
Abstract
Objective:
Orthoses for various joints sections are considered to greatly influence the gait function and energy expenditure in spinal cord-injured (SCI) patients. The aim of this review was to determine the influence of orthoses characteristics and options on the improvement of walking in patients with SCI.
Methods:
A search was performed using the Population Intervention Comparison Outcome (PICO) method, based on selected keywords; studies were identified electronically in the Science Direct, Google Scholar, Scopus, Web of Knowledge and PubMed databases. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) method was used to report the results. Assessment of the quality of all articles was performed based on the Physiotherapy Evidence Database (PEDro scale).
Results:
Twelve studies evaluated the effects of different hip joint options on walking parameters and energy expenditure. Five studies investigated the role of knee joint options on gait parameters and compensatory trunk motion. Only five studies analyzed modified ankle joints on gait parameters in SCI patients. Nine studies analyzed gait parameters in SCI patients as powered orthoses and exoskeleton. These studies had a low level of evidence according to the PEDro score (2/10).
Conclusion:
The various joint types of orthoses appear to be critical in the improvement of walking in patients with SCI. In particular, 'user friendly' orthoses that support the related structure such as the hip joint with a reciprocating mechanism, activated knee joint and movable ankle joint with dorsiflexion assist enable SCI patients to optimize their walking pattern when wearing an orthoses system.
Similar content being viewed by others
Introduction
Orthotic gait training is usually considered for spinal cord-injured (SCI) patients during their rehabilitation process to enable them to stand and ambulate. Although the effectiveness of walking with orthoses has been shown in previous studies in this field, the high energy cost of walking with orthoses is reported as the main reason of rejection rate in these patients.1, 2, 3, 4 According to the required compensatory upper limb and trunk motion to facilitate the swing motion of the paralyzed lower limb, SCI patients inevitably require larger energy expenditure for orthotic gait.5, 6, 7 Furthermore, it can be pointed out that the various orthotics options according to joints sections considerably influence the gait function and energy expenditure in SCI patients.
In a recent literature review, Arazpour et al.8 evaluated the walking efficiency during orthotic gait of SCI paraplegics and determined that there is limited evidence, if any, in terms of superiority of powered orthoses on mechanical orthoses. In a review of mechanical and hybrid orthoses of walking in paraplegic patients, Nene et al.9 also noted that mechanical orthoses were used only for exercise purposes. These systems in general were worn for a few hours in a week because of the high rate of energy consumption used during walking with these orthoses.9 In comparison, Karimi noted differences between mechanical orthoses and hybrid orthoses in various kinetic parameters and energy consumption and stated that mechanical orthoses were more effective in providing stability and reducing energy consumption during walking in paraplegic patients.10 In another review, Arazpour et al. reported on the walking efficiency of powered orthoses on walking in paraplegic subjects.11 Although the effect of orthosis options in walking in paraplegic subjects is well reported, it is not clear to what extent the orthosis options for various joints sections influence gait function performance. The aim of the present review was to analyze the different orthosis with and without reciprocation mechanism or another type of exertion mechanism (for example, orthoses that modified hip joints, knee joints and ankle joints) and powered exoskeleton on the improvement of walking in the SCI patients.
Methods
Search strategy
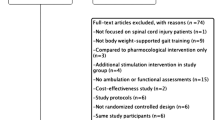
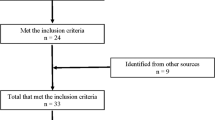
A search was performed using the Population Intervention Comparison Outcome (PICO) method, based on selected keywords and their composition (Table 1). By using ‘OR’, ‘AND’, ‘NOT’ words between the considered keywords, studies were identified electronically in the Science Direct, Google Scholar, Scopus, Web of Knowledge and PubMed databases. Studies were selected by hand searching the reference lists of the electronically identified studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) method was used to report the results. Assessment of the quality of all articles was performed based on the Physiotherapy Evidence Database (PEDro scale). Studies that follow to the outcome measures were included in the final review. According to the chosen inclusion and exclusion criteria, 29 articles were subsequently chosen for final evaluation.
Inclusion and exclusion criteria
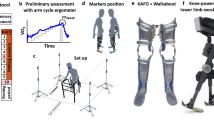
Table 2 demonstrates the inclusion and exclusion criteria in this study. The studies that were considered for inclusion were randomized clinical trials (RCTs), case–control trials, cohort studies, case series studies and single-case studies. Language or year of publication was not considered as restrictions. Studies reporting the effect of all types of mechanical orthoses such as Hip Knee Ankle Foot Orthosis (HKAFOs), Knee Ankle Foot Orthosis (KAFOs), the Louisiana State University Reciprocating Gait Orthosis (LSU RGO), the Advanced Reciprocating Gait Orthosis (ARGO), the Isocentric Reciprocating Gait Orthosis (IRGO), the Parawalker, the Hip Guidance Orthosis (HGO), the Primewalk orthosis, the Walkabout orthosis (WO), the Moorong medial linkage orthosis and powered orthosis (for example, Rewalk, wearable power assist locomotor orthosis (WPAL), the hybrid-assisted limb orthosis (HAL)) designs on paraplegic ambulation were selected for further analysis. Papers were selected from peer reviewed journals, which demonstrated or reported energy consumption, temporal spatial, kinematics and kinetic effects of mechanical orthoses with adding options or alternation in components used in SCI subjects. Studies that included alternative outcome measures, employed ‘body weight support systems with robot-assisted gait', compared primary outcome measures between patients with different disabilities and those that tested orthoses with healthy volunteer subjects (even though the orthoses of interest were utilized in the study) were also excluded. The abstracts and full text of all of the studies found in all databases were compared with the inclusion criteria by two independent reviewers.
Results
The studies identified for those with SCI are either individual case reports or individual subject data from a multiple case series and are therefore classified as poor quality papers (Tables 3, 4, 5, 6). PEDro scores ranged from 1 to 4 across studies, with a median value of 2.
Studies that evaluated modified hip joints on gait parameters in the SCI patients
Table 3 demonstrated studies that evaluated the modified hip joints on gait parameters in the SCI patients. Twelve studies evaluated the effects of different hip joint options on walking parameters and energy expenditure.5, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22 These studies had low level of evidence according to the PEDro score (2/10). Table 3 provides details on the studies evaluating modified hip joints in patients with SCI. As outlined in Table 3, in 4 of 12 studies, functional electrical simulation (FES) with and without RGO was evaluated in comparison with a mechanical orthosis (for example, long leg brace and medial linkage orthosis).5, 12, 17, 19 In 7 of 12 studies, different mechanical orthoses compared with each other, and it has proved that various forms of RGOs have a higher velocity and lower energy expenditure in comparison with conventional and medial linkage orthoses.13, 14, 15, 16, 18, 21, 22 Only one study compared a powered orthosis with two other mechanical orthoses.23
There were three types of mechanical hip joint mechanism (HKAFO, RGO and medial linkage orthosis (MLO)) in orthoses, which were used in walking in SCI patients. A simple hip joint with one degree of freedom generally was used in the HKAFO as the first mechanism of hip joint system. Paraplegic patients use a swing through walking pattern during ambulation with this type of orthosis. RGO, as the second mechanism of hip joint system, were introduced in the late 1960s. The hip joints linked together to provide reciprocal motions of both hip joints that connected two sides KAFOs. Within this type of orthosis, a hip mechanism prevents uncontrolled collapse of the trunk and allows freely upper extremities movement of SCI patients. A modified version of RGOs is referred to as the advanced reciprocating gait orthosis (ARGO) with a one pull–push cable within the pelvic section developed to assist walking performance in paraplegic subjects. A more developed RGO is defined as the isocentric reciprocating gait orthosis (IRGO) and was introduced by Motlock in 1992.24 Another type of mechanical orthosis is MLO as the third mechanism of the hip joint system. There are variations of this type of orthosis, which include the Walkabout,25 Moorong16 and Primewalk,26 the HALO18 and new reciprocating MLO.27
Studies that evaluated modified knee joints on gait parameters in SCI patients
Table 4 demonstrated studies that evaluated the modified knee joints on gait parameters in the SCI patients. Five studies investigated the role of knee joint options on gait parameters and compensatory trunk motion.28, 29, 30, 31, 32 These studies had a low level of evidence according to the PEDro score (2/10). In an identifying paper, it has been shown that adding FES to knee extensor (quadriceps) muscles with the RGO system reduces heart rate and energy expend.
All of the RGOs that are used for ambulation in paraplegic patients hold the knee in a locked and extended position. Combination of these orthoses with external actuators or using mechanical stance control orthosis in this type of orthosis can refine and provide a suitable means of progression of rehabilitation and technology this field. Developments in the mechanical design,29 hybrid orthoses33, 34 active powered knee joints,20, 32 the pneumatic artificial limb in KAFO,35 motorized SCKAFO36 and motorized KAFO37 have been introduced to provide knee flexion during the swing phase of walking by SCI patients.
Studies that evaluated modified ankle joints on gait parameters in SCI patients
Table 5 demonstrated studies that evaluated the modified ankle joints on gait parameters in the SCI patients. Only five studies analyzed modified ankle joints on gait parameters in SCI patients.33, 34, 38, 39, 40 These studies had a low level of evidence according to the PEDro score (2/10). All five studies measured gait parameters and balance with changes in ankle joint from solid to dorsiflexion assist and also adding some changes in shoe such as rocker. In only two studies, energy expenditure was measured.39, 40
Studies investigating the effects of powered orthosis and exoskeleton on gait parameters in SCI subjects
Table 6 shows studies investigating the effects of powered orthosis and exoskeleton on gait parameters by SCI subjects. Nine studies analyzed gait parameters in SCI patients as powered orthoses and exoskeleton.41, 42, 43, 44, 45, 46, 47, 48, 49 These studies had a low level of evidence according to the PEDro score (2/10). Powered lower limb orthoses such as the HAL-5 Type-C (hybrid assistive limb), which has five electric motors45,50 the ReWalk powered orthosis (Argo Medical Technologies),42, 43 the wearable power assist locomotor (WPAL)41 and the e LEGS powered orthosis (Berkeley Bionics) are all examples of commercially developed powered orthoses designed for walking by individuals with paraplegia.
Discussion
Walking with a mechanical orthosis is not ideal for SCI patients because of high loads on upper limb joints and high rate of energy consumption. Some authors have also stated that walking with mechanical orthoses is boring and exhausting.13, 28 Improvement of the mechanical structure of the orthosis and using external power to drive the mechanical orthoses are reported as the two methods that show improvement of gait parameters in paraplegic patients.8 The mechanical orthoses have a simple structure and user friendly design. This type of orthosis, however, has not progressed in development in recent years, as technology of the powered orthoses appears to be the main focus of research in rehabilitation and assisted walking and ambulation in SCI patients.
The influence of the modified hip joint systems on walking in SCI patients
The prescribed option in improvement of walking parameters between mechanical orthoses is the IRGO system. Evaluation of the hip joint mechanism when using the IRGO has been reported to demonstrate improved gait parameters and energy consumption compared with other RGOs, HKAFO and MLOs.51 The difference between walking with optimal mechanical orthoses (IRGOs) with healthy subjects walking is high.23, 52 Recent efforts to improve orthoses for SCI patients have led to systems of orthoses that combine the mechanical orthoses with functional electrical stimulation of selected lower extremity muscles and powered orthoses.5, 10, 19, 53 There are currently only a limited range of powered orthoses, but there is some evidence of an increase in temporal spatial parameters when walking with powered orthoses.54, 55 The results of the reviewed studies suggest positive effects of external power (for example, Rewalk, HAL and WPAL) or improvement of the mechanical structure of the orthosis on gait parameters in paraplegic patients.56 Generally, walking parameters and energy consumption improved with new generation of orthoses.53, 57 The evidence to date suggests that powered orthoses have the capability to improve specific gait parameters when compared with non-powered mechanical orthoses such as the IRGO,11, 54, 58, 59, 60 a conventional HKAFO60 and the ARGO.30, 61
Walking with the IRGO was considered as the higher levels of walking parameters between the RGOs in the SCI patients. The means of speed of walking were reported 0.17, 0.19, 0.22, 0.25 and 0.34 m per second.14, 15, 20, 62, 63 The mean of energy consumption was reported 120±6 to 140±11 beats per min) 144 beats per min.14, 62 In the modified hip joint category in using MLO, the values of this parameter were reported 0.11, 0.14, 0.33 m per second with WO,16, 26 0.13 with Moorong, 0.6 m per second with HALO16, 18 and 0.39 with new reciprocating MLO.21 In using powered hip joint, the mean of walking speed was announced 0.40 m per second compared with 0.16 m per second in using orthosis without hip actuator.30 It shows that adding FES to mechanical orthosis reduced heart rate and improved walking speed during ambulation,19, 28 but using MLO increased the PCI (as the energy consumption predicator) compared with IRGO (155 beats per min, 164 beats per min).16 In wearing new reciprocating MLO, the PCI was reduced in four SCI patients.22
The influence of the modified knee joint on walking in SCI patients
Walking with orthoses that locked the knee in extension demonstrated less gait efficiency compared with the orthoses with provided knee flexion. In addition, an increase in temporal spatial parameters (speed of walking, cadence, step length) was reported with powered knee joints or unlock able knee joint compared with a mechanical orthosis (for example, IRGO, ARGO) in SCI patients.30, 31, 32 In the modified knee joint category in using mechanical linked knee ankle joints, the value of the speed of walking reported 0.14 m per second.29 Using powered knee joint associated with ARGO, IRGO had significant influence. The rate of walking speed reported 0.53, 0.31 and 0.33 m per second.30, 31, 32 Energy consumption was not evaluated when modified knee joint was used in the SCI patients. On the basis of knee extension position in the mechanical orthoses, reduction in compensatory motion is demonstrated by using powered orthosis55 or IRGO with stance control knee joint in SCI patients.64 The reduction in energy consumption is shown related to the reduction in vertical and horizontal compensatory motions in SCI patients.
Gas-powered knee joint is similar to the knee joint used in ARGO, provides stability in stance during walking and aids in standing from a sitting position with orthoses. The results of walking with a stance control knee joint were demonstrated with IRGO in one SCI patient,64 and it was noted that there was poor control of knee joint. It therefore appears that this type of knee joint is not a good option in SCI patients.
Knee flexion during walking is one determinant that was used to smoothing the center of the mass pathway and reduced energy consumption during walking. This parameter is very important especially in patients with double lower limb weakness (for example, paraplegic patients).53, 65 Knee flexion in walking provided less compensatory motion during ambulation66 and during orthotic gait these parameters are thought to increase. It is noted that knee flexion during orthotic gait produced more ground clearance and fewer compensatory motions compared with a fixed extended knee during walking.29 In comparison, it was reported that the lack of knee flexion during the swing phase of gait could be the main reason of rejection and fatigue in paraplegic patients.67, 68
The influence of modified ankle joint and foot sections on walking in SCI patients
The ankle joint has a critical role in facilitating forward propulsion during walking by moving the center of mass forward during push-off, with the ankle plantar flexor muscles performing a pivotal role during this phase. This action can cause a reduction in energy expenditure.69, 70, 71 In other words, to control walking and the alternation, the motor output of spinal motor neurons reciprocating limb loading,72, 73, 74 the afferent feedback from the ankle joint is important.
When using an AFO with dorsiflexion assist in ARGO and using a hip and ankle linked orthosis (HALO) mechanism, the cadence and the speed of walking (ARGO:0.35 m per second, HALO:0.60 m per second) have been shown to improve compared with the ARGO with solid AFO and Primewalk orthosis, respectively.18 The speed of walking reported significantly faster (0.31 m per second) and energy costs reduced in paraplegic patients when the weight-bearing control orthosis (WBCO) was used compared with a previous study in this field.39 The WBCO has a reciprocal gait pattern and a movable foot portion. In all types of mechanical orthosis, the dorsiflexion assist ankle joint should be considered. This type of joint allows dorsiflexion motion in ankle in providing ‘C’ posture and in addition causes foot clearance in the swing phase of gait.
Adding rocker soles associated with the RGO is another option in improvement of walking parameter in paraplegic patients.34,40 A rocker sole provides forward progression of the tibia when sagittal plane ankle motion is restricted. In essence, it facilitates shank advancement over a stationary foot.75 The increase in walking speed (ARGO: 0.36 m per second Primewalk: 0.27 m per second) and step length, and improved sagittal plane hip joint kinematics were reported when rocker sole mechanism was used associated with the ARGO and Prime walk.34, 40 Therefore, using this type of shoe modification has the potential to improve gait parameters in SCI patients.
Quality assessment of related studies
However, from 31 studies, just eight studies have the PEDro scale of 3 and 4 in this review. From 31 studies, just four studies included between-group comparisons.12, 13, 17, 19 Fourteen studies published did not provide data with adequate internal validity, as demonstrated by low scores on the PEDro scale (2/10).The study's flaws included lack of randomization procedures, lack of control group, no masking of examiners and patients and also there was a lack of similarity among groups. These more recent studies have not substantially improved the quality of the research. Some of the proposed interpretations are often based on small sample studies with very heterogeneous participant pools. There is a continuing need for high-quality experimental studies in this area. Future studies should consider stronger designs that can control for confusing factors, such as a case report and single-subject designs. A high-quality RCT provides the best design to control for potential bias, thus offering the strongest evidence of cause-effect inferences between interventions and outcomes.
Subject's individual perception of the exertion associated with walking using an orthoses can be related to the energy consumption (good or bad), as well as having a significant impact on whether they might select to use this orthosis on a regular basis. Spadone et al.76 analyzed the perceived exertion associated with the energy consumption when using the Parastep orthosis during walking by paraplegic subjects.76 Ferguson et al.,77 Marsolais et al.78 and Hardin et al.79 demonstrated that perceived exertion in using the bracing system with FES was ‘easier’ than without stimulation. This point was not evaluated in only mechanical orthoses or powered gait orthoses.
Conclusion
On the basis of the difficulties and limitations of orthotic walking, SCI patients who wish to ambulate should be issued with the most appropriate orthotic system. According to the usage of various orthotic options proposed for walking in paraplegic patients, joint types of the orthosis appear to be critical in the improvement of walking with the orthoses. 'user friendly' orthoses with the appreciative structure (for example, hip joint with reciprocating mechanism, activated knee joint and movable ankle joint with dorsiflexion assist) allow SCI patients to walk in the most optimal of conditions when wearing the system.
These types of orthosis, even the hybrid one with reciprocating and FES, are not enough to provide a functional, efficient gait for the paraplegic patient. Another important issue is the deficit of sensory feedback and proprioception and the high demand to control the whole system with the vision and trunk/upper member’s movement.
References
Bernardi M, Macaluso A, Sproviero E, Castellano V, Coratella D, Felici F et al. Cost of walking and locomotor impairment. J Electromyogr Kinesiol 1999; 9: 149–157.
Chantraine A, Crielaard J, Onkelinx A, Pirnay F . Energy expenditure of ambulation in paraplegics: effects of long term use of bracing. Spinal Cord 1984; 22: 173–181.
Massucci M, Brunetti G, Piperno R, Betti L, Franceschini M . Walking with the advanced reciprocating gait orthosis (ARGO) in thoracic paraplegic patients: energy expenditure and cardiorespiratory performance. Spinal Cord 1998; 36: 223–227.
Nene A, Patrick J . Energy cost of paraplegic locomotion using the ParaWalker—electrical stimulation" hybrid" orthosis. Arch Phys Med Rehabil 1990; 71: 116–120.
Hirokawa S, Grimm M, Solomonow M, Baratta R, Shoji H, D'ambrosia R . Energy consumption in paraplegic ambulation using the reciprocating gait orthosis and electric stimulation of the thigh muscles. Arch Phys Med Rehabil 1990; 71: 687–694.
Solomonow M, Baratta R, Shoji H, Ichie M, Hwang S, Rightor N et al (eds). FES powered locomotion of paraplegics fitted with the LSU reciprocating gait orthoses (RGO). vol. 10, Proc Annual Int Conf. IEEE Eng Medicine and Biology Soc, pp 1672, 1988.
Thoumie P, Le Claire G, Beillot J, Dassonville J, Chevalier T, Perrouin-Verbe B et al. Restoration of functional gait in paraplegic patients with the RGO-II hybrid orthosis. A multicenter controlled study. II: physiological evaluation. Paraplegia 1995; 33: 654–659.
Arazpour M, Bani MA, Hutchins SW . Reciprocal gait orthoses and powered gait orthoses for walking by spinal cord injury patients. Prosthet Orthot Int 2012; 37: 14–21.
Nene A, Hermens H, Zilvold G . Paraplegic locomotion: a review. Spinal Cord 1996; 34: 507–524.
Karimi MT . Functional walking ability of paraplegic patients: comparison of functional electrical stimulation versus mechanical orthoses. Eur J Orthop Surg Traumatol 2013; 23: 631–638.
Arazpour M, Bani MA, Kashani RV, Ghomshe FT, Mousavi ME, Hutchins SW . Effect of powered gait orthosis on walking in individuals with paraplegia. Prosthet Orthot Int 2012; 37: 261–267.
Petrofsky JS, Smith JB . Physiologic costs of computer-controlled walking in persons with paraplegia using a reciprocating-gait orthosis. Arch Phys Med Rehabil 1991; 72: 890–896.
Bernardi M, Canale I, Castellano V, Di Filippo L, Felici F, Marchetti M . The efficiency of walking of paraplegic patients using a reciprocating gait orthosis. Spinal Cord 1995; 33: 409–415.
Harvey LA, Davis GM, Smith MB, Engel S . Energy expenditure during gait using the walkabout and isocentric reciprocal gait orthoses in persons with paraplegia. Arch Phys Med Rehabil 1998; 79: 945–949.
Harvey LA, Smith MB, Davis GM, Engel S . Functional outcomes attained by T9-12 paraplegic patients with the walkabout and the isocentric reciprocal gait orthoses. Arch Phys Med Rehabil 1997; 78: 706–711.
Middleton J, Fisher W, Davis G, Smith R . A medial linkage orthosis to assist ambulation after spinal cord injury. Prosthet Orthot Int 1998; 22: 258–264.
Merati G, Sarchi P, Ferrarin M, Pedotti A, Veicsteinas A . Paraplegic adaptation to assisted-walking: energy expenditure during wheelchair versus orthosis use. Spinal Cord 2000; 38: 37–44.
Genda E, Oota K, Suzuki Y, Koyama K, Kasahara T . A new walking orthosis for paraplegics: hip and ankle linkage system. Prosthet Orthot Int 2004; 28: 69–74.
Shimada Y, Hatakeyama K, Minato T, Matsunaga T, Sato M, Chida S et al. Hybrid functional electrical stimulation with medial linkage knee-ankle-foot orthoses in complete paraplegics. Tohoku J Exp Med 2006; 209: 117–123.
Arazpour M, Bani MA, Kashani RV, Ghomshe FT, Mousavi ME, Hutchins SW . Effect of powered gait orthosis on walking in individuals with paraplegia. Prosthet Orthot Int 2013; 37: 261–267.
Bani MA, Arazpour M, Farahmand F, Azmand A, Hutchins S, Kashani RV et al. The influence of new reciprocating link medial linkage orthosis on walking and independence in a spinal cord injury patient. Spinal Cord 2015; 53: S10–S12.
Ahmadi Bani M, Arazpour M, Farahmand F, Kashani RV, Mousavi ME, Hutchins SW . Comparison of new medial linkage reciprocating gait orthosis and isocentric reciprocating gait orthosis on energy consumption in paraplegic patients: a case series. Spinal Cord Ser Cases 2015.
Arazpour M, Mehrpour S, Bani M, Hutchins S, Bahramizadeh M, Rahgozar M . Comparison of gait between healthy participants and persons with spinal cord injury when using a powered gait orthosis-a pilot study. Spinal Cord 2014; 52: 44–48.
Motlock WM . Principles of orthotic management for child and adult paraplegia and clinical experience with the isocentric RGO. Proc 7th World Congress of the International Society for Prosthetics and Orthotics. 1992; Chicago, p 28.
Kirtley C, McKay S . Principles and practice of paraplegic locomotion: experience with the walkabout walking system. Aust Orthot Prosthet Mag 1992; 7: 4–8.
Saitoh E, Suzuki T, Sonoda S, Fujitani J, Tomita Y, Chino N . Clinical experience with a new hip-knee-ankle-foot orthotic system using a medial single hip joint for paraplegic standing and walking. Am J Phys Med Rehabil 1996; 75: 198–203.
Bani MA, Arazpour M, Farahmand F, Sefati S, Baniasad M, Hutchins S et al. Design and analysis of a new medial reciprocal linkage using a lower limb paralysis simulator. Spinal Cord 2015; 53: 380–386.
Solomonow M, Baratta R, Shoji H, Ichie M, Hwang S, Rightor N et al (eds). FES powered locomotion of paraplegics fitted with the LSU reciprocating gait orthoses (RGO). Engineering in Medicine and Biology Society, Proceedings of the Annual International Conference of the IEEE: IEEE, 1988; 10: 1672.
Greene PJ, Granat MH . A knee and ankle flexing hybrid orthosis for paraplegic ambulation. Med Eng Phys 2003; 25: 539–545.
Ohta Y, Yano H, Suzuki R, Yoshida M, Kawashima N, Nakazawa K . A two-degree-of-freedom motor-powered gait orthosis for spinal cord injury patients. Proc Inst Mech Eng H 2007; 221: 629–639.
Arazpour M, Bani MA, Chitsazan A, Ghomshe FT, Kashani RV, Hutchins SW . The effect of an isocentric reciprocating gait orthosis incorporating an active knee mechanism on the gait of a spinal cord injury patient: a single case study. Disabil Rehabil Assist Technol 2013; 8: 261–266.
Kim G, Kang S, Kang S, Ryu J, Mun M, Kim K . Unlockable knee joint mechanism for powered gait orthosis. Int J Precis Eng Manuf 2009; 10: 83–89.
Bani MA, Arazpour M, Ghomshe FT, Mousavi ME, Hutchins SW . Gait evaluation of the advanced reciprocating gait orthosis with solid versus dorsi flexion assist ankle foot orthoses in paraplegic patients. Prosthet Orthot Int 2013; 37: 161–167.
Arazpour M, Hutchins SW, Ahmadi Bani M, Curran S, Bahramizadeh M, Saberi H et al. The influence of a rocker sole adaptation on gait parameters in spinal cord injury patients ambulating with the advanced reciprocating gait orthosis-a pilot study. Disabil Rehabil Assist Technol 2013; 10: 89–92.
Sawicki GS, Ferris DP . A pneumatically powered knee-ankle-foot orthosis (KAFO) with myoelectric activation and inhibition. J Neuroeng Rehabil 2009; 6: 23.
Arazpour M, Chitsazan A, Bani MA, Rouhi G, Ghomshe FT, Hutchins SW . The effect of a knee ankle foot orthosis incorporating an active knee mechanism on gait of a person with poliomyelitis. Prosthet Orthot Int 2013; 37: 411–414.
Arazpour M, Ahmadi F, Bani MA, Hutchins SW, Bahramizadeh M, Ghomshe FT et al. Gait evaluation of new powered knee–ankle–foot orthosis in able-bodied persons: a pilot study. Prosthet Orthot Int 2013; 38: 39–45.
Arazpour M, Bani M, Hutchins S, Curran S, Javanshir M . The influence of ankle joint mobility when using an orthosis on stability in patients with spinal cord injury: a pilot study. Spinal Cord 2013; 51: 750–754.
Kawashima N, Sone Y, Nakazawa K, Akai M, Yano H . Energy expenditure during walking with weight-bearing control (WBC) orthosis in thoracic level of paraplegic patients. Spinal Cord 2003; 41: 506–510.
Suzuki T, Sonoda S, Saitoh E, Murata M, Uno A, Shimizu Y et al. Development of a novel type of shoe to improve the efficiency of knee-ankle-foot orthoses with a medial single hip joint (Primewalk orthoses): a novel type of shoe for Primewalk orthosis. Prosthet Orthot Int 2005; 29: 303–311.
Tanabe S, Saitoh E, Hirano S, Katoh M, Takemitsu T, Uno A et al. Design of the wearable power-assist locomotor (WPAL) for paraplegic gait reconstruction. Disabil Rehabil Assist Technol 2013; 8: 84–91.
Zeilig G, Weingarden H, Zwecker M, Dudkiewicz I, Bloch A, Esquenazi A . Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: a pilot study. J Spinal Cord Med 2012; 35: 96–101.
Esquenazi A, Talaty M, Packel A, Saulino M . The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am J Phys Med Rehabil 2012; 91: 911–921.
Akahira H, Yamaguchi Y, Nakazawa K, Ohta Y, Kawashima N . Effect of dynamic knee motion on paralyzed lower limb muscle activity during orthotic gait: a test for the effectiveness of the motor-assisted knee motion device. J Nov Physiother 2012; 1: 1–6.
Tsukahara A, Hasegawa Y, Sankai Y (eds). Gait support for complete spinal cord injury patient by synchronized leg-swing with HAL. Intelligent Robots and Systems (IROS). IEEE/RSJ International Conference on IEEE, 2011.
Neuhaus PD, Noorden JH, Craig TJ, Torres T, Kirschbaum J, Pratt JE (eds). Design and evaluation of Mina: a robotic orthosis for paraplegics. Rehabilitation Robotics (ICORR). IEEE International Conference on IEEE, 2011; June 29–July 1, 2011, Zurich, Switzerland: 1–8.
Farris RJ, Quintero H, Goldfarb M . Preliminary evaluation of a powered lower limb orthosis to aid walking in paraplegic individuals. IEEE Trans Neural Syst Rehabil Eng 2011; 19: 652–659.
Kang SJ, Ryu JC, Moon IH, Kim KH, Mun MS (eds). Walker gait analysis of powered gait orthosis for paraplegic. World Congress on Medical Physics and Biomedical Engineering 2006. Springer, Berlin, Heidelberg. 2007; pp 2889–2891.
Quintero HA, Farris RJ, Goldfarb M . A method for the autonomous control of lower limb exoskeletons for persons with paraplegia. J Med Device 2012; 6: 041003.
Suzuki K, Mito G, Kawamoto H, Hasegawa Y, Sankai Y . Intention-based walking support for paraplegia patients with Robot Suit HAL. Adv Rob 2007; 21: 1441–1469.
Ahmadi Bani M, Arazpour M, Farahmand F, Mousavi ME, Hutchins SW . The efficiency of mechanical orthoses in affecting parameters associated with daily living in spinal cord injury patients: a literature review. Disabil Rehabil Assist Technol 2014; 10: 183–190.
Arazpour M, Joghtaei M, Bahramizadeh M, Bani MA, Hutchins SW, Curran S et al. Comparison of gait between healthy participants and persons with spinal cord injury when using the advanced reciprocating gait orthosis. Prosthet Orthot Int 2015.
Yang L, Condie D, Granat M, Paul J, Rowley D . Effects of joint motion constraints on the gait of normal subjects and their implications on the further development of hybrid FES orthosis for paraplegic persons. J Biomech 1996; 29: 217–226.
Audu ML, To CS, Kobetic R, Triolo RJ . Gait evaluation of a novel hip constraint orthosis with implication for walking in paraplegia. IEEE Trans Neural Syst Rehabil Eng 2010; 18: 610–618.
Arazpour M, Chitsazan A, Hutchins SW, Ghomshe FT, Mousavi ME, Takamjani EE et al. Design and simulation of a new powered gait orthosis for paraplegic patients. Prosthet Orthot Int 2012; 36: 125–130.
Arazpour M, Hutchins SW, Bani MA . The efficacy of powered orthoses on walking in persons with paraplegia. Prosthet Orthot Int 2014; 39: 90–99.
Petrofsky J, Smith JB . Physiologic costs of computer-controlled walking in persons with paraplegia using a reciprocating-gait orthosis. Arch Phys Med Rehabil 1991; 72: 890–896.
Kang SJ, Ryu JC, Moon IH, Kim KH, Mun MS (eds). Walker Gait Analysis of Powered Gait Orthosis for Paraplegic. International Federation for Medical & Biological Engineering (IFMBE), seoul, korea; 14(5), Track 16, 2889–2891, 2000.
Arazpour M, Chitsazan A, Hutchins SW, Ghomshe FT, Mousavi ME, Takamjani EE et al. Evaluation of a novel powered hip orthosis for walking by a spinal cord injury patient: a single case study. Prosthet Orthot Int 2012; 36: 105–112.
Arazpour M, Bani M, Hutchins S, Jones R . The physiological cost index of walking with mechanical and powered gait orthosis in patients with spinal cord injury. Spinal Cord 2012; 51: 356–359.
Akahira H, Yamaguchi Y, Nakazawa K, Ohta Y, Kawashima N . Effect of dynamic knee motion on paralyzed lower limb muscle activity during orthotic gait: a test for the effectiveness of the motor-assisted knee motion device. J Nov Physiother S 2012; 1: 2.
Winchester P, Carollo J, Parekh R, Lutz L, Aston J . A comparison of paraplegic gait performance using two types of reciprocating gait orthoses. Prosthet Orthot Int 1993; 17: 101–106.
Leung AK, Wong AF, Wong EC, Hutchins SW . The physiological cost index of walking with an isocentric reciprocating gait orthosis among patients with T12–L1 spinal cord injury. Prosthet Orthot Int 2009; 33: 61–68.
Rasmussen AA, Smith KM, Damiano DL . Biomechanical evaluation of the combination of bilateral stance-control knee-ankle-foot orthoses and a reciprocating gait orthosis in an adult with a spinal cord injury. J Prosthet Orthot 2007; 19: 42–47.
Inman V, Ralston H, Todd F . Human Walking. Williams and Wilkins: Baltimore,. 1981.
Yakimovich T, Lemaire E, Kofman J . Engineering design review of stance-control knee-ankle-foot orthoses. J Rehabil Res Dev 2009; 46: 257.
Scivoletto G, Petrelli A, Di Lucente L, Giannantoni A, Fuoco U, D'Ambrosio F et al. One year follow up of spinal cord injury patients using a reciprocating gait orthosis: preliminary report. Spinal Cord 2000; 38: 555–558.
Sykes L, Edwards J, Powell E, Ross E . The reciprocating gait orthosis: long-term usage patterns. Arch Phys Med Rehabil 1995; 76: 779–783.
Donelan JM, Kram R, Kuo AD . Mechanical work for step-to-step transitions is a major determinant of the metabolic cost of human walking. J Exp Biol 2002; 205: 3717–3727.
Gottschall JS, Kram R . Energy cost and muscular activity required for propulsion during walking. J Appl Physiol 2003; 94: 1766–1772.
Neptune RR, Kautz S, Zajac F . Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J Biomech 2001; 34: 1387–1398.
Capaday C . The special nature of human walking and its neural control. Trends Neurosci 2002; 25: 370–376.
Dietz V, Müller R, Colombo G . Locomotor activity in spinal man: significance of afferent input from joint and load receptors. Brain 2002; 125: 2626–2634.
Grey MJ, Mazzaro N, Nielsen JB, Sinkjær T . Ankle extensor proprioceptors contribute to the enhancement of the soleus EMG during the stance phase of human walking. Can J Physiol Pharmacol 2004; 82: 610–616.
MARZANO R . Orthotic considerations and footwear modifications following ankle fusions. Techn Foot Ankle Surg 2002; 1: 46–49.
Spadone R, Merati G, Bertocchi E, Mevio E, Veicsteinas A, Pedotti A et al. Energy consumption of locomotion with orthosis versus Parastep-assisted gait: a single case study. Spinal Cord 2003; 41: 97–104.
Ferguson K, Polando G, Kobetic R, Triolo R, Marsolais E . Walking with a hybrid orthosis system. Spinal Cord 1999; 37: 800–804.
Marsolais E, Kobetic R, Polando G, Ferguson K, Tashman S, Gaudio R et al. The Case Western Reserve University hybrid gait orthosis. J Spinal Cord Med 2000; 23: 100.
Hardin E, Kobetic R, Murray L, Corado-Ahmed M, Pinault G, Sakai J et al. Walking after incomplete spinal cord injury using an implanted FES system: a case report. J Rehabil Res Dev 2007; 44: 333.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Arazpour, M., Samadian, M., Ebrahimzadeh, K. et al. The influence of orthosis options on walking parameters in spinal cord-injured patients: a literature review. Spinal Cord 54, 412–422 (2016). https://doi.org/10.1038/sc.2015.238
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.238
