
Abstract
Study design:
One cross-sectional study.
Objectives:
To examine the extent to which a sample of adults with spinal cord injury (SCI) meet the SCI-specific physical activity guidelines and to identify potential demographic, injury and motivational characteristics related to participation.
Setting:
Quebec, Canada.
Methods:
A sample of 73 adults from the province of Quebec, Canada living with SCI completed the Leisure Time Physical Activity Questionnaire for People with Spinal Cord Injury to report their current frequency (sessions per week) and duration (minutes per session) in aerobic and resistance physical activity.
Results:
Results showed that 12% of participants in this sample met the guidelines and as many as 44% reported 0 min of physical activity. Only the participants’ mode of mobility and autonomous motivation for physical activity emerged as a marginal correlate of the likelihood of meeting the physical activity guidelines.
Conclusion:
Overall, physical activity participation rates among adults in this sample living with SCI remain quite low. Given the benefits of physical activity for adults with SCI, physical activity promotion efforts are needed.
Similar content being viewed by others

Introduction
A number of studies have examined the physiological and psychological benefits of physical activity for adults with spinal cord injury (SCI). In a systematic review of the literature focusing on the physiological benefits, Hicks et al.1 found physical activity to be effective for improving physical capacity and muscular strength in the SCI population. Extensive research has also explored the psychological benefits of physical activity among adults with SCI. Across three systematic reviews, positive relationships between physical activity and motivation, quality of life and well-being have been consistently found.2, 3, 4
Given the many benefits of physical activity for adults with SCI, a panel of experts was convened in 2011 to develop the first evidence-based physical activity guidelines for this population.5 These guidelines focused on both aerobic and resistance physical activities, with the objective of improving physical fitness among adults with SCI. The guidelines recommend that adults with SCI participate in at least 20 min of moderate-intensity (activities that feel somewhat difficult, but can be sustained) to vigorous-intensity (activities that feel very difficult, and cannot be sustained for long) aerobic physical activity two times per week. These aerobic activities may consist of upper body, lower body or whole-body exercises. For resistance activity, the guidelines recommended two sessions per week, where each training session should consist of three sets of 8–10 repetitions of each exercise, for each major muscle group. Support for these guidelines has been reported in a recent randomized controlled trial6 where participants of a 16-week program that targeted the SCI physical activity guidelines had greater aerobic capacity and endurance, as well as change in muscle strength, compared with participants of a community exercise program who received no direction pertaining to the guidelines.
Current physical activity participation rates
Despite the evidence supporting the benefits of physical activity for adults with SCI, physical activity levels for this population remain lower than the general population.7 For instance, close to 37% of Canadian adults report only 0–15 min of moderate-to-vigorous physical activity per week,8 whereas as many as 50% of adults with SCI report participating in 0 min of physical activity of any kind.9 A separate study examining 277 adults with SCI found similar results where 49% of individuals reported not participating in physical activity of any form.10 These data provide a cursory description of physical activity participation rates among people with SCI, providing insight into the proportion of the population that is completely inactive. However, these studies focus on reports of overall physical activity and do not distinguish between aerobic and resistance physical activities. Given the guidelines recommend both types of physical activity, and that each are associated with different physiological benefits,1 it is important to assess these types of physical activities separately.
We are unaware of any research that has examined the rates of adherence to the physical activity guidelines for people with SCI or examined the demographic, SCI characteristics and psychological correlates of meeting these guidelines. One study11 has attempted to assess rates of physical activity participation in a sample of Swiss adults with SCI relative to the World Health Organization’s (WHO)12 physical activity guidelines (2.5 h of moderate-to-vigorous aerobic physical activity per week) for the general population. This study found that 49% of Swiss adults with SCI met the WHO physical activity guidelines and 50% of their sample reported doing some resistance exercise. Furthermore, the study found that age, gender and severity of injury predicted these participation rates. These physical activity rates are surprisingly high in comparison with the aforementioned studies and the authors acknowledge that these rates were also elevated in relation to physical activity rates of the general Swiss and European populations. Although the instrument used to assess physical activity was designed for individuals with physical disabilities, it did not ask for specific reports of the frequency per week (response options: never, 1–2 days, 3–4 days or 5–7 days) or duration per day (response options: <1 h, <2 h, 2–4 h or >4 h), which may have inflated the physical activity participation rates. In addition, the authors did not report overall physical activity rates (i.e., combined aerobic and resistance) because they were unable to differentiate between individuals who participated in one or two days of resistance physical activity.11 Given these methodological limitations, the findings from this study should be interpreted with caution.
Establishing levels of compliance with the guidelines can provide a benchmark for comparison in future studies and interventions. Therefore, the general purpose of the present study was to examine a sample of adults with SCI and determine the percentage of the sample that are achieving both the aerobic and resistance physical activity guidelines, and determine whether any demographic, SCI characteristics or motivational factors predicted their likelihood of meeting the guidelines.
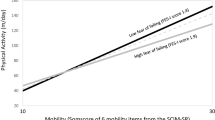
To provide a perspective on the profile of adults with SCI who meet and do not meet the SCI guidelines in this sample, this study will explore the relationship between demographic and SCI-related variables and the likelihood of meeting the SCI-specific physical activity guidelines. In their study, Rauch et al.11 found that women, older adults and individuals with complete tetraplegia were less likely to meet the WHO physical activity guidelines, compared with men, younger adults and individuals with incomplete paraplegia. Similarly, younger age, fewer years since injury, men, manual wheelchair users and individuals with lower injury severity engaged in more physical activity compared with women, power wheelchair users and individuals with higher injury severity, older age and more years since injury.9 In another study exploring the physical activity patterns of people with SCI over an 18-month period, the authors13 found that 22% of the sample was completely inactive and older age, increased time since injury, and severity of injury increased the odds of individuals being classified as inactive, compared with being active. From a motivational perspective, studies have demonstrated that intentions and types of self-efficacy predicted physical activity participation.13, 14 To date, however, no SCI studies have looked at the specific motivational variables that predict meeting the guidelines, nor dissected the specific types of motivation. One framework that looks at different types of motivation is self-determination theory.15 According to this theory, when individuals engage in physical activity for autonomous reasons, where they participated in activity because they value and/or enjoy it, it promotes positive outcomes such as persistence. Alternatively, when individuals engage in behaviours for controlled reasons and participate because of external or internal pressures, they are more likely to experience negative outcomes like burnout. Although this theory has yet to be applied in an SCI physical activity context, one study16 explored the motivational correlates of physical activity in adults with physical disabilities. The authors found that when individuals reported having an autonomous motivation for engaging in physical activity, they reported greater physical activity compared with what would be expected of those who have a controlled motivation towards physical activity.
The specific purpose of this study was to examine the percentage of adults with SCI who meet the SCI-specific physical activity overall guidelines, as well as for the aerobic and resistance guidelines separately, using a sample of adults from Quebec, Canada. A secondary purpose was to examine if any demographic (i.e., age and gender), SCI characteristics (i.e., level of injury, mobility and years since injury) and motivational correlates (i.e., autonomous and controlled motivation) could predict the sample participants’ odds of meeting the physical activity guidelines.
Materials and methods
Participants and procedures
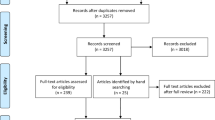
Participants (N=73) were recruited from the Quebec City region of the province of Quebec, Canada through the archives of the primary rehabilitation hospital of the region, as part of a larger research project entitled ‘Towards Interventions Focusing on Community Living and Quality of Life (COM-QOL) for Individuals with Spinal Cord Injury’. To be eligible, participants had to be at least 18 years of age, have an SCI and not report any cognitive impairment. For the study, participants were asked to provide information about their current physical activity by completing a standardized measure of physical activity through a phone interview.
Measures
Participants completed the following measures during a phone interview.
Demographic profile
Participants reported their age, gender, marital status, education, ASIA (American Spinal Injury Association) classification, years since injury and level of injury.
Physical activity behaviour
Participants completed the Leisure Time Physical Activity Questionnaire for People with Spinal Cord Injury (LTPAQ-SCI).17 This questionnaire assessed participants’ self-reported frequency and duration of mild-, moderate- and vigorous-intensity leisure time physical activity during the past 7 days. After hearing a description of each of the three activity intensities, as well as some examples of aerobic and resistance activities that meet each category that were developed alongside the physical activity questionnaire for people with SCI,9 participants indicated the number of times they participated in the specific type of activity in the past 7 days and reported, in minutes, the typical duration of each session. The original validation study supported both the reliability and validity of the scale for measuring physical activity behaviour among adults with SCI.17 For the present study, participants completed the questionnaire twice: once reporting their aerobic activity and a second time reporting their resistance activity. Participants were considered to have met the aerobic physical activity guidelines if they reported at least two sessions of moderate- or vigorous-intensity aerobic activity in the past 7 days and reported that each session had a duration of 20 min or more. The same frequency and duration criteria were applied to resistance physical activity because the questionnaire did not ask about the specific number of sets, repetitions and muscle groups. Using these criteria, the participants were coded into one of the following classifications on the aerobic and resistance physical activity guidelines: (1) Guidelines Met, (2) Some Activity Reported and (3) No Activity Reported. Then, both ratings were combined to create an overall physical activity guideline measure and the following classifications were used: (1) Guidelines Met, (2) Some Activity Reported and (3) No Activity Reported. Participants who reported meeting only one of either the aerobic or resistance physical activity guidelines were classified as ‘Some Activity Reported’.
Motivation for physical activity
Participants also completed the Treatment self-regulation for exercise questionnaire.18 Participants responded to each of the 15 items using a seven-point scale, ranging from 1 (Not at all true) to 7 (Very true) to rate the reason they would meet the physical activity guidelines. A mean score was calculated for autonomous motivation and controlled motivation. The Cronbach’s α were calculated for each subscale and revealed they were above the acceptable limit (α >0.75).
Analyses
As a first step, the data were cleaned to identify any errors or duplicate information, as well as identify any out-of-range or outlier data using standardized scores. Next, descriptive statistics were calculated to report the demographic characteristics of the sample. For the primary purpose of this study, descriptive statistics were calculated on the SCI physical activity data to describe the overall physical activity characteristics of the sample. Then, using this information, participants were classified into one of the three categories based on their reported levels of physical activity. For the secondary purpose, a series of multinomial and binary regressions were conducted to determine whether age, gender, level of injury, mode of mobility, years since injury, autonomous motivation and controlled motivation were related to meeting the physical activity guidelines. Specifically, multinomial logistic regressions were conducted to determine whether demographic, SCI characteristics or motivational factors were related to meeting the aerobic physical activity guidelines, as well as the overall guidelines. Binary logistic regressions were conducted for resistance physical activity guidelines comparing ‘Guidelines Met’ versus ‘No Activity Reported’ groups because too few individuals were categorized in the ‘Some Activity Reported’ group. All logistic regressions were adequately powered as seven or less variables were entered as predictors, meeting the rule of thumb of 10 participants per predictor (n=73).19
Results
Preliminary analyses
The demographic, SCI characteristics and motivational characteristics of this sample are available in Table 1. Descriptive statistics were calculated and participants’ reports of their physical activity behaviour were screened for impossible values and outliers. There were no issues found on participants’ reports of their frequency of physical activity; however, some extremely high scores on participants’ reports of their average session duration were identified (standardized scores (z)=±2.57). These values were recoded to the next closest, but in range, value. The descriptive statistics for these variables after the recoding are presented in Table 2.
Physical activity guidelines
The overall frequencies for each type of physical activity are presented in Figure 1. These results suggest that more adults with SCI in this sample are meeting the aerobic activity (36%), compared with resistance activity guidelines (19%); however, only a small percentage (12%) of the sample met both the aerobic and resistance physical activity guidelines. Looking at the overall guidelines, nearly half (44%) of this sample reported no physical activity whatsoever.

Physical activity rates by specific and overall physical activity guidelines. PAG, physical activity guidelines.
Relationship between demographic/SCI characteristics/motivational factors and SCI-specific physical activity guidelines
No demographic or SCI characteristics predicted meeting the aerobic physical activity guidelines when compared with the no activity or some activity grouping (see Table 3). Looking at the motivational factors, autonomous motivation emerged as a correlate of meeting the aerobic physical activity guidelines compared with the no activity group, odds ratio (OR)=0.21, 95% confidence intervals (CI)=0.09, 0.45. Individuals with higher autonomous motivation for physical activity are more likely (OR=4.76) to be meeting the aerobic guidelines than to be reporting no activity (for ease of interpretation, the inverse of the OR was calculated to make the no activity the reference group). For the resistance physical activity guidelines analyses, no variables emerged as significant correlates. Concerning the overall physical activity guidelines, autonomous motivation was a significant correlate where individuals with an autonomous motivation for physical activity were more likely to meet the guidelines than not (OR=0.20, CIs=0.06, 0.63; inverse OR=5.00) and mobility (manual vs other) had a moderately sized OR of 5.40 with wide CIs ranging from 1.00 to 29.05. Manual wheelchair users were more likely to meet both the aerobic and resistance PA guidelines compared with individuals who reported doing some activity. Mobility may have a role in the extent to which adults meet the SCI-specific physical activity guidelines, but no strong conclusions can be made given the width of the confidence intervals.
Discussion
The purpose of this study was to examine the physical activity rates of a sample of adults with SCI in relation to the SCI-specific physical activity guidelines. This study is the first to conduct such an analysis and found that, in this sample, adults with SCI do not participate in sufficient amounts of physical activity to meet the guidelines to derive fitness and health benefits. Considering the combined aerobic and resistance SCI-specific physical activity guidelines, the percentages of adults with SCI in this sample who reported meeting the SCI-specific physical activity guidelines were 12%. There are no other studies that report on the percent of adults with SCI meeting both the SCI-specific aerobic and resistance physical activity guidelines. We were also unable to examine how our physical activity participation rates compared with the rates of able-bodied Canadian adults who meet the new Canadian physical activity guidelines because the guidelines do not differentiate between resistance and aerobic physical activity.8 The sample did, however, resemble the rates of the American (5%) adult general populations.20 There is evidently more research needed within the SCI population to be able to have better overall SCI-specific physical activity guideline compliance estimates.
Looking at resistance physical activity participation, very few individuals reported participating in resistance activities. Only 19% of our sample met the SCI-specific resistance physical activity guidelines and ~74% of the sample reported no minutes of resistance physical activity. These are lower resistance physical activity rates compared with the findings of Rauch et al.11 (50.3%) with a sample of Swiss adults with SCI. However, Rauch et al.11 were unable to differentiate between individuals who participated in one versus two bouts of resistance physical activity due to the measure used, limiting the comparisons that can be made with the current study findings. In a different sample, Martin Ginis et al.9 found that 33% of adults with SCI participated in some resistance physical activity, leaving ~67% reporting no resistance physical activity. Although this percentage is lower than the 74% found in our study, the Martin Ginis study included time spent in mild intensity resistance physical activity, which also limits the comparison. Again, we were unable to compare the rates with able-bodied Canadian adults because the guidelines do not differentiate between resistance and aerobic physical activity.8 The closest physical activity guidelines approximation in the Canadian population is 15%; however, it was calculated with accelerometers that capture all movement, and thus not accurately measuring resistance physical activity.8 Within the United States, however, we can see that resistance physical activity rates of adults with SCI are ~10% lower than the American able-bodied population whereby 32% of adults participated in at least two bouts of resistance physical activity twice per week.20
The results for the SCI-specific aerobic physical activity guidelines are more encouraging as 36% of adults with SCI in this sample met the guidelines. These rates are lower than the results reported for Swiss adults with SCI relative to the WHO’s12 aerobic physical activity guidelines (48%), as well as lower than the 58% of American able-bodied adults who meet the aerobic criteria for the 2008 Physical Activity Guidelines for Americans.20 Again, there is no specific comparison for able-bodied Canadians because existing data do not differentiate aerobic from resistance physical activity.8 Focusing on the proportion of inactive adults in our study, our results are in line with previous physical activity research, including studies among adults with SCI. We found that 44% of our sample of adults with SCI participated in 0 min of physical activity. These rates of physical inactivity are almost similar to the 50% and 48.5% previously reported by Martin Ginis et al.9 and Anneken et al.,10 respectively, but higher than the 18.6% reported in Rauch et al.11
Mobility emerged as a marginal correlate of the likelihood that individuals met the physical activity guidelines, whereas no other demographic or SCI-related variables were correlates for any other comparisons. These results were somewhat in line with past SCI physical activity studies looking at demographic and SCI variables. For example, among 695 adults with SCI, Martin Ginis et al.9 found that mode of mobility, along with gender, age, years since injury and severity of injury were significant correlates of weekly minutes of reported physical activity. In another study, Martin Ginis et al.21 found a small effect for the number of years post injury as a correlate of physical activity. These studies, however, did not distinguish between reported aerobic and resistance physical activity and the outcome of interest (total minutes per day of Leisure Time Physical Activity) and included mild intensity activity. Rauch et al.11 also found that younger adults, men, adults with incomplete paraplegia and manual wheelchair users were more likely to meet the aerobic recommendations compared with older adults, women, adults with complete paraplegia and individuals without device/support, respectively. Regarding resistance physical activity, the only difference was adults with complete paraplegia were less likely to participate in at least one resistance physical activity per week than adults with incomplete paraplegia. Taken together, it appears that mode of mobility is a consistent correlate of physical activity participation. One such explanation as evidenced by a previous study is that manual wheelchair users report more positive attitudes about physical activity participation compared with power chair users, which can promote increased physical activity participation.22 Although the results of these previous studies explored the correlates of physical activity for adults with SCI, they did not investigate these among adults who meet the overall physical activity guidelines (i.e., both aerobic and resistance guidelines). Despite finding significant relationships between the aforementioned correlates and physical activity, a closer look at the results of these studies with large samples show relatively small effect sizes (βs<0.18), suggesting weak relationships. These consistently weak relationships between correlates and physical activity across studies could explain why we found few significant relationships in comparison with other studies given our sample size.
In terms of motivational factors, autonomous motivation emerged as a correlate of the likelihood that individuals met both the aerobic physical activity guidelines and the overall physical activity guidelines, compared with adults who reported no activity in our sample. These results were in line with a systematic review that supported autonomous motivation as a significant predictor of physical activity16 and one prospective study with adults with a disability.16 More recently, a longitudinal study23 examining autonomous motivation and physical activity for people with physical disabilities (including adults with SCI) did not find the same results. Specifically, they found improvements in autonomous motivation for physical activity over 1 year, but these improvements did not predict increases in reported physical activity. These two studies, however, did not use the same measure of physical activity and neither distinguished between aerobic and resistance physical activity, which may account for the discrepancies between all three studies when it comes to examining motivational correlates. Given the limited research using autonomous motivation as a predictor of physical activity among adults with disabilities, additional studies are needed to truly determine the role of autonomous motivation for physical activity among this population. It appears, however, that autonomous motivation may be an important variable for adults with SCI, as per the results from our sample.
Practical implications
Our results provide a preliminary look at the rates for a sample of adults with SCI who meet the SCI-specific physical activity guidelines. Therefore, our study and that of Rauch et al.11 provide a starting point for future studies and interventions to compare physical activity rates of adults with SCI, using two different sets of guidelines. Given the physical activity rates among adults with SCI remain quite low, physical activity promotion efforts are needed to target both non-active (reporting 0 min of physical activity) and somewhat active (reporting some physical activity, but not meeting guidelines) adults with SCI. It may also be particularly important to promote resistance physical activity specifically among adults with SCI given that over 70% of our sample reported 0 min of resistance activity. Latimer-Cheung et al.24 found that a peer-mediated home-based resistance physical activity intervention resulted in large increases in weekly bouts, duration and overall volume (time/distance) among adults with SCI. Results from these studies prompt a call for more physical activity promotion efforts and echo the conclusions made by Nery et al.25 who also highlighted the need for more physical activity interventions among adults with SCI.
Limitations and future research
Although our study provides an initial look at the compliance of the physical activity guideline in a sample of adults with SCI, there are some limitations. First, the rates are based on self-reported physical activity, which can provide some reporting bias and the sample size of this study was also relatively small. To have sufficient statistical power to move beyond this sample and estimate the physical activity participation rates of adults with SCI at the population level, a much larger sample would be required.9 Therefore, a larger study using an objective measure of physical activity may provide more accurate picture of the percentage of Canadian adults who meet the SCI-specific physical activity guidelines. Next, in measuring resistance physical activity, we only asked participants to indicate the frequency and average minutes of training, but not the number of sets or muscle groups trained. Future studies could attempt to develop a measure to better capture resistance physical activity among adults with SCI. Given the low rates of resistance physical activity, it may also be important for future studies to explore the reasons behind why so few individuals with SCI participate in resistance physical activity and determine whether it is because of a lack of knowledge, skill, motivation or a combination of such reasons. We also only examined if the demographics, SCI characteristics and motivational factors predicted the likelihood of meeting the physical activity guidelines; however, other variables may have a more important role. For example, Martin Ginis et al.9 found that self-regulation had a direct impact on reported physical activity for adults with SCI after controlling for demographic and SCI characteristics. Therefore, psychosocial correlates may have a larger role in predicting the likelihood of meeting the SCI-specific physical activity guidelines compared with demographic and SCI characteristics. Furthermore, we did not ask participants to report on their socioeconomic status or their access to adapted facilities for engaging in physical activity. These factors have been identified as barriers to participation in previous research on adults with SCI14, 26 and future research should also explore how the availability of these facilities, as well as participants’ ability to pay for services influences physical activity participation rates for adults with SCI. Finally, we did not examine participants’ physical activity levels before their injury as a potential correlate of meeting the guidelines. There is conflicting evidence on the role this plays in predicting physical activity. Some research27 has supported that people who are active before their injury are more likely to remain active after their injury, whereas other research9 did not find the same relationship. It would be important to examine how this predicts adults’ likelihood of meeting the SCI-specific physical activity guidelines.
Conclusions
The majority of adults with SCI in this sample do not meet either the aerobic or the resistance physical activity guidelines for this population and only ~12% meet the SCI-specific physical activity guidelines for both types of physical activity. Our study is the first to investigate physical activity guideline compliance rates among adults from Quebec, Canada living with SCI and to use the SCI-specific guidelines as the comparison for such an analysis. Given the lack of research establishing physical activity guidelines compliance rates among adults with SCI, we encourage researchers to use our findings as a basis for future studies to assess participation rates. Such studies will help provide a global picture of the physical activity rates of adults with SCI.
Data archiving
There were no data to deposit.
References
Hicks A, Martin Ginis K, Pelletier C, Ditor D, Foulon B, Wolfe D . The effects of exercise training on physical capacity, strength, body composition and functional performance among adults with spinal cord injury: a systematic review. Spinal Cord 2011; 49: 1103–1127.
Teixeira P, Carraca E, Markland D, Silva M, Ryan R . Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act 2012; 9: 1–30.
Martin Ginis K, Jetha A, Mack D, Hetz S . Physical activity and subjective well-being among people with spinal cord injury: a meta-analysis. Spinal Cord 2010; 48: 65–72.
Tomasone J, Wesch N, Martin Ginis K, Noreau L . Spinal cord injury, physical activity, and quality of life: a systematic review. Kinesiol Rev 2013; 2: 113–129.
Martin Ginis K, Hicks A, Latimer A, Warburton D, Bourne C, Ditor D et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011; 49: 1088–1096.
Pelletier CA, de Zepetnek JT, MacDonald MJ, Hicks AL . A 16-week randomized controlled trial evaluating the physical activity guidelines for adults with spinal cord injury. Spinal Cord 2015; 53: 363–367.
van den Berg E, Bussmann J, Hisma J, Sluis T, van der Woude L, Bergen M et al. prospective study on physical activity levels after spinal cord injury during inpatient rehabilitation and the year after discharge. Arch Phys Med Rehab 2008; 89: 2094–2101.
Colley R, Garriguet D, Janssen I, Craig C, Clarke J, Tremblay M. . Physical activity of Canadian adults: accelerometer results from the 2007 To 2009 Canadian Health Measures Survey. Health Rep. 2011; 2: 7.
Martin Ginis K, Latimer A, Arbour-Nicitopoulos K, Buchholz A, Bray S, Craven C et al. Leisure Time Physical Activity in a Population-Based Sample of People with Spinal Cord Injury Part 1: demographic and injury-related correlates. Arch Phys Med Rehab 2011; 91: 722–728.
Anneken V, Hanssen-Doose A, Hirschfeld S, Scheuer T, Thietje R . Influence of physical exercise on quality of life in individuals with spinal cord injury. Spinal Cord 2010; 48: 393–399.
Rauch A, Hinrichs T, Oberhauser C, Cieza A . Do people with spinal cord injury meet the WHO recommendations on physical activity? Int J Pub Health 2015; 61: 17–27.
World Health Organization. Global recommendations on physical activity for health, 2010 [internet]. Available at:http://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (last accessed 19 September 2015).
Sweet S, Martin Ginis K, Latimer-Cheung A . Examining Physical Activity Trajectories for People with Spinal Cord Injury. Health Psychol 2012; 31: 728–732.
Martin Ginis K, Ma J, Latimer-Cheung A, Rimmer J . A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol Rev 2016; 10: 478–494.
Deci E, Ryan R . Intrinsic Motivation and Self-determination in Human Behavior. Plenum Press: New York, NY, USA. 1985.
Saebu M, Sorensen M, Halvari H . Motivation for physical activity in young adults with physical disabilities during a rehabilitation stay: a longitudinal test of self-determination theory. J Appl Soc Psychol 2013; 43: 612–625.
Martin Ginis K, Phang S, Latimer A, Arbour-Nicitopoulos K . Reliability and validity tests of the Leisure Time Physical Activity Questionnaire for People with Spinal Cord Injury. Arch Phys Med Rehab 2012; 93: 677–682.
Levesque C, Williams G, Elliot D, Pickering M, Bodenhamer B, Finley P . Validating the Theoretical Structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ Res 2016; 22: 691–702.
Vittinghoff E, McCulloch C . Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol 2007; 165: 710–718.
Loustalot F, Carlson S, Kruger J, Buchner D, Fulton J . Muscle-strengthening activities and participation among adults in the United States. Res Q Exercise Sport 2013; 84: 30–38.
Martin Ginis K, Arbour-Nicitopoulos K, Latimer-Cheung A, Buchholz A, Bray S, Craven B et al. Predictors of Leisure Time Physical Activity Among People with Spinal Cord Injury. Ann Behav Med 2012; 44: 104–118.
Martin Ginis K, Papathomas A, Perrier MJ, Smith B,, SHAPE-SCI Research Group. Psychosocial factors associated with physical activity in ambulatory and manual wheelchair users with spinal cord injury: a mixed-methods study. Disabil Rehabil 2015; 39: 187–192.
Skatteboe S, Roe C, Perrin P, Dalen H, Bautz-Holter E, Nyquist A et alOne-year trajectories of motivation and physical activity in persons with disabilities. J Rehabil Med 2016; 48: 371–377.
Latimer-Cheung AE, Arbour-Nicitopoulos KP, Brawley LR, Gray C, Wilson J, Prapavessis H et al. Developing physical activity interventions for adults with spinal cord injury. Part 2: Motivational counseling and peer-mediated interventions for people intending to be active. Rehabil Psychol 2013; 58: 307.
Nery M, Driver S, Vanderbom K . Systematic framework to classify the status of research on spinal cord injury and physical activity. Arch Phys Med Rehab 2013; 94: 2027–2031.
Tasiemski T, Kennedy P, Gardner B, Blaikley R . Athletic identity and sports participation in people with spinal cord injury. Adapt Phys Act Q 2004; 21: 364–378.
Jaarsma E, Dijkstra P, Dekker G . Barriers to and facilitators of sports participation for people with physical disabilities: a systematic review. Scan J Med Sci Sports 2014; 24: 871–881.
Acknowledgements
We thank Anne-Marie Belley, Frédéric Dumont, Samantha Jeske, Isabelle Cummings and Celina Shirazipour for their help with data collection, as well as Kelly Arbour-Nicitopoulos for her comments on the mansucript. These studies were funded through COM-QOL, a collaboration funded through the Ontario Neurotrauma Foundation (ONF) and the Provincial Rehabilitation Research Network (REPAR) Ontario/Quebec Inter-Provincial Partnership grant program; F Routhier and S Sweet are Research Scholars (Junior 1) through the Fonds de recherche du Québec—Santé (FRSQ); and A Latimer-Cheung is funded through the CIHR Canada Research Chair program. Although this study was supported through a number of funding sources, none of the seven authors have any conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Rocchi, M., Routhier, F., Latimer-Cheung, A. et al. Are adults with spinal cord injury meeting the spinal cord injury-specific physical activity guidelines? A look at a sample from a Canadian province. Spinal Cord 55, 454–459 (2017). https://doi.org/10.1038/sc.2016.181
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.181
This article is cited by
-
Healthcare providers’ promotion of physical activity among child and adolescent cancer survivors: strategies and challenges
Journal of Cancer Survivorship (2023)
-
Critical factors influencing the decision to enroll in a physical activity intervention among a predominant group of adults with spinal cord injury: a grounded theory study
Spinal Cord (2021)
-
Exercise for people with SCI: so important but difficult to achieve
Spinal Cord (2021)
-
Physical activity among individuals with spinal cord injury who ambulate: a systematic scoping review
Spinal Cord (2020)
-
Leisure time physical activity participation in individuals with spinal cord injury in Malaysia: barriers to exercise
Spinal Cord (2018)
