
Abstract
Study design: In vitro studies using isolated guinea pig spinal cord.
Objectives: To develop an alternative model using isolated guinea pig spinal cord, which can be used to screen antioxidants for in vivo SCI treatment.
Setting: Department of Basic Medical Sciences, Purdue University, West Lafayette, Indiana, USA.
Methods The compression injury was induced by a constant-displacement of 5-s compression of spinal cord using a modified forceps possessing a spacer. Reactive oxygen species (ROS) were evaluated using three distinct methods: fluorescence microscopy, lipid peroxidation assay, and flow cytometry.
Results: The injury-mediated ROS increases are comparable with other in vivo studies and consistent with our previous observation using a similar injury model and measured with electrophysiological and anatomical technique. Further, ascorbic acid, hypothermia, or the combination of both significantly suppressed superoxide and lipid peroxidation. The combination treatment was the most effective when compared with ascorbic acid or hypothermia alone.
Conclusion: This in vitro model has the advantage of replicating some of the in vivo conditions while gaining the ability to control the experimental conditions. This in vitro model is suitable to study the mechanisms of ROS generation and degradation and can also be used to critically evaluate the effective suppressor of ROS in the contents of spinal cord traumatic injury.
Similar content being viewed by others

Introduction
Traumatic spinal cord injury (SCI) is the consequence of a primary physical injury and a secondary progressive process leading to tissue destruction and neurological dysfunction.1,2,3,4,5 Although the initial function and anatomical deficits are the results of primary injury, the delayed damage is usually more profound and mediated by a series of secondary injury mechanisms. Among these secondary injury mechanisms, reactive oxygen species (ROS) have been postulated to play a critical role in CNS trauma.6,7,8 It is well established that ROS increase significantly following CNS mechanical trauma in live animals.6,9,10 The inhibition of ROS can provide behavioral and functional recovery following various types of injuries.1,6,11 Therefore, reducing oxidative stress of the tissue is considered to be a potential target for effective pharmacological intervention to reduce the secondary neuron damage and enhance overall functional recovery following trauma.11,12 Despite the clinical significance, the detailed generation, regulation of, and target of action of ROS are not firmly established. This is partially due to the limitations of experimental models. For example, much of the evidence for the pathogenic roles of ROS and the protective role for antioxidants in attenuating CNS trauma came from studies using either in vivo whole animals or in vitro cell culture models. Although the in vivo study is more relevant to clinical injury, its experimental condition is difficult to control and is not suitable to dissect out the effects of a particular secondary insult, such as the effects of ROS. On the other hand, cell culture clearly has the advantage of a better-controlled environment. However, its artificial condition usually does not fully mimic an in vivo situation. In particular, it lacks the mechanical interactions between the cells and extracellular matrix which could play important roles in the injury and recovery process of the CNS, especially the spinal cord following mechanical insults.
Motivated to establish an alternative preparation, we would like to establish a model that can to a certain degree preserve the local environment seen in vivo while gaining the ability to control the experimental conditions seen in cell cultures. Here we report that we have developed such a model using isolated guinea pig spinal cord segments which were kept alive and viable in a chamber (equivalent to an organ culture). Using this model, we were able to examine free radical formation and subsequent damage using three distinct methods: fluorescent microscopy, flow cytometry, and biochemical examination of ROS.
Our findings suggest that this isolated spinal cord model mimics the increase of ROS to a degree similar to that in live animal studies. Further, such injury-induced ROS elevation can be inhibited using either physical or pharmacological means. These findings suggest that the current in vitro model possesses the ability to express ROS-related pathology and that such changes can be regulated through physical and pharmacological means. Coupled with the feature that the experimental condition can be well controlled, we conclude that this model is suitable for studying the mechanism and regulation of ROS, and searching for effective inhibitors of ROS. From this understanding, we hope to derive new approaches for the treatments of acute spinal cord injury, and perhaps derive insights to optimize current therapy.
Methods
Isolation of spinal cord and injury model
All animals used in this study were handled in strict accordance with the NIH guide for the Care and Use of Laboratory Animals and the experimental protocol was approved by the Purdue Animal Care and Usage Committee. In these experiments, every effort was made to reduce the number and suffering of the animals used. Adult Hartley guinea pigs, weighing 300–500 g were anesthetized deeply with ketamine (60 mg/kg), xylazine (10 mg/kg). They were then perfused through the heart with 500 ml of oxygenated, cold Kreb's solution (15°C) to remove blood and lower core temperature. The vertebral column was excised rapidly and a complete laminectomy was performed. The spinal cord was removed from the vertebrae and immersed in cold Kreb's solution. The cord was separated first into two halves by midline sagittal division. The gray matter strips were further obtained by removing most of the ventral and dorsal side white matter with a scalpel blade against a soft plastic block (Figure 1A). The composition of the modified Krebs' solution was as follows: NaCl 124 mM; KCl 2 mM; KH2PO4 1.2 mM; MgSO4 1.3 mM; CaCl2 2 mM; dextrose 20 mM; NaHCO3 26 mM, equilibrated by bubbling with 95% O2/5% to produce a pH of 7.2–7.4. The spinal cord strips were maintained in oxygenated Kreb's solution at 37°C for at least 1 h before the onset of the experiment. This was to ensure the recovery from dissection before experimentation. All the samples were bubbled with 95% O2/5% CO2 throughout the duration of the experiment.

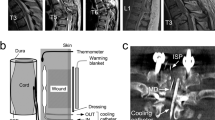
Schematic drawing of the isolated spinal cord strips, the injury device, and its application. (A) After being isolated from the guinea pig, the spinal cord was split into two halves. Most of the white matter was then removed to give rise to the gray matter strip which was used in the majority of the experiments described in this study. A small number of initial experiments were carried out using the whole spinal cord. (B) Following the extraction of the gray matter strip, the tips of the forceps were placed on both sides of the strip. The forceps were then closed quickly, compressing the spinal cord, and were held against the spacer for 5 s. (C) Front and side view of the end of the modified forceps, to show the tips ground to produce two parallel inner surfaces, 8 mm long, which rest 0.8 mm apart when the forceps are closed by finger pressure against the spacer. (D) Diagram showing the method of hemi-compression. The forceps used here is the same as that shown in B and C, except the thickness of the spacer is about 1.5 mm. (E) Diagram showing the technique of whole-width compression. The thickness of the spacer was about 1.2 mm
For all the experiments using three distinct methods, the spinal cords were always randomly divided into three groups: control-uninjured, compression-untreated, and compression-treated. The control-uninjured group did not receive any compression. The compression-untreated group received the compression injury which was induced by a constant-displacement of 5s compression of spinal cord using a modified forceps possessing a spacer (Figure 1). The compression-treated group was placed in Kreb's solution containing 10 mM ascorbic acid and/or kept at room temperature (25°C) after compression. In contrast, the control-uninjured and compression-untreated groups were bathed in the modified Kreb's solution which does not contain ascorbic acid and kept at 37°C.
A small number of experiments were conducted using the entire spinal cord, where either the whole width or one half the width of the cord along the midline, were compressed (Figure 1E,F).
Functional assessment of isolated spinal cord tissue
The function of the spinal cord was assessed by monitoring compound action potential conducted along the bundles of axons within the white matter. This functional recording was carried out using a double sucrose-gap recording chamber. Briefly, white matter strips were extracted and mounted on the double sucrose gap-recording chamber. The central compartment of the chamber was superfused with oxygenated Kreb's solution. The ends of the tissue were carried through the sucrose gap channels to side compartments that were later filled with isotonic (120 mM) potassium chloride. Silicone grease was used to block the flow of fluid between different compartments. The temperature was maintained at 37°C throughout the experiment. The axons were stimulated and compound action potentials recorded by two pairs of silver-silver chloride wire electrodes positioned within the side chambers and the central bath. Recordings were made using a Neurodata Instruments bridge amplifier and Neurocorder, for digital data storage on videotape. Subsequent analysis was performed using Labview® software (National Instruments) on a Dell computer.
Measurement of ROS
Lipid peroxidation (LPO)
LPO was analyzed using a lipid hydroperoxide assay kit from Cayman Chemical Company (Ann Arbor, MI, USA). Briefly, the samples of 6 mm in length were obtained from the center of the injury site, weighed and homogenized. The homogenization was carried out in a Teflon-glass homogenizer in the modified Kreb's solution (no ascorbic acid, pH 7.2) to obtain a 10% (w/v) homogenate. Immediately after homogenization, lipid hydroperoxides were extracted from the sample into chloroform. The measurement was then performed immediately upon extraction. The chromogenic reaction was conducted at 37°C for 5 min. The absorbance was read at 500 nm using a 96 well plate with a spectrophotometer (SLT spectra plate reader, SLT Labinstrument, Salzburg, Australia). The agent, 13-hydroperoxy octadecadienoic acid (13-HpODE), was used as standard. Tissue lipid peroxide was calculated and expressed as nanomoles per 100 mg of wet tissue (nmol/100 mg).
Flow cytometry
Flow cytometric analysis of intracellular superoxide (O2−) was performed using hydroethidine (HE; Molecular Probes, Eugene, OR, USA) by a standard protocol.13 HE is oxidized selectively to ethidium by O2−, thus reflecting intracellular O2− production. Single cells were obtained by a combination of mechanical and enzymatic dissociation methods with some modifications from the methods described by Grogan and colleagues.14 Briefly, spinal cord segments from the center of the injury site were cut into small slices with a surgical blade and then incubated in previously oxygenated (95% O2/5% CO2) modified Kreb's solution (no ascorbic acid) with 0.05 mg/ml pronase for 20 min (keep oxygenating). The concentration of 0.05 mg/ml was determined to be the lowest concentration of pronase that would enable effective dissociation of cells and at the same time cause minimal cell damage. The enzymatic dissociation was terminated by washing the cells three times with PBS. The remaining single cells (106) were washed and then incubated in 1 ml of 1 μM hydroethidine solution at 37°C for 5 min in the dark. Cells were washed twice in PBS and resuspended in 1 ml of PBS for flow cytometric analysis. Flow cytometric data acquisition and analysis were performed on an EPICS XL (Beckman-Coulter, Miami, FL, USA). The flow cytometer was equipped with an argon laser set at 488 nm and a 15 mW output power. The red fluorescence of HE was monitored using a 610 nm long pass filter. For each parameter investigated, 2×104 events (cells) were analyzed per sample.
Fluorescent microscopy
The spinal cord samples were incubated with 1 ml of PBS with HE at final concentrations of 1 μM for 5 min at 37°C in the dark before fixation. After fixation with 3.7% formaldehyde for 2 h, the segments were cut into sections of 40 μm, using an EMS-4000 Tissue Slicer (Electron Microscopy Sciences, Fort Washington, PA, USA). The sections were dehydrated through a graded series of acetone, transferred to xylene and mounted on glass slides with DPX. The sections were then observed with an Olympus Vanox fluorescent microscope (excitation filter: BP 545 nm; barrier filter: 0–590 nm). HE fluorescent images were captured through a 2×objective, using a high-resolution CCD camera (DEI-750, Optronic Eng., Goleta, CA, USA). At this magnification, we were able to capture the whole section with just one image. The images were saved by the image analysis program for later quantification. Camera exposure and light settings were kept identical during each experiment.
Quantification was done from coded slides by an individual who did not know the treatment history of the specimen. The fluorescence intensity measurements were carried out by an image analysis program, Sigmascan Pro (SPSS Science, Chicago, IL, USA). For each tissue sample, which was about 7 mm long, five sections were chosen randomly and the fluorescent intensities were measured separately. An average of the values from these five sections was calculated and used as the final fluorescent value of the cord sample. For each section image, the area occupied by the spinal cord tissue was carefully delineated manually along the edge and the fluorescent intensity of the tissue was taken. Four smaller areas (5% of the total field) were randomly selected at each corner (outside of the spinal cord tissue) and the average fluorescence intensity of these four areas was used as background intensity. The fluorescence intensity of the spinal cord samples was obtained by subtracting the background fluorescence from that of the spinal cord image and expressed in arbitrary units.
Chemicals and reagents
Hydroethidine (HE) was purchased from Molecular Probes (Eugene, OR, USA). A lipid hydroperoxide assay kit was purchased from Cayman Chemical Company (Ann Arbor, MI, USA). DPX Mountant for histology and all other chemicals used were obtained from Sigma Chemical Co. (St. Louis, MO, USA).
Statistical analysis
All data are represented as means±standard deviations. Statistical analysis was performed using Student-t-test. Values were accepted as being statistically significantly different if a P value was <0.05.
Results
Functional assessment of isolated spinal cord tissue
As shown in Figure 2, the amplitude of the CAP from a typical uninjured cord strip showed little decay with 4 h of observation. In addition, the overall shape of the CAP remains virtually the same. An average decay of the CAP amplitude at the end of the 4 h-observation was 4% (n=4). This indicates little deterioration of the isolated spinal cord tissue and demonstrates the functional competency still available at the end of the observation.

Compound action potential (CAP) recording from isolated spinal cord white matter. Each symbol represents the amplitude of a CAP. The length of the recording, as indicated in the X-axis, was more than 4 h, which is the maximal length for the experiments carried out in this study. The individual CAPs (initial and 4 h) shown here were taken at the time of experiment indicated in the graph. Note that there were very little changes in amplitude and the overall shape of CAPs following 4 h of in vitro recording, suggesting the full physiological competency of the isolated spinal cord tissue by the end of each experiment
Fluorescence microscopy
In order to visualize the expression of ROS in situ and gain insights in terms of spatial differential expression of ROS within the spinal cord transverse section, we labeled the spinal cord tissue with HE, whose fluorescence intensity signifies the level of O2−. First, to take advantage of this in vitro model, we performed a hemi-compression to a whole spinal cord using a modified forceps (Figure 1D and Methods section). This was done so that we can use the uninjured half of the cord as an internal control and to unequivocally demonstrate that O2− increases as a result of deliberate injury. As shown in Figure 3A, a standard hemi-compression produced a significantly increased intensity of fluorescence in the injured half compared with the uninjured half, when examined at 1 h after compression. This clearly indicates that compression injury can cause an increase of O2− production in our in vitro model. The fact that the uninjured half showed minimal fluorescence (except a very thin line at the edge of the cord) indicates that the isolating procedure produced minimal tissue damage. This is consistent with our previous studies with this model using the HRP-exclusion assay as well as action potential and membrane potential recordings using a sucrose-gap recording chamber.15,16,17,18,19

Examples of hydroethidine (HE) fluorescence labeling intensity at 1 h after compression injury under different conditions. Vibratome sections were cut in the middle of the injury site. (A) A typical cross-section from a cord is shown in which half of the cord was compressed (see Figure 1D). Note the significantly higher fluorescence labeling intensity in the injured half (left) compared to the control half (right) of the spinal cord. (B) A representative cross-section is shown in which the whole cord was moderately compressed (Figure 1E). Note the fluorescence labeling is more intense in the gray matter area compared to the white matter in the cross-section. (C,D) Fluorescence intensity of a representative area in the gray matter in the control-uninjured group with lower (C) and higher magnification (D). (E,F) Fluorescence intensity in the gray matter of the injured-untreated group with lower (E) and higher magnification (F). (G,H) Fluorescence intensity in the gray matter in the injured-treated group (ascorbic acid and hypothermia) with lower (G) and higher magnification (H). (I) Quantification of HE fluorescence intensity in the gray matter at 1 h after injury. The fluorescence intensity of the sample area was obtained by background subtraction. Values were expressed as percentages of control groups. Note the compression injury caused significant increase of HE fluorescence intensity (n=5, P<0.05 as compared with control). Ascorbic acid and hypothermia reduced HE fluorescence intensity significantly (n=5, P<0.05, as compared with injury). Scale bars: A=B=200 μm, C=E=G=40 μm, D=F=H=10 μm
We would like to determine whether there is any difference in fluorescence intensity between the gray matter, which mainly consists of neurons and glia cells, and white matter, which mainly consists of axons, in our model. This was proven to be indeed the case using the fluorescent microscopy technique. As shown in Figure 1E, a moderate compression was performed to a whole spinal cord segment. In a representative transverse section shown in Figure 3B, the area of high fluorescent intensity coincides almost exactly with the area of gray matter. Therefore this clearly shows that the gray matter has higher fluorescence intensity than white matter as a result of mechanical injury in our model.
Since it is clear that gray matter has higher fluorescence intensity, we decided to focus on gray matter to study the inhibition of O2− by antioxidants and low temperature. As shown in Figure 3, a standard compression produced a higher fluorescence level when examined at 1 h after injury (Figure 3E,F) compared with control-uninjured group (Figure 3C,D). Such an injury-induced increase of ROS can be inhibited by the combined treatment of ascorbic acid and hypothermia (Figure 3G,H). Quantitative analysis shows that the increase of ROS following injury is statistically significant as is the decrease of ROS by the treatment of ascorbic acid and hypothermia. Specifically, the fluorescent intensity of the samples in the injured group increased about 100% 1 h after injury (Figure 3I) (P<0.01, n=5), while the combination of ascorbic acid and hypothermia reduced the increase to 45%, a reduction of 55% (P<0.01, n=5).
Lipid peroxidation
In this study, we first examined lipid peroxide generation and its regulation 1 h after compression. The tissue used consisted mainly of gray matter. As we mentioned in the Methods section, the spinal cords were divided into three groups (control-uninjured, compression-untreated, and compression-treated). First, as shown in Figure 4A, the control-uninjured group had a minimal LPO level, 6.86±1.26 nmol/100 mg. This level is consistent with our findings based on fluorescent labeling of O2−. This level is also comparable with other in vivo studies.20,21 Secondly, a standard compression produced an LPO level of 21.23±3.22 nmol/100 mg at 1 h after injury, a 200% increase from the control-uninjured group (P<0.01, n=5). Thirdly, a treatment of either ascorbic acid or hypothermia to the compressed cords reduced the lipid peroxidation level of 17.96±3.0 nmol/100 mg and 16.43±2.89 nmol/100 mg; both are significantly lower than those measured in the compression-untreated group (P<0.01, n=5). In addition, the combination treatment of ascorbic acid and hypothermia was able to reduce the level to lipid peroxidation to 12.32±2.46% nmol/100 mg, a near 50% reduction (P<0.001, n=5). This combination treatment is clearly more effective than ascorbic acid or hypothermia alone.

The change of lipid peroxidation (LPO) following compression and its inhibition. (A) The elevation of LPO following compression and its inhibition at 1 h post-injury. LPO (nmol/100 mg wet tissue) was expressed as mean±SD (n=5 in each group). *Indicates significant difference compared to injury group (P<0.01. (B) Time course of LPO changes in control and following compression and treatment. The LPO value at time point `0' represents that of the spinal cord 1 h after isolation. No significant difference was found between the LPO value of the spinal cords taken 1 h after isolation and those taken at 1, 2, 3, and 4 h after the onset of the experiment (n=6, P>0.05). Compression injury resulted in significant increases of LPO at 1, 2, 3, and 4 h after injury (n=6, P<0.01). Note that the highest LPO value occurred at 1 h after injury. The combination treatment of ascorbic acid and hypothermia significantly lowered the injury-mediated elevation of LPO at all time points examined (n=6, P<0.01). *Indicates significant difference (P<0.01) between control-uninjured and injured-untreated groups. **Indicates significant difference (P<0.01) between injured-untreated and injured-treated groups
Since it is possible that the increase of ROS and lipid peroxidation lasts more than 1 h, we set out to determine the time course (up to 4 h following injury) of the increase of lipid peroxidation and its inhibition by ascorbic acid and hypothermia. As is shown in Figure 4B, the LPO level of the control-uninjured group remained low during the period of experimentation (4 h following isolation). Compression produced a significant increase of LPO during the entire 4 h period following injury (P<0.01, n=6), with the peak increase at 1 h after injury (up to 200% increase). Likewise, the combination treatment of ascorbic acid and hypothermia reduced the production of LPO significantly compared to the compression-untreated group in every point that was measured (P<0.01, n=6).
Measurement of superoxide (O2−) generation by flow cytometry
In this study, the cords were again divided into three groups, similar to the study using LPO. The level of O2− was determined by ethidium fluorescence, which is converted from HE upon oxidation by O2−. Figure 5A displays three histograms of flow cytometry measurements taken at 1 h following injury. These three histograms represent three groups: control-uninjured, compression-untreated, and compression-treated, respectively. It is important to point out that the peak of fluorescent intensity had shifted to the right from a to b, indicating an increase of fluorescent intensity. The overall intensity was reduced from b to c due to the combination treatment of ascorbic acid and hypothermia. Figure 5B shows the quantification and the time course (1–4 h following injury) of the increase of fluorescence intensity and subsequent decrease by treatment. The fluorescence intensity in compression-untreated groups was significantly higher at all of the time points examined, ie, 1, 2, 3, and 4 h after injury, as compared with that of controls (a 26–33% increase, P<0.01 at all time points, n=5). Consistent with the findings from other methods, the increase was inhibited by the combined treatment of ascorbic acid and hypothermia at all time points (1–4 h following injury) (P<0.05, n=5).

Flow cytometry analysis of intracellular superoxide anion (O2−) generation after compression injury and combination treatment of ascorbic acid and hypothermia. Intracellular O2− levels were evaluated after a period of 5-min incubation with HE solution. (A) A typical experiment showing the level of O2− detected by flow cytometry in control-uninjured (a), injured-untreated (b), and injured-treated group (c) respectively. Data were collected at 1 h after injury or injury and treatment. (B) Time course of O2− changes up to 4 h in control and following compression and treatment. No significant difference was found in the control-uninjured group between the ethidium bromide (EB) fluorescence value of the spinal cords taken 1 h after isolation (time point `0') and those taken at 1, 2, 3, and 4 h after the onset of the experiment (n=5). Compression injury resulted in significant increases of EB fluorescence intensity at 1, 2, 3, and 4 h after injury (n=5, P<0.01). Note that the highest EB fluorescence level occurred at 1 h after injury. The combination treatment of ascorbic acid and hypothermia significantly lowered the injury-mediated elevation of EB fluorescence at all the time points examined (n=5, P<0.01). *Indicates significant difference (P<0.01) between control-uninjured and injured-untreated groups. **Indicates significant difference (P<0.01) between injured-untreated and injured-treated groups
Discussion
Isolated guinea pig spinal cord injury model
It is well known that reactive oxygen species (ROS) play an important role in post-traumatic neuronal degeneration. The generation and regulation of such compounds are the focus of many investigations in CNS injury.6,11,12 Such studies have mainly been carried out using either in vivo whole animal or in vitro cell culture models.4 While both models are useful in studying the mechanisms of the formation and the adverse effects of oxygen radicals in cellular or whole animal levels, they have limitations. We have developed an alternative model using isolated guinea pig spinal cords, which to a certain degree preserves the local environment as that of the in vivo conditions while gaining the ability to better control the experimental conditions. Our experimental results suggest that this model is appropriate for studying ROS injuries in the context of the spinal cord injury following mechanical insults. In our previous studies using similar preparation, we have found that controlled compression can produce predictable neurophysiological and anatomical deficits, such as action potential and membrane potential losses, and axonal membrane permeability changes.15,17,19,22 In the current study, the elevation of reactive oxygen species following compression has also been characterized. These indicators of physical injury in this model correlated well, which indicates that each individual indicator can reflect the severity of the insults, although combination measurements give a more comprehensive picture.
As in all other in vitro studies involving tissue extraction, the process of separating the spinal cord from live guinea pigs like our model would inevitably cause certain degrees of cell injury and free radical generation. It is clear, however, that such cell damage has been kept at a minimal level in our current model, indicated mainly by minimal production of ROS and lipid peroxidation (Figures 3 and 4). Further, the ROS level measured in the control-uninjured group in our study is comparable with that of healthy tissue of other effective in vivo models.20,21
Our measurements also indicate that our in vitro experimental condition was sufficient to sustain the functional integrity of the extracted tissue. For example, electrophysiological recording, using double sucrose-gap chamber, showed that the isolated spinal cord tissue, when no deliberate compression was performed, was functionally competent by the end of the maximal experimental period (4 h) (Figure 2). The electrophysiological assessment was also consistent with other types of measurements on uninjured cord which indicate that the free radical production and LPO remain low during the entire period of the experiments. This was evidenced in Figure 3, where minimal ROS production and related damage up to 4 h after spinal cord extraction was displayed. This is also in agreement with our previous histology and electrophysiology studies.15,17,19,22 Using the double sucrose gap recording device15,16,17,19 and an HRP-exclusion assay,17,18,23 we have demonstrated that spinal cord strips extracted by the same procedure used in this study maintained cellular membrane integrity, as well as normal electrophysiological functions. We believe this is due to the combination of cold Kreb's solution perfusion, fast surgery procedure, and subsequent sufficient perfusion of Kreb's at physiological temperature.17,18 In summary, in this current in vitro model, the isolation surgery produced minimal damage, which makes it possible for the tissue to show the increase of ROS caused by deliberate compression injury and be sensitive to treatment.
The noted feature of this current model is the ability of the isolated cord to show significant elevation of free radicals after a compression injury, indicated by a marked increase in the ROS production and lipid peroxidation which is comparable to other in vivo studies.21 This demonstrates that the isolated spinal cord in our model retained the ability to produce significant levels of ROS in the injured tissue. This elevation was produced in the absence of blood cells, such as neutrophils, which are considered to be a major source of free radicals24 and responsible for subsequent cell damage25 in in vivo studies. This also indicates that neurons and/or glia cells are capable of producing significant levels of ROS in response to mechanical insults in our model.
The current investigation clearly shows that the gray matter has higher fluorescence intensity than white matter as a result of mechanical injury in our model. There are several possible explanations for this phenomenon. One is that the gray matter, laden with neuronal cell bodies, has more machinery which is capable of producing ROS in higher quantity than white matter containing mainly neuronal axons. An alternative explanation is that perhaps the astrocytes/oligodendrocytes in the white matter have a higher capacity for scavenging/neutralizing ROS. Another possibility could be that the gray matter is more sensitive than white matter to compression in our model. This is consistent with the observation that in a rodent contusion spinal cord injury model, a central core lesion area was surrounded by a rim of spared white matter.26 This could be due to the location of the gray matter vs the white matter27 as well as the fact that the cell bodies are structurally different than axons and could possibly be injured more easily.
Lastly, we have shown that the combination treatment of ascorbic acid and hypothermia can significantly reduce ROS production and lipid peroxidation in our model, as has been shown in some other cell culture studies and whole animal studies.28,29 This indicates that the treatment we applied through the perfusion solution could successfully penetrate the tissue and reach the injury site. This suggests that this model can be used as an effective means to search for effective pharmaceutical and physical interventions that can significantly inhibit the production of ROS and related tissue damage.
Methods to detect free radical formation and lipid peroxidation
There are a number of methods available for quantifying the generation of ROS and their adverse effect.30 The most commonly used method is the detection of thiobarbituric acid reactive substances (TBARS), consisting mainly of malondialdehyde (MDA).31 TBARS determination is an indirect method which measures aldehydes. However, aldehydes can also be generated from peroxides during heating, a necessary stage of the assay which can obviously introduce errors. Consequently, an overestimation of MDA as a result of injury is possible. Because of this disadvantage, we used a lipid hydroperoxide assay kit to detect LPO in the current study. The current assay measures hydroperoxides directly, which is expected to be more accurate than TBARS. The result using this method demonstrates that SCI induced by compression led to increased LPO, which is consistent with the results obtained using the other two methods in the current study (fluorescent microscopy and flow cytometry). This indicates that the LPO assay is suitable and effective in the current model.
Although enhanced LPO after spinal cord injury has been repeatedly demonstrated in in vivo and tissue culture studies, the time courses and values of LPO elevation varies widely among different investigations.20,21,32 For example, the LPO values range from about 6–10 nmol/100 mg20,21 to 158 nmol/100 mg32 in the control. One possible explanation of such a phenomenon is the inability to standardize the experimental condition in these in vivo studies. One advantage of the current study is the ability to accurately control the experimental condition, which enables us to produce highly repeatable results. Considering the fact that there is no consistent time course data in other in vivo studies, it is important for us to establish the time course of ROS elevation for the current model. Based on our data, the elevation of LPO reaches the peak at 1 h following injury and declines thereafter, although the level of LPO remains significantly elevated up to 4 h post-injury.
One of the challenges of using flow cytometry to detect free radicals in the current model is the preparation of single-cell suspensions. Dissociation is the first step in the process of obtaining single-cell suspension for flow cytometry examination. The methods currently available to dissociate cells are mechanical, enzymatic, and a combination of these two.14 In this study, we have found that for flow cytometry, the combination method was the most effective, rendering maximal dissociated single cells without causing significant cell damage. Using this dissociation method, we were able to produce cells appropriate for flow cytometry examination, and obtain the information of ROS elevation similar to that using the other two methods.
HE has been used as an intercellular superoxide indicator in flow cytometry and confocal or fluorescent microscopy.13,33,34,35 As a cell-permeant fluorescent dye, HE can enter cell plasma membranes freely in single-cell suspensions34 or individual neurons in culture and in brain slices.35 For in vivo animal studies, HE has been shown to reach the injury site through blood circulation.36 The current study shows that HE is capable of penetrating the spinal cord tissue in the absence of blood flow, by direct diffusion. This demonstrates the versatility of this dye in different biological samples.
By using three complimentary methods with different mechanisms, we have overcome some of the shortcomings that each individual method has. For example, although the biochemical technique (LPO) is useful in measuring the overall level of tissue lipid peroxidation, it is not appropriate for the detection of oxidant damage inside the individual cells. Flow cytometry, on the other hand, gives an estimation of total production of ROS by the summation of fluorescent intensities from each individual cell, while excluding ROS in the extracellular space. Therefore, the combination of LPO and flow cytometry offers a more complete picture in terms of the production and effect of ROS of total tissue as well as intracellular and extracellular compartments in the current isolated spinal cord injury model.
By comparing the data from flow cytometry and LPO, we have found a difference between flow cytometry measurement of O2− and biochemical measurement of LPO. For example, at 1 h following compression, there was a 209% increase of LPO detected by biochemical method and only a 33% increase in O2− generation as detected by flow cytometry. This likely reflects that these two methods focus on different cellular compartments. The LPO assay is a cumulative measurement of the products of oxidative reaction and both intracellular and extracellular lipid peroxides were included. O2− generation determined by flow cytometry measures the intracellular O2− level at different time points. Since the life span of O2− is short, there is much less accumulation of it. This is probably the reason that measured O2− is lower than that of LPO. Furthermore, O2− is the only one of many contributors of LPO. Other ROS could also induce LPO.
Inhibition of free radical formation and lipid peroxidation
The central nervous system has a relatively high susceptibility to ROS and is difficult to treat. One of the main reasons for this is that many antioxidants in the blood stream do not easily cross the blood-brain barrier. However, ascorbate can be taken up from the blood into cerebrospinal fluid (CSF) through active, stereospecific, Na+-dependent-transport at the choroid plexus.29 Ascorbate can also enter the ECF by carrier-mediated uptake and by simple diffusion across brain capillaries at the blood-brain barrier.29,37 Ascorbic acid has the potential to protect both cytosolic and membrane components of cells from oxidant damage.38 For example, ascorbic acid scavenges free radical species in the cytosol and reduces the α-tocopheroxyl radical to α-tocopherol for cellular membranes.38 As one of the potential treatments, hypothermia has been shown in numerous animal and clinical studies to attenuate neuronal damage and dysfunction after mechanical injury and ischemia in the spinal cord.28 The mechanisms proposed to account for the protection produced by hypothermia include reducing metabolic rate of oxygen consumption, attenuating excitotoxicity and decreasing generation of ROS.32,39,40,41,42,43 Since ascorbate and hypothermia act on different mechanisms, it is not surprising that ascorbic acid and hypothermia act synergistically to reduce ROS production and related injury in our current study. In agreement with our finding, a recent study shows that antagonism of free radicals can increase the neuroprotective efficacy of hypothermia.44 Furthermore, other successful combination treatments have also been reported. For example, the combination of riluzole (a glutamate release inhibitor) and methylprednisolone was more effective in improving measures of oxidative stress following traumatic spinal cord injury than each applied separately.45 This and many other reports suggest that the combination method is a good strategy to effectively suppress ROS and other secondary injuries in the spinal cord and other CNS trauma.
In conclusion, this study shows that this in vitro model has an advantage of controlling experimental conditions and at the same time mimicking the ROS pathology similar to an in vivo model. Therefore, the current method constitutes a suitable model which can be used to examine the effects of antioxidants for the treatment of spinal cord injury. The study has also shown that treatments with a combination of ascorbic acid and hypothermia inhibit LPO production and decrease superoxide level. We have also demonstrated that flow cytometry can be effectively used to detect the formation of superoxide in an in vitro model of spinal cord injury.
References
Amar AP, Levy ML . Pathogenesis and pharmacological strategies for mitigating secondary damage in acute spinal cord injury Neurosurgery 1999 44: 1027–1039
Blight AR . Morphometric analysis of a model of spinal cord injury in guinea pigs, with behavioral evidence of delayed secondary pathology J Neurol Sci 1991 103: 156–171
Faden AI . Experimental neurobiology of central nervous system trauma Crit Rev Neurobiol 1993 7: 175–186
Faden AI . Comment: need for standardization of animal models of spinal cord injury J Neurotrauma 1992 9: 169–170
Tator CH . Update on the pathophysiology and pathology of acute spinal cord injury Brain Pathol 1995 5: 407–413
Hall ED . Free radicals and CNS injury Crit Care Clin 1989 5: 793–805
Lewen A, Matz P, Chan PH . Free radical pathways in CNS injury J Neurotrauma 2000 17: 871–890
Povlishock JT, Kontos HA . The role of oxygen radicals in the pathobiology of traumatic brain injury Human Cell 1992 5: 345–353
Liu D et al. Superoxide production after spinal injury detected by microperfusion of cytochrome c Free Rad Biol Med 1998 25: 298–304
Springer JE et al. 4-hydroxynonenal, a lipid peroxidation product, rapidly accumulates following traumatic spinal cord injury and inhibits glutamate uptake J Neurochem 1997 68: 2469–2476
Hall ED . Inhibition of lipid peroxidation in central nervous system trauma and ischemia J Neurol Sci 1995 134: Suppl S79–S83
Juurlink BH, Paterson PG . Review of oxidative stress in brain and spinal cord injury: suggestions for pharmacological and nutritional management strategies J Spinal Cord Med 1998 21: 309–334
Robinson JP . Handbook of flow cytometry methods New York: Wiley, Liss 1993
Grogan WM, Collins JM . Guide to flow cytometry methods New York: Marcel Dekker 1990
Shi R, Blight AR . Compression injury of mammalian spinal cord in vitro and the dynamics of action potential conduction failure J Neurophysiol 1996 76: 1572–1580
Shi R, Blight AR . Differential effects of low and high concentrations of 4-aminopyridine on axonal conduction in normal and injured spinal cord Neuroscience 1997 77: 553–562
Shi R et al. Control of membrane sealing in injured mammalian spinal cord axons J Neurophysiol 2000 84: 1763–1769
Shi R, Pryor JD . Temperature dependence of membrane sealing following transection in mammalian spinal cord axons Neuroscience 2000 98: 157–166
Shi R, Borgens RB . Acute repair of crushed guinea pig spinal cord by polyethylene glycol J Neurophysiol 1999 81: 2406–2414
Kaptanoglu E et al. Effect of mexiletine on lipid peroxidation and early ultrastructural findings in experimental spinal cord injury J Neurosurg 1999 91: Suppl 2 200–204
Iwasa K, Itata T, Fukuzawa K . Protective effect of vitamin E on spinal cord injury by compression and concurrent lipid peroxidation Free Rad Biol Med 1989 6: 599–606
Shi R, Kelly TM, Blight AR . Conduction block in acute and chronic spinal cord injury: Different dose-response characteristics for reversal by 4-Aminopyridine Exp Neurol 1997 148: 495–501
Asano T, Shi R, Blight AR . Horseradish peroxidase used to examine the distribution of axonal damage in spinal cord compression injury in vitro J Neurotrauma 1995 12: 993
Taoka Y et al. Role of neutrophil elastase in compression-induced spinal cord injury in rats Brain Res 1998 799: 264–269
Blight AR . Macrophages and inflammatory damage in spinal cord injury J Neurotrauma 1992 9: Suppl S83–S91
Ma M et al. Behavioral and histological outcomes following graded spinal cord contusion injury in the C57B1/6 mouse Exp Neurol 2001 169: 239–254
Shi R, Borgens RB . Anatomic repair of nerve membrane in crushed mammalian spinal cord with Polyethylene Glycol J Neurocytol 2000 29: 633–644
Martinez-Arizala A, Green BA . Hypothermia in spinal cord injury J Neurotrauma 1992 9: Suppl 2 S497–S505
Rice ME . Ascorbate regulation and its neuroprotective role in the brain Trends Neurosci 2000 23: 209–216
de Zwart LL et al. Biomarkers of free radical damage applications in experimental animals and in humans Free Rad Biol Med 1999 26: 202–226
Ohkawa H, Ohishi N, Yagi K . Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction Anal Biochem 1979 95: 351–358
Tuzgen S et al. The effect of epidural cooling on lipid peroxidation after experimental spinal cord injury Spinal Cord 1998 36: 654–657
Rothe G, Valet G . Flow cytometric analysis of respiratory burst activity in phagocytes with hydroethidine and 2′,7′-dichlorofluorescence J Leukoc Biol 1990 47: 440–448
Carter WO, Narayanan PK, Robinson JP . Intracellular hydrogen peroxide and superoxide anion detection in endothelial cells J Leukoc Biol 1994 55: 253–258
Bindokas VP et al. Superoxide production in rat hippocampal neurons: selective imaging with hydroethidine J Neurosci 1996 16: 1324–1336
Chan PH et al. Overexpression of SOD1 in transgenic rats protects vulnerable neurons against ischemic damage after global cerebral ischemia and reperfusion J Neurosci 1998 18: 8292–8299
Lam DKC, Daniel PM . The influx of ascorbic acid into the rat's brain Q J Exp Physiol 1986 71: 483–489
May JM . Is ascorbic acid an antioxidant for the plasma membrane? FASEB J 1999 13: 995–1006
Colbourne F, Sutherland G, Corbett D . Postischemic hypothermia. A critical appraisal with implications for clinical treatment Mol Neurobiol 1997 14: 171–201
Dietrich WD et al. Brain damage and temperature: cellular and molecular mechanisms Adv Neurol 1996 71: 177–194
Farooque M et al. Effects of moderate hypothermia on extracellular lactic acid and amino acids after severe compression injury of rat spinal cord J Neurotrauma 1997 14: 63–69
Globus MY et al. Glutamate release and free radical production following brain injury: effects of post-traumatic hypothermia J Neurochem 1995 65: 1704–1711
Schwab S et al. Moderate hypothermia in the treatment of patients with severe middle cerebral artery infarction Stroke 1998 29: 2461–2466
Schmid-Elsaesser R et al. Combination drug therapy and mild hypothermia: a promising treatment strategy for reversible, focal cerebral ischemia Stroke 1999 30: 1891–1899
Mu X, Azbill RD, Springer JE . Riluzole improves measures of oxidative stress following traumatic spinal cord injury Brain Res 2000 870: 66–72
Acknowledgements
This study was supported by funding from Purdue University, the State of Indiana, and a grant from NIH-NINDS. We thank Dr Richard Borgens for his support and encouragement, and Dr Brad Duerstock and Kathryn E Ragheb for their invaluable assistance in the course of this study. We also thank James Whitebone and Phyllis Zickmund for their critical reading of this manuscript.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Luo, J., Li, N., Robinson, J. et al. The increase of reactive oxygen species and their inhibition in an isolated guinea pig spinal cord compression model. Spinal Cord 40, 656–665 (2002). https://doi.org/10.1038/sj.sc.3101363
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101363
Keywords
This article is cited by
-
Anatomical study of the arterial blood supply to the thoracolumbar spinal cord in guinea pig
Anatomical Science International (2015)
-
Pushing the science forward: chitosan nanoparticles and functional repair of CNS tissue after spinal cord injury
Journal of Biological Engineering (2013)
-
The Neuroprotective Ability of Polyethylene Glycol is Affected by Temperature in Ex Vivo Spinal Cord Injury Model
The Journal of Membrane Biology (2013)
-
Microglia inhibition is a target of mild hypothermic treatment after the spinal cord injury
Spinal Cord (2008)
-
Effect of postinjury intravenous or intrathecal methylprednisolone on spinal cord excitatory amino-acid release, nitric oxide generation, PGE2 synthesis, and myeloperoxidase content in a pig model of acute spinal cord injury
Spinal Cord (2006)
