) can be employed to synthesize a reciprocal walking pattern in individuals with spinal cord injury (SCI). FES applied to the knee extensor muscles is utilized to provide the stance phase of a step with the swing phase being reproduced by appropriately timed generation of flexion reflexes.1, 2, 3 However, the quality of gait produced in this way is often poor due to variability and habituation in the magnitude of the evoked flexion reflex. This variability is seen functionally as loss of effective ground clearance, a stride length that reduces over time and even a complete failure to initiate swing when required.4, 5, 6, 7
While habituation in flexion reflexes may be the consequence of purely central mechanisms, a number of peripheral factors acting via afferent feedback may also contribute to the variability of flexion reflex magnitude. For example, many studies in human and reduced animal preparations have demonstrated that proprioceptive and cutaneous afferents can influence flexion reflex expression and patterned motor output during locomotion.8, 9, 10, 11, 12, 13, 14, 15, 16, 17 This raises the possibility that afferent activity induced by FES of muscle when used to generate the stance phase of gait could also influence flexion reflex pathways and indirectly influence the quality of swing achieved in FES-based walking.
In the present study, we investigated whether the magnitude of the flexion reflex is modulated following FES of the rectus femoris (RF) muscle in subjects with chronic motor complete SCI under static conditions. Our results demonstrate that FES conditioning significantly influences the magnitude of flexion reflexes. The predominant effect of FES on flexion reflexes excitability is inhibitory. This observation has implications for gait rehabilitation based on the use of FES after SCI. Preliminary accounts of this work have been published in abstract form.18, 19
Methods
Study participants
Experiments were conducted with local ethics committee approval (South Glasgow University Hospitals NHS Trust, Glasgow, UK) and the written informed consent of all volunteers prior to testing. Seven male SCI subjects with thoracic lesions ranging from T5 to T12 participated in the study. The impairment scale of the American Spinal Injury Association (ASIA)20 was employed to classify the completeness of the lesion (Table 1). Only one subject (S5) reported limited joint sensation from the digital joints of the right foot. No subject at the time of the study received antispasticity medication. All experimental tests were completed with subjects seated (hip angle 120°, knee angle 160°, and ankle angle 110°) and with their feet secured on separate footplates. Both lower limbs and feet were restrained to prevent any movement during reflex testing and FES conditioning.
Elicitation and recording of the flexion reflex
The flexion reflex was evoked by electrical stimulation of the sural nerve according to the procedures described by Roby-Brami and Bussel.22 Two disposable pre-gelled Ag/Ag–Cl electrodes (Ambu Inc., Ølstykke, Denmark) were placed over the course of the sural nerve at the lateral submalleolar region of the right leg. The reflex was evoked by a 30 ms train of 1 ms pulses delivered at 300 Hz once every 10 s (Figure 1b, lower panel). At this interval reflex habituation was not encountered.

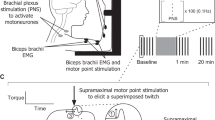
(a) The components of the flexion reflex (early and long latency; ELFR and LLFR) are indicated as full-wave rectified EMG averages of 20 responses (upper and lower trace), and are identified by vertical cursors placed at the start and at the end of the corresponding EMG. In the upper trace, EMG recordings indicate a case where both components of the flexion reflex were present, while in the lower trace EMG recordings indicate a case where only the LLFR was present. Both records are from subject 3. (b) Schematic illustration of the relationship between the timing of RF muscle and sural nerve stimulation. The top stimulus train illustrates the time course of conditioning stimulus and the bottom record shows the relative timing of sural nerve stimulation used to generate the flexion reflex (the timing intervals are not to scale). The conditioning test (C-T) represents the interval between the conditioning stimulus train and the stimulus train delivered to the sural nerve
In all experiments, the sural nerve was stimulated between 1.2 and 2 × reflex threshold. At this stimulation intensity, the reflex is submaximal but easily observable by electromyographic (EMG) recordings but does not generate gross limb movement. Surface EMG was recorded via disposable pre-gelled Ag/Ag–Cl electrodes (A-10-N, Ambu Inc., Ølstykke, Denmark) placed over the belly of the tibialis anterior (TA) muscle following light mechanical abrasion of the skin. The EMG signals were amplified (Neurolog, Digitimer Ltd, UK) and band-pass filtered (10 Hz–1 kHz) before being sampled at 2 kHz (CED 1401 and laboratory interface running Spike 2 software; Cambridge Electronics Design Ltd, Hertfordshire, UK).
In SCI subjects, the flexion reflex can show early and late components.23 The presence of reflex components at latencies less than 100 ms was considered to be representative of the early latency flexion reflex (ELFR). Reflex bursts occurring at latencies greater than 120 ms were categorized as long latency flexion reflex (LLFR) components.22 The digitized EMG signals were rectified and the size of ELFR and LLFR was quantified by measuring the area under the full-wave rectified EMG records (Figure 1a). Estimates of the mean size of the control flexion reflex and flexion reflexes conditioned by prior FES to the RF muscle were obtained by calculating the average size of the reflex from 20 individual reflexes.
FES-induced RF muscle contraction
The subjects and the protocol employed to electrically stimulate the RF muscle were identical to those reported in Knikou and Conway.24 Two circular self-adhesive electrodes (electrode type 879300R, PALS, Med-Fit Systems, Fallbrook, CA, USA) were positioned on the skin of the right leg at sites close to the motor points of the RF muscle. Using a constant current stimulator (DS7A, Digitimer, UK), single shocks (pulse width 200 μs) of increasing intensity were used to determine the motor threshold (MT) of the RF muscle. MT was defined as the stimulus intensity that evoked a motor response of the RF muscle. All subsequent conditioning stimuli were presented as trains of pulses graded to MT.
For all subjects, the conditioning RF stimulus train consisted of five pulses with an inter-pulse interval of 43 ms (23 Hz) repeated once every 10 s (Figure 1b, upper panel). This stimulation frequency is consistent with that employed in FES studies.25 In conditioning trials, three intensities of FES were employed (0.7, 1, and 2 × MT). At 2 × MT a clear isometric contraction of the RF muscle was observed.24 In all subjects, the RF conditioning stimulation preceded the test TA flexion reflex by variable delays measured from the time of the last pulse in the FES train to the first pulse in the stimulus directed to the sural nerve (Figure 1b).
In all subjects, sets of control flexion reflexes were recorded prior to and following each set of FES conditioning trials. Rest periods of 5 min were given between each set of measurements and each set of measurements were repeated on each subject. In all, 11 different conditioning test (C-T) intervals were examined when conditioning the flexion reflex by RF stimulation at 2 × MT. The C-T intervals studied ranged from 0 to 16 (incremented by 2 ms), 100, and 120 ms. The choice of short and long intervals was selected to reflect the anticipated changes in afferent feedback associated with the time course of the mechanical events generated by an FES-evoked RF contraction.24 At the lower stimulation intensities of 0.7 × MT and 1.0 × MT, the C-T intervals tested were restricted to 0, 2, and 4 ms (FES conditioning of RF at 1.0 × MT and 0.7 × MT were not performed on subject 1). As no significant evoked contraction occurred at these conditioning intensities and a mechanically induced afferent activation was not generated, no longer C-T intervals were investigated. Limitation in the time available for subject testing, also precluded longer C-T intervals being tested at these lower intensities.
Data analysis
For each subject and conditioning stimulation intensity, the conditioned ELFR and the LLFR were expressed as a percentage of the associated control flexion reflex. A one-way repeated analysis of variance (ANOVA) was applied separately to the data. When significant differences between the control and the conditioned reflexes were encountered, post hoc Bonferroni tests were performed to determine whether the modulation of the reflex varied with changes in time (across C-T intervals), using P<0.05 as the criterion of statistical significant difference.
The mean amplitude of the conditioned flexion reflex from each subject was then grouped by the C-T interval and conditioning stimulus intensity employed. A two-factor repeated measures ANOVA was performed in order to establish if changes in the amplitude of the conditioned flexion reflexes were evident with changes in the C-T interval and conditioning stimulation intensity employed. Results are presented as mean values and standard error of the mean (SEM).
Results
Under control conditions sural nerve stimulation resulted in the generation of an LLFR in all subjects. An ELFR was also evident under control conditions in one subject (S1) and following RF conditioning stimulation in additional two subjects only (S3 and S5). Example recordings of the ELFR and LLFR components are illustrated in Figure 1a. Table 2 provides a summary on the presence or absence of ELFR and LLFR components for each subject during test and control conditions.
Effects of RF stimulation at 2 × MT on the flexion reflex
In Figure 2a the effects of RF stimulation at 2 × MT on the average LLFR (n=20) at a C-T interval of 0 ms are shown for subject 2. In these EMG recordings, the conditioning stimulation can be seen to reduce significantly the magnitude of the LLFR. A significant reduction in the size of the LLFR was observed in five of the seven SCI subjects. On average, the amplitude of the LLFR in these five subjects was reduced by 30±7.3% of control reflex values. The reduction in the reflex size was maintained over a wide range of C-T intervals covering periods in which the RF muscle is actively contracting (0–16 ms), and at longer intervals when the muscle is relaxing or relaxed (100, 120 ms) (Figure 2b). No significant difference in the size of the conditioned LLFR was encountered over the range of C-T intervals tested (P>0.05).

(a) The effects of RF stimulation at 2 × MT (0 ms C-T interval) on the full-wave rectified waveform average of the LLFR (20 reflex responses). The decrease in the amplitude of the LLFR was statistically significant (P<0.05) compared to the control reflex. Records are from subject 2. (b) Histogram showing the average magnitude of the LLFR along the C-T intervals tested, as a percentage of the associated control flexion reflex following RF muscle stimulation at 2 × MT. For all C-T intervals, the depression of the LLFR was statistically significant (P<0.05). Error bars designate the SEM. The different sizes of stimulus artefacts in the EMG traces were due to aliasing
A facilitation of the LLFR was observed in two subjects (S1 and S3) following FES of RF muscle at 2 × MT (Figure 3a and b). In subject 1, the LLFR was significantly increased compared to control values at short C-T intervals ranging from 2 to 14 ms. However, this facilitation was not maintained, and at a C-T interval of 120 ms the reflex was significantly reduced in size when compared to control reflex values. For subject 3, a considerable variation in the magnitude of the LLFR facilitation was seen at C-T intervals ranging from 0 to 12 ms but at C-T intervals of 14 and 16 ms the reflex was not significantly different from control values (Figure 3a) (P>0.05). At the longest C-T intervals tested (100–120 ms), facilitation of the LLFR re-emerged in this subject.

The long latency flexion reflex recorded in subjects S1 (a) and S3 (b) and the early component of the flexion reflex recorded in subject S1 (a) following RF muscle stimulation at 2 × MT are illustrated. Data represent the mean amplitude (±SEM) of the flexion reflex as a percentage of the associate control reflex observed at each C-T interval. Asterisks indicate cases of statistically significant differences between the control and the conditioned flexion reflex
The ELFR was present in three subjects following RF muscle stimulation at 2 × MT (S1, S3, and S5). However, a control estimate for the ELFR was only available for comparison in the data obtained from subject S1 (Figure 3a), being absent under control conditions in subjects 3 and 5. For subject 1, the ELFR was significantly reduced at all C-T intervals tested. Overall, Figure 3a suggests that for subject 1 the ELFR size continues to decrease over the range of C-T intervals tested. It is noteworthy that the changes in the ELFR in this subject are of different sign to the changes seen in the LLFR at short (0–16 ms) C-T intervals suggesting that they are generated and acted on by different spinal pathways.
Effects of RF stimulation at 0.7 and at MT on the flexion reflex
The conditioning effect of 0.7 × MT and MT RF stimulation was examined in six subjects (S2–S7). At stimulation intensities equal to MT the muscle response consisted of local fasciculation close to the electrodes sites. No mechanical activation of the muscle was evident following conditioning at 0.7 × MT. Only LLFRs were observed in the participating subjects. The average size of the conditioned flexion reflex for each C-T interval is presented in Figure 4. This figure presents a summary of data from all the six subjects tested.

The average size (±SEM) of the long latency flexion reflex for each conditioning test interval as a percentage of the control reflex size following RF muscle stimulation at 1 × MT and at 0.7 × MT is illustrated. The conditioning-test intervals are denoted on the abscissa. Asterisks indicate cases of statistically significant differences between the control and the conditioned reflex
RF stimulation at MT significantly depressed the LLFR for the C-T intervals of 2 and 4 ms, reducing the average amplitudes to 72 and 74% of the control LLFR, respectively. Decreasing the conditioning stimulus intensity to 0.7 × MT resulted also in a significant decrease in the size of the LLFR at each C-T interval tested (Figure 4).
Two-factor ANOVA showed that the flexion reflex depression observed at 0, 2 and 4 ms C-T intervals did not vary with changes in the level of the conditioning stimulation intensity, for example 2 × MT or 0.7 × MT (P=0.647). This suggests that at least part of the depression observed in the LLFR at each of the stimulation intensities studied may be due to activation of populations of cutaneous afferents close to the site of electrode placement. Note that at these levels of sensorimotor conditioning, the LLFR in subject 3 was significantly depressed, in contrast to the reflex facilitation observed with 2 × MT of RF muscle stimulation.
Discussion
The present work extends our previous observations that FES applied to the RF muscle produces a long-lasting depression in the transmission of the soleus H-reflex in neurologically intact and SCI subjects.24 Current findings reveal that FES-induced isometric contraction of the RF muscle and excitation of cutaneous afferents of the thigh result mainly in a depression of the LLFR in the majority of the SCI subjects tested (five out of seven). Our findings highlight that the pathways responsible for the generation of the flexion reflex can strongly be influenced by feedback resulting from FES. The consequences of this afferent feedback therefore should be considered when utilizing FES to promote walking in SCI patients.
FES-induced afferent feedback and its relation to the timing of sural nerve stimulation
FES directed to the RF muscle at 2 × MT is anticipated to generate a multisensory afferent volley that is composed of activity resulting from the direct excitation of afferent axons (axonal diameter⩾diameter of stimulated α motor axons), and the changing proprioceptive reaction to the FES-induced contraction. In our current experiments, it is important to consider the temporal structure of the FES-induced afferent feedback in relation to the time course of the evoked contractions and the range of C-T intervals investigated.
We have previously shown, using identical FES stimulation parameters, that the peak force of contraction in normal subjects occurs approximately 40 ms after the end of the stimulus train before returning to zero 150 ms later.24 Given that following SCI26 the maximal velocity of contraction in quadriceps increases by 50% and that the half relaxation time decreases by approximately 20%, it should be apparent that the short C-T interval range (0–16 ms) examined in this study will coincide with periods when the RF muscle is actively contracting. The longer C-T intervals of 100 and 120 ms will coincide with periods where the muscle is relaxing or relaxed. Thus, the initiation of the flexion reflex at the short and long C-T intervals will correlate with different phases of an evoked RF contraction and therefore to different epochs of FES-induced muscle afferent convergence to the spinal cord.
At conditioning stimulus intensities of 0.7 and 1 × MT the afferent volley will simply feature an activation of large diameter cutaneous and muscle afferents lying close to the stimulation electrodes.
FES-induced modulation of the LLFR
FES stimulation of the RF muscle resulted in LLFR depression in the majority of subjects at stimulation strengths above (five out of seven subjects tested) and below MT (six out of six subjects tested). The LLFR depression was present at all C-T intervals (0–120 ms) following RF stimulation at 2 × MT, and at the short C-T intervals tested (ie 0–4 ms) in response to 0.7 × MT. Thus, it would seem safe to conclude that low-threshold muscle and cutaneous afferents recruited directly by the stimulus train can exert a significant depressive action on flexion reflex pathways in SCI subjects, and that this depression is established early in response to FES stimulation.
However, considering the short lag time associated with transmission of the direct FES-induced afferent volley to the spinal cord and the long latency of the flexion reflex, it is unlikely that postsynaptic inhibition resulting from the action of afferents recruited directly by the RF stimulus can alone account for the duration of reflex depression seen here (>120 ms). Recurrent inhibition has been reported to be preserved in humans after SCI,27 and although RF stimulation at 2 × MT will provoke antidromic activation of motor axons, the time course of recurrent inhibition (∼30 ms) is too brief to account for the long lasting reflex depression observed.28, 29 Hence, postsynaptic inhibition resulting from direct electrical stimulation of afferent or efferent axons is unlikely to be a major factor in the depression seen in the LLFR.
RF-induced contraction at 2 × MT will evoke changes in muscle afferent activity over the time course of the evoked contraction. Accordingly, when sural nerve stimulation occurs during active force generation (short C-T intervals) the resulting flexion reflex will be generated during a period when Ib afferent feedback will be increasing and muscle spindle output decreasing.30, 31, 32 At long C-T intervals, the reflex will occur during periods when muscle spindle afferent activity is recovering and Ib afferent activity has been reduced. Despite the different afferent conditioning experienced by the spinal cord during these phases of evoked muscle contraction, no clear differences existed in the depression of the LLFR at short or long C-T intervals. The constant level of the reflex depression across the C-T intervals, strongly suggests that ongoing postsynaptic inhibition of the TA motor pool due to afferent activity caused by the muscle contraction is not a significant factor in generating the flexion reflex depression. Importantly, at the inter-stimulus interval used here (10 s), we also found no evidence of habituation in the flexion reflex.4, 33, 34, 35
Stimulation of afferents that can evoke flexion reflexes are known to potentiate presynaptic inhibition of Ia afferent terminals in healthy and SCI humans.36, 37 Given that the flexion reflex depression was long lasting and of similar strength above and below MT, it is conceivable that a common mechanism mediated the depression at the conditioning intensities employed. It is therefore likely that presynaptic inhibitory mechanisms play a significant part in establishing and maintaining the reflex depression observed following FES.
In two subjects (S1 and S3), the LLFR was enhanced as a consequence of FES conditioning at 2 × MT. Why a facilitation of the LLFR occurred in these two subjects in comparison with the others in the study is not clear and would warrant further investigation. However, it is worth noting that for S1 the facilitation was only seen at short C-T intervals during the period where the RF muscle would be actively generating force and that the LLFR was depressed at the longest C-T intervals tested in this subject. In animal and human locomotion studies reflex reversal or gating is commonly reported.38, 39 It is therefore conceivable that depending on prevailing conditions a conditioning stimulus could generate a different action on flexion reflex pathways in the same or different subjects.
Observations on the expression of the ELFR
The incidence of the ELFR was low. This is in agreement with previous observations on this reflex component in SCI subjects,22, 23 and its known high variability.34, 35 In this study, the flexion reflex stimulus intensity was normalized to the threshold of the first sign of evoked TA EMG activity, which for all subjects corresponded to the appearance of the LLFR. Thus, the absence of an ELFR component in the majority may be due to the stimulation intensity being subthreshold for the ELFR. In normal subjects, separable flexion reflex components are associated with activation of different groups of afferents,40 and in stroke patients the threshold of the ELFR component appears increased.41
In a single subject (S1), an ELFR was observed under control conditions, and in further two subjects it was evoked when the test reflex stimulus train was conditioned by 2 × MT stimulation. It is noteworthy that for subject 1 the ELFR and LLFR components displayed different modulation patterns (inhibition/facilitation) in response to the same conditioning stimuli supporting the view that transmission of flexion reflex activity at short and at long latencies is mediated through different spinal interneuronal pathways.42
Functional considerations for SCI rehabilitation
Electrical stimulation of skeletal muscle (above and below MT) appears to be a strong modulator of spinal reflex excitability in individuals with chronic motor complete SCI and generates long lasting actions. The LLFR in complete SCI has been compared with the late flexion reflex observed in L-dopa-treated spinal animals,22, 37, 43 a reflex which in the cat is considered to utilize interneurons of spinal locomotor centres.44, 45 Our findings demonstrate that as has been found in reduced preparations9, 10, 12, 46 the LLFR in SCI man is influenced by afferent feedback from both cutaneous and muscle afferents.
FES protocols commonly utilize the flexion reflex to provide a synchronized movement of hip, knee, and ankle during the swing phase of assisted locomotion programs.2, 47 In these programs, a reciprocal walking pattern is accomplished by sustaining the stance phase of a step by FES of the quadriceps before inducing swing (at the appropriate time) via a flexion reflex. It has been noted that when using this approach for gait rehabilitation the resulting step can be of poor quality due to the variability in the amplitude of the flexion reflex.48 Based on the current findings, part of this variability might be attributed to the long lasting effects associated with the afferent feedback generated via the FES applied to the quadriceps muscle during stance. We would therefore suggest that in order to maximize the effectiveness of FES assisted gait that the central actions resulting from the sensory consequences of the applied electrical stimulation on individual subjects are considered.
References
Bajd T, Kralj A, Turk R, Benko H, Sega J . The use of a four channel stimulator as an ambulatory aid for paraplegic patients. Phys Ther 1983; 63: 116–120.
Bajd T, Kralj A, Stefancic M, Lavrac N . Use of functional electrical stimulation in the lower extremities of incomplete spinal cord injured patients. Artif Organs 1999; 23: 403–409.
Kralj T, Bajd R, Turk R, Krajnik J, Benko H . Gait restoration in paraplegic patients: a feasibility demonstration using multichannel surface electrodes FES. J Rehabil Res Dev 1983; 20: 3–20.
Andrews BJ, Baxendale RH, Granat MH, Nicol DJ . Long latency flexion reflexes in man may limit restoration of gait in FES in SCI man. J Physiol (London) 1990; 420: 63.
Andrews BJ, Nicol DJ, Granat MH, Baxendale RH . Control of FES flexion reflex stepping in paraplegics. Neuromuscular Systems 1991; 13: 887–888.
Granat MH, Nicol DJ, Baxendale RH, Andrews BJ . Dishabituation of the flexion reflex in spinal cord injured man and its application in the restoration of gait. Brain Res 1991; 559: 344–346.
Nicol DJ, Granat MH, Tuson SJ, Baxendale RH . Variability of the dishabituation of flexion reflexes for FES assisted gait in spinal injured man. Med Eng Phys 1998; 20: 182–187.
Hagbarth KE . Excitatory and inhibitory skin areas for flexor and extensor motoneurones. Acta Physiol Scand 1952; 26(Suppl 94): 1–57.
Grillner S, Rossignol S . On the initiation of the swing phase of locomotion in chronic spinal cats. Brain Res 1978; 146: 269–277.
Grillner S, Rossignol S . Contralateral reflex reversal controlled by limb position in the acute spinal cat treated with clonidine i.v. Brain Res 1978; 144: 411–414.
Baxendale RH, Ferrell WR . Modulation of transmission in flexion pathways by knee joint afferent discharge in the decerebrate cat. Brain Res 1980; 202: 497–500.
Conway BA, Scott DT, Riddell JS . The effects of plantar nerve stimulation on long latency flexion reflexes in the acute spinal cat. In: Taylor A, Gladden MN, Durbada R (eds). Alpha and Gamma Motor Systems. Plenum Press: 1995, pp 593–595.
Ellrich J, Treede RD . Convergence of nociceptive and non-nociceptive inputs onto spinal reflex pathways to the tibialis anterior muscle in humans. Acta Physiol Scand 1998; 163: 391–401.
Andersen OK, Sonnenborg FA, Arendt-Nielsen L . Modular organization of human leg withdrawal reflexes elicited by electrical stimulation of the foot sole. Muscle Nerve 1999; 22: 1520–1530.
Schomburg ED, Steffens H, Wada N . Parallel nociceptive reflex pathways with negative and positive feedback functions to foot extensors in the cat. J Physiol (London) 2001; 536: 605–613.
Sonnenborg FA, Andersen OK, Arendt-Nielsen L, Treede RD . Withdrawal reflex organisation to electrical stimulation of the dorsal foot in humans. Exp Brain Res 2001; 136: 303–312.
Zehr EP, Stein RB, Komiyama T . Function of sural nerve reflexes during human walking. J Physiol (London) 1998; 507: 305–314.
Conway BA, Knikou M . Effects of applied plantar pressure and electrically induced muscle contraction on reflex excitability in spinal cord injured subjects. Eur J Neurosci (Suppl) 2000; 12: 198.
Knikou M, Conway BA, Rymer WZ . Effects of electrically induced muscle contraction on reflex excitability in SCI subjects. Soc Neurosci Abstr 2000; 57: 19.
Maynard FM et al. International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord 1997; 35: 266–274.
Ashworth B . Preliminary trial of carisoprodol in multiple sclerosis. Practioner 1964; 192: 540–542.
Roby-Brami A, Bussel B . Long latency spinal reflex in man after flexor reflex afferent stimulation. Brain 1987; 110: 707–725.
Shahani BT, Young RR . Human flexor reflexes. J Neurol Neurosurg Psychiatry 1971; 34: 616–627.
Knikou M, Conway BA . Reflex effects of induced muscle contraction in normal and spinal cord injured subjects. Muscle Nerve 2002; 26: 374–382.
Ladoucer M . The therapeutic effect of functional electrical stimulation assisted walking in incomplete spinal cord injured participants. Sixth Internet World Congress for Biomedical Sciences Presentation No. 66, 2000. http://www.uclm.es/inabis2000/index.htm.
Gerrits HL, De Haan A, Hopman MTE, Van Der Woude LHV, Jones DA, Sargeant AJ . Contractile properties of the quadriceps muscle in individuals with spinal cord injury. Muscle Nerve 1999; 22: 1249–1256.
Barbeau H, Marchand-Pauvert V, Meunier S, Nicolas G, Pierrot-Deseilligny E . Posture-related changes in heteronymous recurrent inhibition from quadriceps to ankle muscles in humans. Exp Brain Res 2000; 130: 345–361.
Bussel B, Pierrot-Deseilligny E . Inhibition of human motoneurones, probably of Renshaw origin, elicited by an orthodromic motor discharge. J Physiol (London) 1977; 269: 319–339.
Meunier S, Penicaud A, Pierrot-Deseilligny E, Rossi A . Monosynaptic Ia excitation and recurrent inhibition from quadriceps to ankle flexors and extensors in man. J Physiol (London) 1990; 423: 661–675.
Matthews PBC . Mammalian Muscle Receptors and Their Central Actions. Edward Arnold Publishers: 1972.
McKeon B, Burke D . Muscle spindle discharge in response to contraction of single motor units. J Neurophysiol 1984; 49: 291–302.
Halliday DM, Kakuda N, Wessberg J, Vallbo AB, Conway BA, Rosenberg JR . Correlation between Ia afferent discharges, EMG and torque during steady isometric contraction of finger muscles. In: Taylor A, Gladden MN, Durbada R (eds). Alpha and Gamma Motor Systems. Plenum Press: 1995, pp 547–549.
Fuhrer MJ . Interstimulus interval effects on habituation of flexor withdrawal activity mediated by the functionally transected human spinal cord. Arch Phys Med Rehabil 1976; 57: 577–582.
Dimitrijevic MR, Nathan PW . Studies of spasticity in man. 3. Analysis of reflex activity evoked by noxious cutaneous stimulation. Brain 1968; 91: 349–368.
Dimitrijevic MR, Nathan PW . Studies of spasticity in man. 4. Changes in flexion reflex with repetitive cutaneous stimulation in spinal man. Brain 1970; 93: 743–768.
Rossi A, Decchi B, Ginanneschi F . Presynaptic excitability changes of group Ia fibres to muscle nociceptive stimulation in humans. Brain Res 1999; 818: 12–22.
Roby-Brami A, Bussel B . Effects of FRA stimulation on the soleus H-reflex in patients with a complete spinal cord lesion: evidence for presynaptic inhibition of Ia transmission. Exp Brain Res 1990; 81: 593–601.
Côté M-P, Ménard A, Gossard J-P . Spinal cats on the treadmill: changes in load pathways. J Neurosci 2003; 23: 2789–2796.
Duysens J, Tax AA, Trippel M, Dietz V . Phase-dependent reversal of reflexly induced movements during human gait. Exp Brain Res 1992; 90: 404–414.
Meinck HM, Kuster S, Benecke R, Conrad B . The flexor reflex-influence of stimulus parameters on the reflex response. Electroenceph Clin Neurophysiol 1985; 61: 287–298.
Milanov IG . Flexor reflex for assessment of common interneurone activity in spasticity. Electromyogr Clin Neurophysiol 1992; 32: 621–629.
Schomburg ED . Spinal sensorimotor systems and their supraspinal control. Neurosci Res 1990; 7: 265–340.
Roby-Brami A, Bussel B . Inhibitory effects on flexor reflexes in patients with a complete spinal cord lesion. Exp Brain Res 1992; 90: 201–208.
Lundberg A . Multisensory control of spinal reflex pathways. In: Granit R Pomeiano O (eds) Reflex Control of Posture and movement. Progress in Brain Research. Elsevier: Amsterdam 1979, pp 11–28.
Baldissera F, Hultborn H, Illert M . Integration in spinal neuronal systems. In: Brooks VB (ed) Handbook of Physiology, Motor Control. American Physiological Society: Bethesda, MD 1981, pp 508–595.
Conway BA, Hultborn H, Kiehn O . Proprioceptive input resets central locomotor rhythm in the spinal cat. Exp Brain Res 1987; 68: 643–656.
Barbeau H, Ladoucer M, Mirbagheri MM, Kearney RE . The effect of locomotor training combined with functional electrical stimulation in chronic spinal cord injured subjects: walking and reflex studies. Brain Res Rev 2002; 40: 274–291.
Granat MH, Heller MH, Nicol DJ, Baxendale RH, Andrews BJ . Improving limb flexion in FES gait using the flexion withdrawal response for the spinal cord injured person. J Biomed Eng 1993; 15: 51–56.
Acknowledgements
We thank the support of staff and patients of the Queen Elizabeth National Spinal Injuries Unit, Scotland, UK.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Knikou, M., Conway, B. Effects of electrically induced muscle contraction on flexion reflex in human spinal cord injury. Spinal Cord 43, 640–648 (2005). https://doi.org/10.1038/sj.sc.3101772
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101772
Keywords
This article is cited by
-
Brain and spinal cord paired stimulation coupled with locomotor training affects polysynaptic flexion reflex circuits in human spinal cord injury
Experimental Brain Research (2022)
-
Transspinal stimulation and step training alter function of spinal networks in complete spinal cord injury
Spinal Cord Series and Cases (2021)
-
Augmented visual feedback counteracts the effects of surface muscular functional electrical stimulation on physiological tremor
Journal of NeuroEngineering and Rehabilitation (2013)
-
Flexion reflex modulation during stepping in human spinal cord injury
Experimental Brain Research (2009)
-
Plantar cutaneous input modulates differently spinal reflexes in subjects with intact and injured spinal cord
Spinal Cord (2007)
