
Abstract
Design: Deficits in trunk control due to spinal cord injury (SCI) lead to slower target-reaching movements of the hand. We investigated whether the movement path is also affected, and whether providing external support for the trunk can abolish the kinematic differences.
Objective: To compare movement trajectories between individuals with SCI and neurologically normal individuals, with and without external trunk support.
Setting: Neural Control/Biomechanics Laboratory, University of Illinois, Chicago, USA.
Methods: Five subjects with levels of injury between C7 and T4 were tested 3–8 years post-injury, and compared with five control subjects. Two targets were employed. Trajectories were recorded by a motion-capture system using infrared emitting markers. Peak speed and path curvature were calculated for the fingertip and for the acromion.
Results: Compared with control subjects, the subjects with SCI exhibited lower peak speed of the fingertip but not of the acromion, and less straight paths for both. When the trunk was supported externally, the difference in fingertip speed persisted. The support abolished the difference in path curvature for the fingertip but accentuated that for the acromion.
Conclusion: The slower hand movements of individuals with SCI are not simply time-scaled versions of those of normal subjects, and the provision of trunk support does not erase the kinematic differences between the reaching movements of the two groups.
Similar content being viewed by others

Introduction
Control of the trunk is an important component of the control of arm movements performed by seated, neurologically normal (NN) subjects.1,2,3 Indeed, prior to initiation of reaching movements of the hand to targets in different directions, substantial anticipatory activity of either the erector spinae or the abdominal muscles is observed depending on target direction.4 Individuals with spinal cord injury (SCI) who have lost control of the erector spinae and abdominal muscles cannot employ such anticipatory activity in conjunction with arm movements. A limited degree of trunk stabilization can be provided, however, by the innervated latissimus dorsi and trapezius muscles.5,6
Little attention has been paid to the effect of the limitations in trunk control on the kinematics of arm movements. Reaching movements performed by SCI subjects have been reported to be considerably slower than those of NN subjects despite the intact innervation of arm and pectoral-girdle muscles and despite the availability of a backrest.7 The slowness is presumably a learned adaptation that reduces the disturbing forces exerted on the trunk by the motion of the arm, thereby diminishing the need for active trunk stabilization. Other than the reported difference in speed, however, there do not appear to be any reports of kinematic comparisons of reaching movements between NN and SCI individuals, which is a gap we attempt to fill.
The first question to be addressed is whether the target-reaching arm movements of SCI subjects are simply a slowed-down version of the movements of NN subjects, or they represent an altogether different pattern of coordination between the trunk and the arm. If the former were the case, then the movement path in space of any point on the arm, scapula, or trunk should be similar for NN and SCI subjects, though the path may be traversed at different speeds. As a first step toward answering this question we compare in the present report the movements of the hand and of the acromion between the two groups of subjects. Because the trunk motion in NN subjects is small when the hand moves to a ‘near’ target – defined as one that lies within arm's length, and is larger for a ‘far’ target – defined as lying beyond arm's length,1 we employ a ‘near’ as well as a ‘far’ target for these comparisons.
The second question to be addressed is whether kinematic differences, including the known difference in speed, can be mitigated by providing stable support to the trunk through strapping it to a backrest. While such support makes movements to far targets impossible, for near targets it should resist the disturbing forces arising from arm acceleration as well as deceleration, obviating the need for active trunk stabilization.8 If this is the case then the external support should abolish any kinematic differences of the hand and acromion movements between NN and SCI individuals.
An anecdotally observed feature of reaching movements by SCI subjects is that they find it more difficult to maintain trunk stability when the arm is held in an outstretched position than when the arm reaches out for a brief instant before returning. Our third question, therefore, is whether the kinematics are different between reach-and-pause and reach-and-immediately-return movements of the arm.
Methods
The studies were approved by the Institutional Review Board. Five SCI subjects and five NN subjects participated in the study after giving informed consent. Among the SCI subjects, who were tested 3–8 years post-injury, the levels of injury (and ASIA scores) were: C7 (B), T1 (B), T2 (A), T4 (B), and T4 (B). None had spasticity that could interfere with transfers or with sitting, nor was any impairment of hand function apparent. SCI subjects ranged in age from 23 to 35 (mean=25.8), and NN subjects from 23 to 30 (mean=26.4) years. All subjects were right handed and were males, except for one female SCI subject.
The subject sat on a padded bench, keeping the left hand immobile on the abdomen. From an initial position of the right hand on the right thigh, and the trunk as upright as possible, the subject, on hearing a beep sound, reached with the right hand to touch a target placed in the parasagittal plane through the right shoulder. Two target positions were employed, at distances from the shoulder of 80% (‘near target’) and 110% (‘far target’) arm's length. Arm's length was defined in full extension as the distance from the acromion to the tip of the third finger. The far target could not be placed any further away without making the task impossible for the SCI subjects. Either target was placed in a direction 45° above the horizontal line through the right shoulder. Thus, to reach either target the hand had to move upward and somewhat anteriorly, which in NN subjects is associated with considerable anticipatory paraspinal muscle activity.4
With the wrist splinted, the NN or SCI subject was instructed to reach for the designated target as fast as possible without losing balance; accuracy was not emphasized. Ten trials were performed to the near target without any trunk support, and 10 trials with the chest strapped to a backrest. The backrest, which was in the form of a grid, was affixed to the bench on which the subject sat. The strap was approximately 10 cm wide and the top of it was applied snugly to the chest at nipple level and wrapped around and through the backrest. This set-up allowed virtually no anterior–posterior or lateral motion. The trunk-support trials were performed last. No support was used with the far target, for which 2 NN and 3 SCI subjects performed 10 trials each, and the others did 20 trials; this inequality stemmed from a decision during the study to give more emphasis to the far-target trials. Half of the above-mentioned trials were performed with the instruction to come back to the initial position immediately after touching the target (reach-and-return), and the other half with the instruction to hold the finger in contact with the target until hearing a second beep, which sounded 0.5 s after target contact (reach-and-pause). Much longer pause periods were not feasible with SCI subjects because of the threat to their balance. Throughout the experimental session one of the investigators stood behind the subject, ready to provide support if the trunk became unstable. With the experimental protocol chosen, this occurred rarely; such trials were discarded.
The target was a small metal plate (3×2 cm), connected to a contact-detector circuit whose output was sampled (200/s) by an A/D converter and stored as a data file. A separate file was generated for the kinematic data using a Selspot motion-capture system with active, infrared LED markers and two cameras. The data consisted of the 3-dimensional positions of each of the markers, sampled at 200/s for a duration of 3 s. Pairs of markers were affixed with Velcro straps to the forearm, upper arm, thorax, and sacrum, and a single marker was affixed with tape at the acromion. Because individuals can use different parts of the trunk, as well as the scapula, in rather complex ways,6 we chose to focus on the motion of the acromion, which reflects the net kinematic effect of trunk and scapular motions.
Fingertip position was calculated based on the locations of the two forearm markers and the measured fixed distance between one of them and the fingertip. The fingertip and acromion position data were smoothed by a least-squares digital filter – Savitzky-Golay, 3rd degree polynomial fit to 10 neighboring samples on each side – which also yielded the velocity values.9 An index of curvature of the path from the initial position to target contact was defined as the ratio of the length of the curved path to the straight-line distance between the initial and final positions, both computed in 3-dimensional space. This measure, which equals 1.00 for a straight-line path and 1.57 for a semicircular path, is identical to the ‘length index’ defined by Cirstea and Levin.10 The peak speed and the curvature index for the fingertip and for the acromion comprised four kinematic descriptors. The acromion's motion was described by two additional variables: displacement, ie, straight-line distance moved from initial position to target contact, and the direction of this straight line in the sagittal plane (0°=anterior, 90°=upward, 180°=posterior). We thus examined a total of six dependent variables.
Results
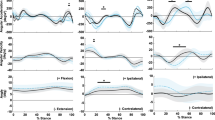
Figure 1 shows, from initial position to target contact, the sagittal-plane paths of the fingertip and acromion (upper panels), and their speeds (lower panels), for three representative reach-and-pause movements of an NN subject. The fingertip paths are curved in all instances. Trunk motion results in the acromion moving anteriorly and upward for the far target (Figure 1A), but mostly upward for the near target (Figure 1B,C). Figure 2 depicts analogous data for an SCI individual. The acromion motion is less anteriorly directed when reaching to the far target (compare Figures 2A and 1A), and the speed profiles are more complex. For the near target, trunk support renders the fingertip path less curved but the acromion path more curved (compare Figures 2B and C).

Records from three reach-and-pause movement trials performed by a neurologically normal individual. (A) depicts motions to the far target, and (B) and (C) to the near target, without and with the trunk strapped to a backrest. Upper panels show the sagittal-plane paths of the fingertip (f) and the acromion (a) from initial position to the moment of target contact, as seen from the subject's right. Solid-line arrows in (A) indicate direction of motion. The initial position of the distal segment (elbow–fingertip, e–f) is shown, as is its position at target contact. Lower panels depict the corresponding speed profiles. Time zero corresponds to the auditory ‘go’ signal

Records from three reach-and-pause movement trials performed by an individual with spinal cord lesion at T2. The format is the same as in Figure 1, but the time and speed scales are different
Each of the six dependent variables described in Methods was subjected to Anova, treating each trial as independent. The criterion for significance was set at P<0.05. For the far-target data, Anovas with two factors (NN/SCI, return/pause) failed to find significant differences between reach-and-return and reach-and-pause movements for any of the six dependent variables. The same was true for the near-target data, using a 3-factor Anova (additional factor: no support/trunk support). For subsequent analyses we pooled the reach-and-return and reach-and-pause data trials.
Table 1 gives the means and standard deviations of the dependent variables in the various conditions for the NN and SCI groups. Focusing first on the column for the far target, for which t-tests were used to compare the two groups of subjects and significant differences are marked by an asterisk (*), it is seen that the SCI subjects' peak fingertip speed is much less than that of NN subjects, and the path is less straight. For the acromion, too, the path is less straight, but the peak speed is too variable to be significantly different. The acromion displacement is less for SCI individuals, and its direction is remarkably different between the two groups, confirming the impression given by Figures 1A and 2A.
For the near target, Anovas were performed with two factors (NN/SCI, no support/trunk support), whose results are also given in Table 1. Significant main effects of group and support condition are indicated by * and } respectively. Fingertip peak speed is again lower for SCI subjects compared to NN subjects, and the provision of trunk support has no significant effect on it. The fingertip path curvature is greater for SCI subjects, and trunk support has a main effect: the support reduces the curvature index. As suggested by the significant interaction effect and confirmed by post-hoc t-tests, the difference in path curvature between the two groups of subjects is significant only in the absence of trunk support; its significance vanishes when the trunk is supported. Table 1 also confirms the impression from Figure 2 (B,C) that while trunk support reduces the curvature of the fingertip path in SCI subjects, it increases significantly the curvature of the acromion's path. In contrast to the situation with the far target, the direction of acromion motion is not significantly different between the groups, and its displacement is smaller in NN subjects.
Discussion
We found significant differences in acromion and hand kinematics between NN and SCI individuals. In addition to confirming the difference in hand speed,7 we found both the fingertip and acromion paths to be significantly less straight in SCI individuals. For the far target the acromion displacement in SCI individuals was directed mostly vertically upwards rather than anteriorly and upwards as in NN individuals, and was smaller in magnitude. For the near target, however, the direction was mostly upward for both groups but the magnitude was smaller for NN individuals. Presumably, the upward displacement of the acromion was a reflection of upper thoracic extension, which could contribute to the reach distance since the targets were above the shoulder level. The finding that the acromion displacement in SCI individuals was always nearly upwards was to be expected from the individuals' inability to control a flexed trunk. But we did not expect that the magnitude of the displacement would not be modulated as much with target position as well as support condition as it was for NN individuals.
If the slower movement of SCI individuals reflected simply a time-scaled version of the movement of NN individuals, then one would have expected to find correspondingly slower motion of the acromion as well, and no differences in fingertip or acromion paths between SCI and NN individuals. On the contrary, we found that the peak acromion speed was not significantly different between the two groups, whereas there were significant differences in the paths. The time course of the acromion speed, too, was highly variable, even from trial to trial, but we did not analyze this phenomenon. From our analyses we can conclude, for the near as well as the far target, that the movements of SCI individuals are not simply a slowed version of the movements of NN individuals, but rather represent a different pattern of coordination of the trunk, scapula and arm.
We investigated whether the kinematic differences between the NN and SCI subjects are obliterated when the trunk is strapped to the backrest. We found that strapping the trunk did abolish the difference in fingertip path curvature between the two groups of subjects. Nevertheless, other significant differences persisted in the presence of trunk support: lower fingertip speed, less straight acromion path, and greater acromion displacement. The persistence of the speed difference when the back was supported is inconsistent with the idea that SCI individuals choose a slower speed only when there is risk of trunk instability due to the forces applied by the moving arm. Although slower speed may well have been chosen to avoid trunk instability, it continued to be chosen even when not necessary in the presence of trunk support. The precise manner of scapular and other motions whereby trunk support induces a more straight fingertip path together with a more curved acromion path remains to be elucidated.
Faced with a deficit in trunk control the individuals with SCI often resort to stabilizing the trunk by counterbalancing the motion of the reaching arm with an opposite motion of the contralateral arm.11 We noted that when this strategy is not feasible, such individuals try to avoid holding the arm in an outstretched position where static equilibrium would require paraspinal activity. In particular, SCI individuals were unable to perform reach-and-pause movements without the trunk becoming unstable when the pause duration was much in excess of 0.5 s. Employing a pause duration of 0.5 s for testing the difference between reach-and-pause and reach-and-return movements, we did not find a significant difference in any of the kinematic variables tested.
The characteristics of reaching movements in individuals with paraplegia have the potential of providing information about the functional deficit in trunk control. For example, the level of spinal lesion, which determines the deficit in trunk control, is known to affect the maximum reach distance,11 but it does not necessarily affect other arm movement patterns such as those used for wheelchair propulsion.12 The present study documents some of the differences in arm kinematics in reaching, as a prelude to more extensive studies in larger and more varied groups of SCI subjects. It may also contribute to future investigations of the extent to which the kinematic differences are adaptive.
References
Kaminski TR, Bock C, Gentile AM . The coordination between trunk and arm motion during pointing movements Exp Brain Res 1995 106: 457–466
Dean C, Shepherd R, Adams R . Sitting balance I: trunk-arm coordination and the contribution of the lower limbs during self-paced reaching in sitting Gait Posture 1999 10: 135–146
Pigeon P, Yahia LH, Mitnitski AB, Feldman AG . Superposition of independent units of coordination during pointing movements involving the trunk with and without visual feedback Exp Brain Res 2000 131: 336–349
Tyler AE, Hasan Z . Qualitative discrepancies between trunk muscle activity and dynamic postural requirements at the initiation of reaching movements performed while sitting Exp Brain Res 1995 107: 87–95
Seelen HA, Vuurman EF . Compensatory muscle activity for sitting posture during upper extremity task performance in paraplegic persons Scand J Rehab Med 1991 23: 89–96
Potten YJ et al. Postural muscle responses in the spinal cord injured persons during forward reaching Ergonomics 1999 42: 1200–1215
Do MC, Bouisset S, Moynot C . Are paraplegics handicapped in the execution of a manual task? Ergonomics 1985 28: 1363–1375
Curtis KA, Kindlin CM, Reich KM, White DE . Functional reach in wheelchair users: the effects of trunk and lower extremity stabilization Arch Phys Med Rehabil 1995 76: 360–367
Press WH, Teukolsky SA, Vetterling WT, Flannery BP . Numerical Recipes in Fortran: The Art of Scientific Computing Cambridge: Cambridge University Press 1992 pp 644–649
Cirstea MC, Levin MF . Compensatory strategies for reaching in stroke Brain 2000 123: 940–953
Lynch SM, Leahy P, Barker SP . Reliability of measurements obtained with a modified functional reach test in subjects with spinal cord injury Phys Ther 1998 78: 128–133
Newsam CJ et al. Three dimensional upper extremity motion during manual wheelchair propulsion in men with different levels of spinal cord injury Gait Posture 1999 10: 223–232
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Reft, J., Hasan, Z. Trajectories of target reaching arm movements in individuals with spinal cord injury: Effect of external trunk support. Spinal Cord 40, 186–191 (2002). https://doi.org/10.1038/sj.sc.3101277
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101277
Keywords
This article is cited by
-
Test-retest reliability and validity of the Sitting Balance Measure-Korean in individuals with incomplete spinal cord injury
Spinal Cord (2022)
-
Kinematic Outcome Measures using Target-Reaching Arm Movement in Stroke
Annals of Biomedical Engineering (2017)
-
Adapted sport effect on postural control after spinal cord injury
Spinal Cord (2016)
-
Upper limb kinematics after cervical spinal cord injury: a review
Journal of NeuroEngineering and Rehabilitation (2015)
-
Kinematic characteristics of tenodesis grasp in C6 quadriplegia
Spinal Cord (2013)
