
Abstract
Overt symptoms of Parkinson's disease do not manifest themselves until there is a substantial loss of the dopaminergic nigrostriatal projection. However, as neuroprotective strategies are developed, it will be essential to detect the disease in its preclinical phase. Performance on conditioned reaction time tasks is known to be impaired by extensive 6-hydroxydopamine-induced lesions of the nigrostriatal dopamine pathway. However, the effect of smaller lesions on a reaction time task has not been systematically assessed. We, therefore, used this test to examine behavioral deficits as a function of striatal dopamine loss. When injected at doses that produced striatal DA depletion <50%, 6-hydroxydopamine infused in the medial forebrain bundle produced no reliable impairment in the reaction time task. Higher doses producing ⩾60% DA depletion in the striatum produced a decrease in the percent correct responding throughout the 5 week testing period and akinetic deficits expressed by an increase in delayed responding. In addition, larger DA depletions (⩾95%) profoundly altered motor control with decreases in percent correct responses, increases in delayed responses and increases in reaction time. These results suggest that reaction time may be a relatively sensitive measure of preclinical or subtle deficits, although it might be even more useful in quantitating the severity of depletion once overt deficits or symptoms appear and has the advantage of measuring such deficits over time to follow recovery of function. Furthermore since reaction time deficits required extensive loss of dopamine, these results are consistent with a predominant role of extrasynaptic dopamine in the mediation of relatively skilled motor tasks.
Similar content being viewed by others

Main
The primary neuropathology of Parkinson's disease is the loss of dopamine (DA) neurons within the substantia nigra (SN) and massive depletion of DA in the striatum, the terminal region of the SN. This loss of DA appears to be responsible for the most prominent symptoms of Parkinson's disease. The degree of neurological deficit is related to the loss of striatal DA (Hornykiewicz and Kish 1987). The neurotoxins 6-hydroxydopamine (6-OHDA) and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), used extensively to induce selective loss of DA neurons within the SN, provide animal models that share several of the characteristics of Parkinson's disease (see reviews by Zigmond and Keefe 1997; Jenner and Marsden 1986; Gerlach and Riederer 1996; Przedborski and Jackson-Lewis 1998). In addition, whereas intrastriatal injection of indirect DA agonists induces stereotypy (Costall et al. 1973; Statton and Solomon 1984), 6-OHDA lesions of the striatum block this stereotyped behavior (Price and Fibiger 1974). Finally, chronic administration of DA receptor antagonists produce extrapyramidal effects reminiscent of Parkinson's disease, and this is believed to be due to their action at D2 receptors located in the striatum (Coffin et al. 1989).
Although resting tremor and muscular rigidity are generally not reported in rodents after pharmacological manipulation of the nigrostriatal pathway, deficits in movement initiation and execution have been studied using several tests including a conditioned reaction time task. In this task, animals are typically required to respond in a particular way and within a limited period in order to receive a reward, such as a food pellet. This behavioral paradigm is responsive to pharmacological manipulation of dopaminergic neurotransmission mediated by the D2 subtype of DA receptors (Amalric and Koob 1987, 1989; Amalric et al. 1993, 1995; Smith et al. 2000). For example, we have shown that low dose blockade of D2 receptors, but not D1 or D3 receptors, decreased correct responses in the conditioned reaction time task, increased delayed responses, and lengthened reaction time in a manner suggestive of dysfunctions in movement initiation (Amalric et al. 1993; Smith et al. 2000). Moreover, deficits in reaction time have also been reported in Parkinson's disease (Evarts et al. 1981; Gauntlett-Gilbert and Brown 1998; Berry et al. 1999). These deficits appear to be mediated by the nigrostriatal dopaminergic pathway, as 6-OHDA-induced loss of SN neurons and striatal DA, and not accumbal DA, produces impairments in this task (Amalric and Koob 1987), and intrastriatal infusion of the DA receptor antagonist haloperidol has a comparable effect (Amalric and Koob 1989).
Previous experiments have examined the effect of large 6-OHDA-induced lesions on performance in a simple and choice reaction time task. Because of the debilitating effects of bilateral lesions, the majority of these studies examined the effect of unilateral lesions on performance in the reaction time task. Massive unilateral lesions of the nigrostriatal pathway (⩾95% loss of striatal DA) produced unilateral deficits in movement initiation, which had not recovered two months later. The deficits were characterized by an increase in the reaction time on the side contralateral to the lesion and a preferential response bias ipsilateral to the lesion (Carli et al. 1985, 1989; Brown and Robbins 1989, 1991; Phillips and Brown 1999). In the few cases in which bilateral lesions of the nigrostriatal pathway have been examined, profound deficits in the reaction time task were observed, and included lengthened reaction times and decreases in the percent correct responses (Amalric and Koob 1987, 1989; Moukhles et al. 1994). An increase in the number of delayed and premature responses also was observed, suggesting a disruption in cognitive as well as motor function. Deficits in the reaction time task following bilateral 6-OHDA lesions appeared after a 70% depletion of striatal DA, were present one week post-lesion, and persisted for at least three months post-lesion (Moukhles et al. 1994).
The effects of smaller lesions have not been systematically assessed. However, the ability to detect deficits prior to a majority loss of striatal DA would be quite useful. Recent evidence shows that several trophic factors are neuroprotective in animal models of Parkinson's disease when these factors are administered either before or after appreciable loss of striatal DA and SN neurons (Choi-Lundberg et al. 1997, 1998; Rosenblad et al. 1998; Connor et al. 1999; Kozlowski et al. 2000). Should these or other treatments prove to be clinically efficacious, it will be essential to develop neurological tests that detect nigrostriatal degeneration in the “preclinical” phase of Parkinson's disease so that neuroprotective strategies can be used to delay or even prevent the appearance of more disruptive functional deficits. Therefore, in the present study the sensitivity of the conditioned reaction time task to striatal DA loss was examined in 6-OHDA–lesioned rats.
MATERIALS AND METHODS
Subjects
Twenty four male Wistar rats (Beckman, The Scripps Research Institute, La Jolla, CA), weighing 120–150 g at the start of the experiment, were housed in groups of three and maintained on a reverse 12-h light/dark cycle with lights on at 10 P.M. Behavioral measurements were conducted during the animals’ light cycle between the hours of 7 and 10 A.M., 5 days a week. Rats were initially food deprived for 24 h at the start of training and subsequently food restricted to 15–17 g of food (Harlan Teklad Laboratories, Bartonville, IL) per day for the duration of the experiment to maintain them at 80–85% of their free food body weight. Water was freely available throughout the experiment. All procedures were in strict accordance with the guidelines for the NIH Care and Use of Laboratory Animals and approved by the Institutional Animal Care and Use Committee of The Scripps Research Institute.
Training Procedure
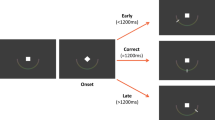
Experiments were conducted in standard experimental chambers (29 cm l × 24 cm w × 19.5 cm h; Coulbourn Instruments, Allentown, PA) placed in sound attenuated cubicles. A retractable lever (BRS/LVE), located 4 cm above the grid floor and 9 cm below the cue light (0.5 cm diameter), was extended immediately after the animals were placed in the experimental chambers. After completion of a successful trial, the food pellet was delivered to the food trough in less than 1 s. The temporal resolution of the instrumental setup was 10 msec. Animals were initially trained to press the lever for a 45-mg food pellet (P.J. Noyes Company, Inc., Lancaster, NH) on a schedule that provided one food pellet for every lever press (fixed ratio-1 reinforcement schedule). After the rats successfully responded for more than 100 pellets, they were trained to hold down the lever until a conditioned stimulus (CS) was presented (light cue above the lever). To receive a food pellet during this phase of training, rats had to release the lever within 1 s after the onset of the CS. The time between the lever press and the onset of the light was initially set to 50 msec and was increased by 50 msec after every five consecutive correct trials. Each session ended after 200 trials. When the rats had been trained to hold down the lever for 1.25 s and received reinforcement with 50% accuracy, the interval between the lever press and the onset of the CS was randomized between four time intervals (250, 500, 750 and 1000 msec). The initial restriction time of 1 s was decreased by 50 msec increments to 700 msec. Each session ended after 100 trials, which animals typically achieved within 10–15 min during the pre-lesion testing period. Correct responses were those in which the rats released the lever within the 700-msec restriction time. Incorrect responses were divided into two categories. If the lever was released prior to the presentation of the CS it was recorded as an incorrect response and termed a premature response. Similarly, if the lever was released outside of the 700-msec restriction time, it was recorded as an incorrect response and was termed a delayed response. Reaction time was measured between the presentation of the CS and the release of the lever.
Bilateral Lesioning of Medial Forebrain Bundle (MFB)
After rats successfully completed at least 50% of the trials for five consecutive days, they received 2 μl of either 6-OHDA hydrobromide (0.25, 0.5, 1, 2, or 4 μg free base; Sigma Chemicals) or vehicle (0.02 mg/ml ascorbic acid in 0.9% saline) bilaterally into the MFB. The coordinates were 4 mm posterior to bregma, ± 1.8 mm from the midline and 7.6 mm ventral from skull. Thirty minutes prior to surgery rats received pargyline (25 mg/kg i.p.). Infusions of 6-OHDA were made under halothane anesthesia with a 30 gauge bilateral cannula and a Harvard syringe pump (model 975) delivering the neurotoxin at 0.3 μl/min. The cannula remained in place for 5 min after cessation of infusion to allow for diffusion of 6-OHDA. After surgery rats were given subcutaneous Ringer's solution and allowed to recover for seven days. During the recovery period, two rats that had received 4 μg 6-OHDA had to be fed by oral gavage. These rats received 3 ml of Sustacal supplemented with 2 g of sucrose by oral gavage 3 times a day, and had free access to laboratory rat chow that had been mashed with Sustacal during the 7-day recovery period. Behavioral testing resumed on day 8 and the 5-day a week testing schedule continued for five additional weeks.
Neurochemical Assay
At the end of the 5-week post-lesion testing period, rats were sacrificed and their brains removed. The following brain regions taken from different anterior levels (according to the atlas of Paxinos and Watson (1986)) were dissected for neurochemical analysis: the prefrontal cortex (A 1320 to A 1120) olfactory tubercle, anterior dorsal striatum (A 1120 to A 1020 at the level of nucleus accumbens), posterior striatum (A1020 to A820) and the amygdala (A 644 to A 540). Tissue samples from the left and right hemispheres were pooled and then were homogenized in 0.1 mM perchloric acid containing 0.2 mM sodium bisulfate. Homogenate was centrifuged for 10 min and the supernatant stored at –80°C until assayed. Tissue samples were assayed for DA, 3,4-dihydroxyphenylacetic acid (DOPAC) and homovanillic acid (HVA) by injecting a 20 μl aliquot of the supernatant onto a Symmetry, C18, 3 μm, 3.9 × 150 mm Waters column. The mobile phase consisted of 50 mM sodium dihydrogen phosphate monohydrate, 0.72 mM sodium octyl sulfate, 0.075 mM ethylenediaminetetraacetic acid disodium salt dihydrate and 16% methanol (v/v), pH 2.7. The mobile phase was pumped through the system at 0.7 ml/min using a Shimadzu LC-10AD pump. Analytes were detected coulometrically using an ESA coulochem 5100A detector with an ESA conditioning (model 5010) and microdialysis cell (model 5014B, E1 = +0.26 V, E2 = + 0.28 V and guard cell = + 0.4 V). The limits of detection (3 times baseline noise) for DA, DOPAC, and HVA were 1 nM, 5 nM and 5 nM, respectively.
Data and Statistical Analysis
The data for each parameter of motor performance were an average of the five sessions in a 1-week period and are presented as mean ± standard error of the mean. The responses (correct, premature, and delayed) are presented as percentage of responses because animals did not always complete the session in the allotted 60-min testing period. To equalize standard deviations across means the data were subjected to logarithmic transformation prior to statistical analysis. The number of correct responses, delayed responses, premature responses, and reaction times were analyzed separately. The effect of a particular lesion size on performance over the 6-week testing period was analyzed for each treatment group using an ANOVA with two within-group factors (number of weeks and number of consecutive sessions), followed by Tukey-Kramer multiple comparison tests. To determine the effect of the lesion size on the parameters of motor performance in the reaction time task, another ANOVA was performed with the lesion size as the between group factor and the five consecutive sessions as the within group factor, followed by post-hoc Tukey-Kramer multiple comparison tests. Tissue levels of DA as a function of lesion size for a given brain region were analyzed by one-way ANOVA followed by post-hoc Tukey-Kramer multiple comparison tests.
RESULTS
6-OHDA–induced Depletion of DA and Metabolites
Tissue levels of DA for the striatum, prefrontal cortex, nucleus accumbens, olfactory tubercle, and the amygdala were measured at the termination of the experiment (Table 1). The most marked deficits in tissue DA levels were seen in the striatum at the three highest doses of 6-OHDA. A 49% depletion of tissue levels of DA was seen in the animals that received 1 μg 6-OHDA (p < .05), 58% in animals receiving 2 μg (p < .05) and a 95% depletion in the animals that received 4 μg (p < .001). A general trend toward decreased tissue levels of DA were also observed in other brain regions with the highest dose of 6-OHDA infused; however, only the nucleus accumbens was significantly affected with a 71% depletion of DA tissue levels (p < .05).
Behavioral Data
There was no significant difference in the pre-lesion baseline values for any parameter of motor performance among the groups. The overall means were 59.4 ± 0.5 correct responses, 30.5 ± 1.0 premature responses, and 9.1 ± 0.7 delayed responses. Incorrect trials during baseline resulted mostly from premature responses (release of lever prior to onset of the CS). The mean reaction times for correct and delayed responses were 332 ± 8 and 1189 ± 12 msec, respectively.
Performance of the sham control animals was stable throughout the six weeks of testing (1 wk pre-lesion and 5 wks post-lesion). Their number of correct and incorrect (premature and delayed) responses did not change during the testing period (30 sessions). In contrast, during the first week of post-lesion testing, animals that sustained the largest lesion (95%) failed to complete the task. These animals failed to consume food pellets in their home cage during the first week post-lesion and their food intake was lower than other groups throughout the post-lesion testing period. They also displayed decreased locomotion as evidenced by their failure to explore their environment when placed on the weighing scale and in the testing chamber. Additionally, during the testing session, these rats would press the lever but had difficulty retrieving the food pellet from the food trough, suggestive of gross motor deficits. As noted above, two rats that received 4 μg 6-OHDA had to be fed by oral gavage one week after lesion. One of these animals had to be eliminated from the study because it never acquired normal eating behavior.
Animals whose striatal DA levels were <40% depleted displayed no differences over the 5-week post-lesion testing period on any parameter of motor performance in the reaction time task. Larger lesions (50-60% DA depletion) resulted in a significant decrease in the percent correct responses throughout the 5-week testing period (p < .05) (Figure 1). However, >90% DA depletion produced a more profound impairment in correct responses with deficits appearing the first week post-lesion and persisting throughout the remaining four weeks of testing (p < .001 weeks 1-4 versus baseline and p < .01 week 5 versus baseline). Additionally, the number of correct responses for this group was significantly lower than the other groups during weeks 1-4 of testing (p < .01 versus all groups) and significantly lower than animals that sustained <40% depletion during week 5 (p < .01).

A representative graph showing the percent correct responses in the reaction time task after five weeks post-lesion as a function of DA depletion. A correct trial is the release of the lever within the 700-msec restriction time after the onset of the cue (n = 4/group). a: p < .05 vs. baseline; b: p < .01 vs. baseline; c: p < .001 vs. baseline; d: p < .01 vs. all groups.
The lesion-induced decrease in the number of correct responses for the larger lesion groups (⩾60%) resulted from an increase in the number of delayed responses. This effect persisted for three weeks post-lesion in the animals with DA depletion around 60% and recovered by the fourth week post-lesion (Figure 2; p < .001 baseline versus weeks 1 and 2; p < .05 versus week 3), whereas no recovery was observed in animals whose lesion was >90% over the entire 5-week period (p < .05 baseline versus weeks 1 and 4; p < .01 baseline versus weeks 2, 3, and 5). This effect was accompanied by an increase in the reaction time of delayed responses in this group of animals (Table 2). There was no significant effect of any dose of 6-OHDA at any time point on premature responding (data not shown).

A representative graph showing the percent delayed responses in the reaction time task at an early (2-wk) and late (5-wk) time points after 6-OHDA infusions in the MFB. A delayed response is the release of the lever after the 700-msec restriction time (n = 4/group). a: p < .001 vs. baseline; b: p < .01 week 2 and 5 post-lesion vs. baseline.
DISCUSSION
We used a conditioned reaction time task to ascertain the level of striatal DA depletion that is necessary before behavioral deficits in this task can be detected. Previous investigators examining the effect of large bilateral depletion of striatal DA observed disruptions in reaction time performance, suggestive of difficulty with movement initiation (Amalric and Koob 1987; Amalric et al. 1995; Moukhles et al. 1994). In agreement, we also observed deficits that were associated with a preponderant loss of DA (⩾60%) in the striatum in comparison to the other brain structures innervated by the MFB. Furthermore, the severity of the deficits and the time course varied with the extent of striatal DA depletion.
No significant behavioral impairment was observed in animals that sustained <40% depletion of striatal DA (in comparison to sham-lesioned animals). Striatal DA depletion of 49% produced a mild impairment in the performance of the reaction time task but this was not manifest until the fourth week post-lesion. At that point the animals showed a 13% decrease in the number of correct responses and a trend toward increased delayed responses, suggesting that animals began to have problems with movement initiation. However, there was no effect of this lesion size on reaction time. A 58% striatal depletion of DA, (85% posterior striatum) displayed a similar decrease in percent correct responses. However, although this was accompanied by a significant increase in the number of delayed responses, there was no lengthening of reaction time, suggesting only mild deficits in movement initiation. Similar impairments had been observed after a 60–70% posterior striatal DA depletion in response to intrastriatal 6-OHDA infusion (Amalric and Koob 1989; Amalric et al. 1995). In those studies, the larger depletions also produced an increase in premature responding, suggesting that cognitive as well as motor dysfunctions had occurred in these animals. However, the large inter-animal variability in the number of premature responses in the present study precluded any significant changes that might have occurred in this parameter.
A 95% DA depletion in the striatum (95% posterior striatum) displayed a 49% decrease in correct responses, 235% increase in delayed responses and a 200% increase in the reaction time of delayed responses. Therefore, these animals had severe impairments in movement initiation. Because of the gross motor deficits produced by this percent depletion of DA, previous studies examining the effect of bilateral lesions in this task restricted their striatal DA percent depletion to 70%. However, unilateral lesions of this magnitude have been examined and were found to produce impairments on the contralateral side of the lesion similar to those observed in the present study (Carli et al. 1985, 1989; Brown and Robbins 1989, 1991; Phillips and Brown 1999). Comparable results were also obtained with antagonists of D2 DA receptors, further establishing the role of this receptor in motor function (Amalric et al. 1993; Smith et al. 2000).
In addition to the differences in the severity of deficits between these groups, the deficits also followed a different time course. The impairment in animals that sustained 49% DA depletion was not observed until the fourth week post-lesion. Previous studies have shown that with sub-maximal striatal depletion of DA, the remaining neurons compensate for the loss with a decrease in the uptake, and an increase in the synthesis, metabolism, and release of DA, thereby maintaining extracellular DA levels (Hefti et al. 1980; Altar et al. 1987; Stricker and Zigmond 1976; Zigmond et al. 1984). Indeed, it has been shown that with less than 80% depletion, the extracellular concentration of DA is maintained in the presence of the remaining terminals (Robinson and Whishaw 1988; Zhang et al. 1988; Abercrombie et al. 1990; Castañeda et al. 1990; Parsons et al. 1991; Robinson et al. 1994). This compensation could account for the lack of a functional deficit during the first three weeks post-lesion; however, if so, these same mechanisms failed to prevent the appearance of deficits in the fourth and fifth week post-lesion. Slow anterograde degeneration of striatal DA terminals could result in the late emergence of behavioral deficits, and delayed degeneration has been observed in the nigrostriatal system in response to transient forebrain ischemia (Volpe et al. 1995). However, striatal fiber degeneration in response to infusion of 6-OHDA into the SN was observed 1–7 days post-lesion without any further degeneration up to 60 days post-lesion (Jeon et al. 1995), and striatal depletion of DA levels is maximal 5–7 days post-lesion in response to infusion of 6-OHDA into the MFB (Smith et al., unpublished results). Alternatively, the difference in the behavioral pattern of the deficits observed after 49 and 59% DA depletion may come from regional differences in the extent of the lesion. Previous studies have shown that a more ventral extension of the lesion in the striatum produced an early increase in premature responding precluding the development of akinetic symptoms (i.e. delayed responding) in the first week of testing (Amalric, unpublished results). The dorso-lateral location of the lesion, in contrary, produced immediate increases in delayed responses (Amalric et al. 1995). It could thus be postulated that these two doses producing similar striatal DA loss (50–60% depletion) did not reached the same striatal areas. Further studies are needed to address this question.
The dysfunction in movement initiation observed in animals that sustained 58% striatal depletion was present one week post-lesion and had recovered by the fourth week post-lesion. Thus, it is possible that the same mechanisms that prevented the appearance of behavioral deficits during the first three weeks post-lesion in the 49% DA depletion animals were responsible for the limited behavioral recovery observed with respect to delayed responses in this group. Some investigators have reported that adaptations in synthesis and release are maximal three days post-lesion (Altar et al. 1987; Zigmond et al. 1984). However, Robinson et al. (1994) have shown that normalization of the extracellular concentration of DA, which is the net result of several processes (synthesis, release, uptake and diffusion), occurs gradually over three to four weeks. In addition, when DA depletion exceeds 85%, compensatory post-synaptic receptor supersensitivity develops several weeks after the lesion in response to reduced extracellular DA levels (Neve et al. 1982, 1984; Zigmond and Stricker 1980). Thus, some combination of increased availability of DA and increased sensitivity to the transmitter may explain the behavioral recovery.
Whereas delayed responses were restored to pre-operative values after 58% DA depletion, deficits in correct responses persisted throughout the 5-week post-lesion period. Indeed, the deficit during the last two weeks of testing was characterized by a non-significant increase in premature responding. It is possible, therefore, that normalized extracellular levels in the presence of supersensitive postsynaptic receptors actually caused an increase in DA neurotransmission above control, leading to behavioral activation. In support of this hypothesis, increases in DA neurotransmission caused by amphetamine have been shown to cause impairments in the reaction time task characterized by decreased correct responses, decreased reaction time, and increased premature responses (Baunez et al. 1995a, 1995b; Döbrössy and Dunnett 1997).
The deficits in the 95% striatal lesion animals were also present seven days post-lesion; however, they were not compensated for during the 5-week post-lesion testing period. Neurochemical analysis showed a 95% decrease in the striatum. Thus, the early and persistent behavioral deficits are consistent with the observation that animals with less than 5–10% of their terminals remaining in the striatum are not able to maintain normal extracellular DA levels even in the presence of enhanced neuronal processes (Robinson and Whishaw 1988; Zhang et al. 1988; Abercrombie et al. 1990; Castañeda et al. 1990; Parsons et al. 1991; Robinson et al. 1994). Furthermore, even in the presence of enhanced neuronal processes and supersensitive postsynaptic receptors, these animals do not recover from their behavioral deficits (Zigmond and Stricker 1973; Creese and Snyder 1979; Marshall 1979, 1984; Neve et al. 1982, 1984). Thus, even though the nigrostriatal DA system shows resiliency in response to massive insult, a critical number of DA nerve terminals appears to be required for behavioral recovery to occur.
The observation that poor behavioral performance in the reaction time task coincides with the inability of the DA system to maintain extracellular DA levels underscores the importance of extrasynaptic transmission. Indeed, previous research has shown that the dopaminergic system actually favors this mode of transmission (Garris et al. 1994; Zigmond 2000). Furthermore, in situations where DA uptake is compromised, as is the case with Parkinson's disease and after 6-OHDA or MPTP neurotoxicity, this mode of transmission is facilitated and may actually play a role in functional recovery (Zigmond et al. 1990; Schneider et al. 1994). First, the extrasynaptic location of the DA transporter (Cerruti et al. 1991; Nirenberg et al. 1996; Hersch et al. 1997) favors leakage of DA to the extrasynaptic compartment, suggesting that it regulates extracellular levels of DA and the distance DA diffuses once it exits the synapse. Second, the extrasynaptic location of DA receptors suggests that this extrasynaptic DA has physiological significance (Yung et al. 1995; Caillé et al. 1996). Moreover, the observation that large deficits in reaction time performance occur at a percent depletion of striatal DA when the system is no longer able to maintain extracellular DA levels, suggests that it plays a role in regulating skilled motor behaviors.
In light of the fact that the behavior in the reaction time paradigm is reinforced with food, it is important to note that the animals that received the highest dose of 6-OHDA decreased their food intake and stopped pressing the lever to initiate the trial. Therefore, their performance could have resulted from a motivational deficit. Indeed, these animals did sustain a significant depletion of DA in limbic structures, particularly the nucleus accumbens, a brain region shown to be involved in reward and motivation. However, 6-OHDA lesions of the nucleus accumbens are reported not to have an effect on performance in the reaction time task (Amalric and Koob 1987). Moreover, we observed that animals in this group had difficulty handling the food pellet and would normally, without much success, attempt to consume the pellet while it was still in the food trough. Salamone et al. (1990) have reported that animals with large DA depleting lesions in the striatum usually have deficits in forelimb use, including deficits in grasp and reach. Thus, although the animals may have been motivated to press the lever for food, failure to successfully retrieve the food pellets caused by gross motor deficits may have prevented them from making further attempts.
Although DA in the striatum plays a major role in motor function, other brain regions have also been implicated in the control of motor function. Specifically, depletion of prefrontal cortex DA has been shown to cause deficits in movement initiation in a simple reaction time task (Hauber et al. 1994) and a role for the frontal cortex has been proposed for deficits in reaction time observed in Parkinson's disease, as well (Berry et al. 1999). In the present study, the animals with the largest striatal lesion sustained a 55% decrease in prefrontal DA, thus contribution of this structure to the impairments in this group of animals cannot be ruled out.
In summary, the present work supports and extends previous work examining the effects of 6-OHDA lesions of the nigrostriatal pathway in a reaction time task. As with previous studies it was observed that a persistent impairment in the task is observed when a moderate depletion (i.e. 60%) of DA tissue level is measured in the striatum. Therefore, the measurement of reaction time may be a useful tool for measuring dysfunctions that might be present during the preclinical stage of Parkinson's disease, but subtle dysfunctions at depletion levels less than 60% remain a challenge for future work.
References
Abercrombie EA, Bonatz AE, Zigmond MJ . (1990): Effects of l-dopa on extracellular dopamine in striatum of normal and 6-hydroxydopamine-treated rats. Brain Res 525: 36–44
Altar CA, Marien MR, Marshall JF . (1987): Time course of adaptations in dopamine biosynthesis, metabolism, and release following nigrostriatal lesions: implications for behavioral recovery from brain injury. J Neurochem 48: 390–399
Amalric M, Koob GF . (1987): Depletion of dopamine in the caudate nucleus but not in nucleus accumbens impairs reaction time performance in rats. J Neurosci 7: 2129–2134
Amalric M, Koob GF . (1989): Dorsal pallidum as a functional motor output of the corpus striatum. Brain Res 483: 389–394
Amalric M, Berhow M, Polis I, Koob GF . (1993): Selective effects of low-dose D2 dopamine receptor antagonism in a reaction time task. Neuropsychopharmacology 8: 195–200
Amalric M, Moukhles H, Nieoullon A, Daszuta A . (1995): Complex deficits on reaction time performance following bilateral intrastriatal 6-OHDA infusion in the rat. Eur J Neurosci 7: 972–980
Baunez C, Nieoullon A, Amalric M . (1995a): In a rat model of parkinsonism, lesions of the subthalamic nucleus reverse increases of reaction time but induce a dramatic premature responding deficit. J Neurosci 10: 6531–6541
Baunez C, Nieoullon A, Amalric M . (1995b): Dopamine and complex sensorimotor integration: further studies in a conditioned motor task in the rat. Neuroscience 65: 375–384
Berry EL, Nicolson RI, Foster JK, Behrmann M, Sagar HJ . (1999): Slowing of reaction time in Parkinson's disease: the involvement of the frontal lobes. Neuropsychologia 37: 787–795
Brown VJ, Robbins TW . (1989): Deficits in response space following unilateral striatal dopamine depletion in the rat. J Neurosci 9: 983–989
Brown VJ, Robbins TW . (1991): Simple and choice reaction time performance following unilateral striatal dopamine depletion in the rat. Impaired motor readiness but preserved response preparation. Brain 114: 513–525
Caillé I, Dumartin B, Bloch B . (1996): Ultrastructural localization of D1 dopamine receptor immunoreactivity in rat striatonigral neurons and its relation with dopaminergic innervation. Brain Res 730: 17–31
Carli M, Evenden JL, Robbins TW . (1985): Depletion of unilateral striatal dopamine impairs initiation of contralateral actions and not sensory attention. Nature 313: 679–682
Carli M, Jones GH, Robbins TW . (1989): Effects of unilateral dorsal and ventral striatal dopamine depletion on visual neglect in the rat: a neural and behavioural analysis. Neuroscience 29: 309–327
Castañeda E, Whishaw IQ, Robinson TE . (1990): Changes in striatal dopamine neurotransmission assessed with microdialysis following recovery from a bilateral 6-OHDA lesion: variation as a function of lesion size. J Neurosci 10: 1847–1854
Cerruti C, Drian MJ, Kamenka JM, Privat A . (1991): Localization of dopamine carriers by BTCP, a dopamine uptake inhibitor, on nigral cells cultured in vitro Brain Res 555: 51–57
Choi-Lundberg DL, Lin Q, Chang YN, Chiang YL, Hay CM, Mohajeri H, Davidson BL, Bohn MC . (1997): Dopaminergic neurons protected from degeneration by GDNF gene therapy. Science 275: 838–841
Choi-Lundberg DL, Lin Q, Schallert T, Crippens D, Davidson BL, Chang YN, Chiang YL, Qian J, Bardwaj L, Bohn MC . (1998): Behavioral and cellular protection of rat dopaminergic neurons by an adenoviral vector encoding glial cell line-derived neurotrophic factor. Exp Neurol 154: 261–275
Coffin VL, Latranyi MB, Chipkin RE . (1989): Acute extrapyramidal syndrome in Cebus monkeys: development mediated by dopamine DA but not D1 receptors. J Pharmacol Exp Ther 249: 769–774
Connor B, Kozlowski DA, Schallert T, Tillerson JL, Davidson BL, Bohn MC . (1999): Differential effects of glial cell line-derived neurotrophic factor (GDNF) in the striatum and substantia nigra of the aged Parkinsonian rat. Gene Ther 6: 1936–1951
Costall B, Naylor RW, Olley J . (1973): Stereotypy and anti-cateleptic action of amphetamine after intracerebral injection. Eur J Pharmacol 18: 83–94
Creese I, Snyder SH . (1979): Nigrostriatal lesions enhance striatal [3H]apomorphine and [3H]spiroperidol binding Eur. J Pharmacol 56: 277–281
Döbrössy MD, Dunnett SB . (1997): Unilateral lesions impair response execution on lateralized choice reaction time task. Behav Brain Res 87: 159–171
Evarts EV, Teravainen H, Calne DB . (1981): Reaction time in Parkinson's disease. Brain 4: 167–186
Garris PA, Ciolkowski EL, Pastore P, Wightman RM . (1994): Efflux of dopamine from the synaptic cleft in the nucleus accumbens of the rat brain. J Neurosci 14: 6084–6093
Gauntlett-Gilbert J, Brown VJ . (1998): Reaction time deficits and Parkinson's disease. Neurosci Biobehav Rev 22: 865–881
Gerlach M, Riederer P . (1996): Animal models of Parkinson's disease: an empirical comparison with the phenomenology of the disease in man. J Neural Transm Gen Sect 103: 987–1041
Hauber W, Bubser M, Schmidt WJ . (1994): 6-Hydroxydopamine lesion of the rat prefrontal cortex impairs motor initiation but not motor execution. Exp Brain Res 99: 524–528
Hefti F, Melamed E, Wurtman RJ . (1980): Partial lesions of the dopaminergic nigrostriatal system in rat bran: biochemical characterization. Brain Res 195: 123–137
Hersch SM, Yi H, Heilman CJ, Edwards RH, Levey AI . (1997): Subcellular localization and molecular topology of the dopamine transporter in the striatum and substantia nigra. J Comp Neurol 388: 211–227
Hornykiewicz O, Kish S . (1987): Biochemical pathophysiology of Parkinson's disease. Adv Neurol 45: 19–34
Jenner P, Marsden CD . (1986): The actions of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine in animals as a model of Parkinson's disease. J Neural Transm (Suppl 20):11–39
Jeon BS, Lewis VJ, Burke RE . (1995): 6-Hydroxydopamine lesion of the rat substantia nigra: time course and morphology of cell death. Neurodegeneration 4: 131–137
Kozlowski DA, Connor B, Tillerson JL, Schallert T, Bohn MC . (2000): Delivery of a GDNF gene into the substantia nigra after a progressive 6-OHDA lesion maintains functional nigrostriatal connections. Exp Neurol 166: 1–15
Marshall JF . (1979): Somatosensory inattention after dopamine depleting intracerebral 6-OHDA injections: spontaneous recovery and pharmacological control. Brain Res 177: 311–324
Marshall JF . (1984): Brain function: neural adaptations and recovery from injury. Annu Rev Psychol 35: 277–308
Moukhles H, Amalric M, Nieoullon A, Daszuta A . (1994): Behavioral recovery of rats grafted with dopamine cells after partial striatal dopaminergic depletion in a conditioned reaction-time task. Neuroscience 63: 73–84
Neve KA, Kozlowski MR, Marshall JF . (1982): Plasticity of neostriatal dopamine receptors after nigrostriatal injury: relationship to recovery of sensorimotor functions and behavioral supersensitivity. Brain Res 244: 33–44
Neve KA, Altar CA, Wong CA, Marshall JF . (1984): Quantitative analysis of [3H]spiroperidol binding to rat forebrain sections: plasticity of neostriatal dopamine receptors after nigrostriatal injury. Brain Res 302: 9–18
Nirenberg MJ, Vaughan RA, Uhl GR, Kuhar MJ, Pickel VM . (1996): The dopamine transporter is localized to dendritic and axonal plasma membranes of nigrostriatal dopaminergic neurons. J Neurosci 16: 436–447
Parsons LH, Smith AD, Justice JB Jr . (1991): The in vivo microdialysis recovery of dopamine is altered independently of basal level by 6-hydroxydopamine lesions to the nucleus accumbens. J Neurosci Methods 40: 2–3 139–147
Paxinos G, Watson C . (1986): The rat brain in stereotaxic coordinates. San Diego, Academic Press
Phillips J, Brown VJ . (1999): Reaction time performance following unilateral striatal dopamine depletion and lesions of the subthalamic nucleus in the rat. Eur J Neurosci 11: 1003–1010
Price MT, Fibiger HC . (1974): Apomorphine and amphetamine stereotypy after 6-hydroxydopamine lesions of the substantia nigra. Eur J Pharmacol 29: 249–252
Przedborski S, Jackson-Lewis V . (1998): Mechanisms of MPTP neurotoxicity. Mov Disord 13: 35–38
Robinson TE, Whishaw IQ . (1988): Normalization of extracellular dopamine in striatum following recovery from a partial unilateral 6-OHDA lesion of the substantia nigra: a microdialysis study in freely moving rat. Brain Res 450: 209–224
Robinson TE, Mocsary Z, Camp DM, Whishaw IQ . (1994): Time course of recovery of extracellular dopamine following partial damage to the nigrostriatal dopamine system. J Neurosci 14: 2687–2696
Rosenblad C, Martinez-Serrano A, Bjorklund A . (1998): Intrastriatal glial cell line-derived neurotrophic factor promotes sprouting of spared nigrostriatal dopaminergic afferents and induces recovery of function in a rat model of Parkinson's disease. Neuroscience 82: 129–137
Salamone JD, Zigmond MJ, Stricker EM . (1990): Characterization of the impaired feeding behavior in rats given haloperidol or dopamine depleting brain lesions. Neuroscience 39: 17–24
Schneider JS, Rothblat DS, DiStefano L . (1994): Volume transmission of dopamine over large distances may contribute to recovery from experimental parkinsonism. Brain Res 643: 86–91
Smith AD, Smith DL, Zigmond MJ, Amalric M, Koob GF . (2000): Differential effects of dopamine receptor subtype blockade on performance of rats in a reaction time paradigm. Psychopharmacology (Berl) 148: 355–360
Statton LM, Solomon PR . (1984): Microanalysis of D-amphetamine into the nucleus accumbens and caudate putamen. Physiol Psychol 12: 159–162
Stricker EM, Zigmond MJ . (1976) Recovery of function after damage to central catecholamine-containing neurons: a neurochemical model for the lateral hypothalamic syndrome. In Sprague JM, Epstein A (eds), Progress in Psychobiology and Physiological Psychology, Vol 6. New York, Academic Press, pp 121–187
Volpe BT, Wessel TC, Mukherjee B, Federoff HJ . (1995): Temporal pattern of internucleosomal DNA fragmentation in the striatum and hippocampus after transient forebrain ischemia. Neurosci Lett 186: 157–160
Yung KKL, Bolam JP, Smith AD, Hersch SM, Ciliax BJ, Levey AI . (1995): Immunocytochemical localization of D1 and D2 dopamine receptors in the basal ganglia of the rat: light and electron microscopy. Neuroscience 65: 709–730
Zhang WQ, Tilson HA, Nanry KP, Hudson PM, Hong JS, Stachowiak MK . (1988): Increased dopamine release from striata of rats after unilateral nigrostriatal bundle damage. Brain Res 461: 2 335–342
Zigmond MJ . (2000): When it comes to communications between neurons, synapses are over-rated: insights from an animal model of Parkinsonism. In Agnati LF, Fuxe, K, Nicholson C, Sykova E (eds), Progress in Brain Research: Volume Transmission Revisited. New York, Elsevier, pp 317–326
Zigmond MJ, Keefe KA . (1997): 6-Hydroxydopamine as a tool for studying catecholamines in adult animals. Lessons from the neostriatum. In Kostrzewa RM (ed), Highly Selective Neurotoxins: Basic and Clinical Applications. New Jersey: Humana Press Inc., pp 75–107
Zigmond MJ, Abercrombie ED, Berger TW, Grace AA, Stricker EM . (1990): Compensations after lesions of central dopaminergic neurons: some clinical and basic implications. Trends Neurosci 113: 290–296
Zigmond MJ, Acheson AL, Stachowiak MK, Stricker EM . (1984): Neurochemical compensation after nigrostriatal bundle injury in an animal model of preclinical parkinsonism. Arch Neurol 41: 856–861
Zigmond MJ, Stricker EM . (1980): Supersensitivity after intraventricular 6-hydroxydopamine: relation to dopamine depletion. Experentia 36: 436–437
Zigmond MJ, Stricker EM . (1973): Recovery of feeding and drinking by rats after intraventricular 6-hydroxydopamine or lateral hypothalamic lesions. Science 182: 717–720
Acknowledgements
This research was supported by NIH grant DA 04398 (GFK) and NS19608 (MJZ). This is publication number 13807-NP from the Scripps Research Institute. The authors would like to thank Michael Arends for editing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smith, A., Amalric, M., Koob, G. et al. Effect of Bilateral 6-Hydroxydopamine Lesions of the Medial Forebrain Bundle on Reaction Time. Neuropsychopharmacol 26, 756–764 (2002). https://doi.org/10.1016/S0893-133X(01)00420-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/S0893-133X(01)00420-1
Keywords
This article is cited by
-
Tyrosine Hydroxylase Inhibition in Substantia Nigra Decreases Movement Frequency
Molecular Neurobiology (2019)
-
Evidence for cross-hemispheric preconditioning in experimental Parkinson’s disease
Brain Structure and Function (2018)
