
Abstract
Study design:
A cross-sectional study.
Objectives:
This study was performed for epidemiological assessment of Iranian Traumatic Spinal Cord Injuries (TSCI), referred to a specialized spine center.
Setting:
Patient recruitment and evaluations were conducted at the Brain and Spinal Injury Research Center, Tehran, Iran.
Methods:
This study was performed from September 2011 to March 2015 on 1137 consecutive TSCIs. History, clinicoradiological findings as well as chronic complications and social integration were recorded. The capture–recapture method was used to calculate a rough estimation of TSCI prevalence in Tehran Province.
Results:
Our report includes 1137 cases with a mean age of 29.1 years (s.d.=11.2 year)—79.2% of them being male (M/F=3.8/1). Rough estimation of TSCI prevalence in Tehran province was 2.36 per 10 000 population. Regarding etiology, 61.8% were due to motor vehicle accident (MVA), followed by falling 24.5%, heavy drop 5.2%, violence 3.8%, sport 2.8% and others causes 1.9%. Regarding injury level, 31.5% were cervical, 57.9% thoracic and 10.6% lumbar. Complete lesions were 53.5% of patients and 46.5% were incomplete. Most common neurological type was T1-S5 (American Spinal Injury Association Impairment Scale: A, B, C, 61.7%). Most common complications included urinary tract infection followed by pressure sore (grade III and IV, 37.5%), autonomic dysreflexia (37%) and neuropathic pain (31.2%). Substance abuse was observed in 8.8% of cases. Overall, ~25% in our cases were employed after TSCI. Secondary divorce was also much more frequent than normal matched controls.
Conclusion:
MVA was the most common cause for TSCI. The elderly subjects were less frequent among our patients than more developed countries. The high rate of unemployment and divorce in our cases deserves special consideration.
Similar content being viewed by others

Introduction
Traumatic Spinal Cord Injury (TSCI) is a devastating neurological state causing long-term morbidity and marked changes in patients’ lifestyle, especially in the young and healthy population.1 Worldwide epidemiology of TSCI has been reported with spatial and temporal diversities.2 Iran as a Middle East country, with its particular cultural differences, and a history of recent war, may have special TSCI characteristics. A glance at the population age pyramid reveals that Iran has a young population (mean=29.86 years, according to 2011 national census; http://www.amar.org.ir/; 2011) and is among the countries with a high rate of trauma due to motor vehicle and industrial accidents, as well as natural disasters (http://amar.sci.org.ir/; 2011). As expected, the high rate of trauma in Iran is associated with high rate of TSCI, which demands meticulous epidemiological evaluation.3 The worldwide distribution of TSCI has been reported elsewhere, with a variable etiological spectrum including motor vehicle accidents (MVAs), falling, sports, violence (gunshot, stab wound) and others.4 In developed countries such as Canada, USA and Italy, MVA accounts for most TSCIs,5, 6, 7 whereas falling (especially in youngster) has a far more important role for TSCI in the developing countries.8 Determining national TSCI epidemiology needs a sophisticated registry system to obtain exact epidemiological information with temporal profiles.9 In Iran, some studies have been conducted in this field, but it still does not draw an appropriate image of TSCI status nationwide.10 Low sample size, focusing on the capital and not reporting detailed etiological and neurological findings are among limitations in this regard. Therefore, the role of different etiologies for Iranian TSCI still remains unclear.
Major complications are also quite common throughout patients’ life as secondary morbidities associated with TSCI.11 These complications make TSCI among the most costly human maladies;12 therefore, their epidemiological evaluation is a necessity for proper health-care planning.13
Furthermore, social impacts of TSCI should be addressed for the caregivers and health policy makers for better strategic planning.14 As a result, further indepth evaluation of TSCI characteristics in Iran in a greater scale is a necessity. Tertiary spine centers with wide spread patient referral could be a good source for obtaining representative samples, until national registries are available.15 Moreover, as a temporary measure, employing the capture–recapture method16 would yield a rough estimation of the TSCI prevalence in the studied subpopulation.
In this study, the referred patients to Brain and Spinal Injuries Research Institute as a specialized spine center, for outpatient rehabilitation programs, were evaluated to further determine the impact, demographic and clinical features of TSCI. Also, we have reported a rough estimation of TSCI prevalence in Tehran province (the most crowded province with approximately one-fifth of the total Iranian population).
Materials and methods
This cross-sectional study was performed on TSCI patients referred to Brain and Spinal Injury Research Center center, which began its services since 2005 for TSCI subjects. The center had been introduced to TSCI patients, and acute care spine centers, as a specialized facility for rehabilitation since 2007. These cases had been referred from all provinces over the country for outpatient rehabilitation programs, monitoring of health indices and chronic complications of TSCI. Most of these cases had not undergone the early optimal postacute rehabilitation program. Also, prognostication of neurological outcome was an important question for many of these cases. In this center, patients had the opportunity to participate in multidisciplinary outpatient and inpatient programs for TSCI. The outpatient multidisciplinary team studied patients recruited from September 2011 to March 2015 among those referred for rehabilitation programs from 32 provinces. Institutional Review Board of Tehran University of Medical Sciences had approved the study.
All the participants had informed consent for participation in the study, and a medical record for documenting their TSCI, and were assured that their information would remain confidential. Demographic and background data as well as neurological status were obtained from the patients by two separate trained research assistants. Data recheck was performed to ensure prevention of possible random errors. Each case was examined by two neurosurgeons for at least 30 min to determine detailed neurological characteristics of injury including level and American Spinal Injury Association Impairment Scale (AIS). Meanwhile, classification of spinal injury mechanism based on either sub-axial injury classification and severity score17 or thoracolumbar injury classification and severity score18 was performed according to imaging and medical records. Patients were registered in the database, regardless of their willingness to join the outpatient or inpatient rehabilitation programs. The patients’ data were recorded in the registration software (Microsoft Office Access 2007, Redmond, WA, USA) on presentation. Missing parameters of the patients’ records were completed in their consecutive visits. The geographical distribution of the provincial residence of our patients was recorded, and the referral frequencies from 31 different provinces were recorded. As a sampling method, we employed the capture–recapture technique, to estimate point prevalence of TSCI in Tehran province. The study cases formed the first sample, and the second sample was obtained from the database of ‘Protection Center of Spinal Cord Disabled of Iran’.
Variables included gender, age, marital status, etiology, education level, occupational status, duration of injury, neurological level, spinal pathology, severity of injury and complications. The neurological level and severity of TSCI were categorized according to standard protocols recommended by Wyndaele19 and Burns.20 Complications were evaluated as follows: neuropathic pain by Visual Analogous Scale, spasticity by Modified Ashworth Scale, depression categories by Beck Depression Index and pressure ulcers (PUs) graded from I to IV by the classification scheme of Ennis and Sarmiento. We used the Petersen statistic for population size estimation in the capture–recapture method. Point prevalence of TSCI in Tehran province was calculated according to the following formula:

In these formulae, τ̂ represents estimated total number of TSCI in Tehran province; x represents the number of overlapped cases between the two samples; y and x represent the total number of cases in each sample, and finally P̂ represents the estimated prevalence of TSCI in Tehran province.
Clinically relevant associations between categorical variables were assessed by χ2 or Fisher’s Exact test, if indicated. The data analyses were performed with SPSS software version 22 (IBM, Chicago, IL, USA). A P-value <0.05 was considered as significant.
Results
Among a total of 1215 patients with TSCI referred to Brain and Spinal Injury Research Center center, 78 cases were excluded because of either non-traumatic SCI (68 cases) or a lack of informed consent for the study (10 cases). The study was performed on 1137 cases with TSCI. Missing parameters of 12 cases were completed in their consecutive visits. The geographical distribution of relative frequency (number of referred cases/province population) of referred TSCIs has been depicted in Figure 1.

Geographic distribution of spinal cord injury patients in 31 Iranian provinces.
By the capture–recapture sampling method, the point prevalence of TSCI in Tehran province was estimated. The number of cases in our series from Tehran province was 218 cases. The second sample for capture–recapture analysis was obtained from ‘Protection Center of Spinal Cord Disabled of Iran’ database for Tehran province (1256 cases). The two centers overlapped in 95 cases. Peterson statistics in our cases for τ̂ and P̂ yielded the following:
 (estimation of total number of TSCI in Tehran province)
(estimation of total number of TSCI in Tehran province)

(in 10 000 population, 95% confidence interval=2.02–2.71).
Dividing the number of our cases from Tehran province, by the total estimation of the province (see Results), shows that we are reporting about one-thirteenth of the TSCI population of Tehran province (218/2882).
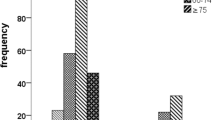
The demographic and background data have been shown in Table 1. The mean age of our cases was 29.1 (s.d.=11.2) years, 50% of them being between ages 21.6 and 35.7 years, and 79.2% were males (M/F=3.8/1). There was not a significant age difference between the males and females (P=0.615). As seen in Figure 2, histogram of frequency for age at the time of injury shows a unimodal pattern. The mean duration of TSCI in our patients was 29.3 months (s.d.=27.7). The mean education year was 9.54 years (range: 0–19 years), and ~7.0% were illiterate (Table 1). As shown in Table 1, ~56.8% of patients were married. Regarding the impact of TSCI on marital status at the time of assessment, the percentage of divorce and/or emotional separation was 6.5% in males and 9.3% in females after TSCI. This figure was 0.67% for males and 1.4% for females in the Iranian general population (>10 years of age; http://www.amar.org.ir/; 2011). As seen that the prevalence of divorce in TSCI is much more than general population. The mean age of divorced cases was significantly lower than that of non-divorced cases (32.8 vs 34.8 years; P=0.037). The higher the level of injury, the more was the divorce percentage (P=0.097). Multiple logistic regression analysis revealed that females had 1.42 (95% confidence interval=0.81–2.5) times more chance to be divorced or separated in comparison with males adjusted for age, education and occupation (P=0.11). The most common cause of injury was MVA (61.8%) followed by falls (24.5%), heavy drop (5.2%), violence (3.8%), sports (2.8%) and others (1.9%). Different mechanisms for MVA included car (46.5%), bike (11.3%) and pedestrian (4.0%) accidents. Surprisingly, walnut trees were a common cause for falling and included 72% of all falls from trees (9.0% of all falls). Different etiologies for sport injuries included diving (2%), gymnastics (0.2%), wrestling (0.1%) and others (0.5%).

Age distribution of the patients.
The occupational status of our patients has been tabulated in Table 2. About 35.1% of cases did have an independent income source to live (employed, retired and housekeeper), whereas 64.9% were dependent either on their family support or social welfare and insurance organizations for their care costs. The more severe and rostral the TSCI, the higher was the prevalence of unemployment (P<0.001). Accordingly, the highest prevalence of unemployment was found in patients with complete tetraplegia (78.9%).
Overall, most participants had thoracic cord injuries (57.9%) followed by cervical lesions (31.5%). Figure 3 shows distribution of neurological levels in our patients. As shown, a bimodal distribution with two peaks at C5 (11.8 %) and T12 (17.0 %) levels is observed. The most common morphology for the spinal injury was facet dislocation for cervical and translation rotation for thoracolumbar injuries (Table 3). Spinal Cord Injury Without Radiological Abnormality (SCIWORA) was found in 6.15% of all participants (51.4% cervical and 48.6% thoracic). Childhood TSCIs (⩽15 years) were 74 cases (6.7%). In children, the etiologies were MVA (68.5%), child abuse (12.3%), fall (11.0%), sport (5.5%) and heavy drop (2.7%). Also, SCIWORA was the most common mechanism for all childhood TSCI (46.4%). Childhood SCIWORA was mostly due to MVA (73.2%), followed by falling (16.9%). Regarding the severity of TSCI in children, ~56.7% were AIS A. All child abuses had a penetrative etiology in our cases—five cases due to bullet and four cases due to stab wound.

Bar chart for frequency distribution according to the neurological level of the injury.
According to Wyndaele categorization (Table 4), as expected, most participants (61.7%) belonged to the third group (that is, injury level T1-S5 with AIS A, B or C). In the same way, according to Burns classification (Table 5), the most common category in our participants was complete paraplegia (43.6%).
Falling and sports as the etiology for TSCI were much more common in men compared with women (28.0% vs 13.6% and 3.5% vs 0.4%, respectively; P<0.001). There was a significant association between age and etiology (P<0.001). Falling was more common (48.4 vs 11.0%) in older participants (⩾46 years) in comparison with children (⩽15 years). With increasing years of education, sport-related injuries became more common, whereas violence and heavy drop became less common (P=0.022). In illiterate subjects, there was no case of sport-related injuries, whereas 5.5% of TSCI in patients with university education was athletics. In contrast to all other causes, incomplete tetraplegia was the most common category in sport-related injuries (75.0%), and thoracic lesions were very rare in these patients (6.3%, P<0.001).
Frequencies of various complications after TSCI in our patients have been tabulated in Table 6. The most common complications after TSCI were PUs (37.5%, grade III or IV), followed by autonomic dysreflexia (37%) for lesions above T6. Smoking was observed in 16.0% of all subjects; the mean (pack/year) for smokers was 5.03 (s.d.=5.59). Illicit drug abuse following TSCI was observed in 8.8% (mostly opium 8.7%, and stimulants 0.1%), whereas alcohol abuse was found in 3.2% of cases.
Discussion
Epidemiological studies for TSCI show significantly different indices among various societies.2 Information about these differences helps health policy makers make more efficient decisions for that region.13 The obtained data may be of benefit for developing and even developed countries.8 Most epidemiological studies on TSCI give an estimation for disease prevalence or incidence in their target population. In a systematic review for worldwide TSCI epidemiology, prevalence of TSCI was reported to be 236.0–1298.0 per million population. Although the current study may not provide the exact figures for TSCI incidence and prevalence in Iran, nevertheless a rough estimation of TSCI prevalence in Tehran was 236 per million population. Despite a high national rate for accidents, this relatively low figure in comparison with most developed countries may be due to higher mortality at the accident scene, and acute care service. Accordingly, in a population-based study in Tehran, the point prevalence of TSCI was estimated to be 440 per million population.10 The discrepancy may be due to the fact that our estimation is for Tehran province, whereas that report was for Tehran city only.
The geographical distribution of TSCI is very important for planning establishment of the outpatient care centers. Distribution of our cases in Iran (Figure 1) shows the referral pattern from various provinces. The cases had been referred more frequently from less privileged cities, situated over the Alborz and Zagros mountains. This may be a notification for the necessity of building local spine centers in those cities.
The mean age in our cases was 29.1 years and 56.8% of our cases were between 16 and 30 years, and this is in concordance with reported age (between 15 and 30 years) from Canada21 but still less than world average (33 years).4 Many developed countries have reported much older mean age for their TSCI in some centers—for example, 50 years for an acute trauma center in Canada.15 Our finding shows a propensity for the youngster in Iran and the necessity of considering preventive measures to be started for lower age groups. Also, the high costs of care in the younger population due to longer survival is a special concern in this regard.22 Studies have reported a bimodal pattern with two peaks at 15–29 and above 65 years of age.23 However, our study shows a single peak at late 20s. This difference may be due to the very low number of elderly people in our study, which in turn could be a result of either lower survival in older Iranian spinal cord injury patients or accessibility issues in older cases to attend our center.
Regarding gender, 79.2% of our cases were males, and this figure is at the level of the world average (79.8%).4 Despite cultural differences between developed and developing countries, male-to-female ratio is nearly the same worldwide.
In our study, falling and sport have been reported to be more common in men (M/F: 7.65/1, 31.0/1 respectively, P<0.001), which is quite different with other reports where women have fairly equal frequencies,24 and this may be due to cultural differences regarding female lifestyle in Iran. Again falling has been reported as a major etiology for the elderly (65+ years) in developed countries.24 Although in our cases falling was more common in older ages, nevertheless we had very few cases in the elderly (65+ years) because TSCI in Iran is mainly a disorder of youngster. Overall, falling was the etiology of TSCI in 24.5% of our cases. High falls (work related) in our cases were ~86.3% of all the falls, and this is in contrast to developed countries where work-related falls were less common, ~25% (building (16%), ladder (9%) in those aged 16–45 years). Low falls in the elderly (slipping, tripping, stumbling, stairs and steps) have been reported to constitute ~36% of the falls in developed countries.25
MVAs have been the most common etiology in our cases, and this pattern is a common finding in other studies. The percentage of MVA as the cause of TSCI was 61.8% in our cases, and this figure is very high with respect to developed countries (38%: North America and 47% United Kingdom). Some countries in the Middle East and Africa also have reported very high figures—Saudi Arabia (85%),26 Qatar (72%),27 Kuwait (63.3%),28 Botswana (68%) 29and Nigeria (88.8%).30 On the other hand, developed countries report a much less figure for MVA etiology—North America (38%),22 Iceland (42.5),31 Norway (40.8%),32 Spain (40.9%)33and United Kingdom (47%).1 Also, in some countries, the figure is very low for MVA, such as India (28%)34and Bangladesh (18%),35 which may be due to less usage of motor vehicles for their land transport. The high percentage of MVA as etiology of TSCI in Iran36 demands nationwide effort for considering preventive measures.
Education level may be of concern as a risk factor for TSCI—for example, violence and heavy drop were more common in less educated subjects, whereas sport/leisure-related injuries were more common in those with university education. In our study, violence and heavy drop were inversely related to literacy, in contrast to sport injuries, which were directly correlated with the education level. PubMed search did not disclose a similar association reported by other studies.
The relative frequency of cervical cases in our study (31.5%) was much less than developed countries (59–82%);22, 37, 38 this may be due to older age at the time of injury,39 as well as better survival of cervical cases in those countries.40 This lower frequency in our cases also may be due to accessibility issues.
The bimodal distribution of the neurological level has been mentioned elsewhere;37 the reported C5 and T12 peaks were also found in our study. In addition, another minor peak was found at the T6 level not reported in other studies. Regarding morphology of spinal injuries in the cervical region, the percentage of facet dislocations in our study was 64.7%, whereas this figure was 32.1% in other studies.41
Regarding complications of TSCI, PUs have been the second most common cause for hospitalization in patients with TSCI after urinary tract infections.42 Excluding urinary tract infections, in the current study, PUs have been the most common complication (67.8%), followed by neuropathic pain (66.1% overall, 31.2% Visual Analogous Scale ⩾50), and autonomic dysreflexia (37.0%). The incidence of moderate-to-severe neuropathic pain (Visual Analogous Scale ⩾50) has been reported to be ~77.7% in other studies.43 Significant spasticity defined as Modified Ashworth Scale ⩾3 was found in 25.4% of our cases. Overall, spasticity has been reported up to 70% of TSCI, but the observed Modified Ashworth Scale scoring has not been clarified.44
The female preponderance on divorce and/or emotional separation may be explained on the basis of more familial adherence among the partners of the male TSCI cases in Iran. The high divorce rate found in the young subjects may be due to more economic vulnerability in young couples.
Regarding social integration, 86 (4%) of them had been employed before injury. However, after ~29 months post TSCI, 21.9% of our cases were employed (C1–C4: 1%, C5–C8:11.2%, T1-S1: 68.8% for AIS A, B and C, cases; AIS D and E: 19%). The 1-year employment figure in Canada has been 32%, whereas 62% of their cases had been employed before TSCI,45 their employment rate was near 50%, this figure was 25% for Iranian TSCIs. Risk factors for unemployment after TSCI are reported to be older age, not being married, unmet SCI needs, as well as lower functional independence measure score, and no participation in social roles.45, 46 The same trends were observed in our cases as the rational for lower employment rate.
There are some limitations in generalizibity of our results to the Iranian TSCI population, because our sampling method was not population based; however, the sample is to a large extent a representative sample for TSCI in Iran. Also, there are some limitations in our study for assumptions of the capture–recapture method, such as independence of samples and equal chance to be included in each sample.
Conclusion
The study shows a young age for victims of TSCI in Iran—MVA being its most common cause. The rough estimation of TSCI prevalence needs sophisticated registry system. The elderly subjects were less frequent than in the developed countries. The high rate of unemployment and divorce in our cases deserves especial consideration for social integration and supporting programs.
Data archiving
There were no data to deposit.
References
Pickett W, Simpson K, Walker J, Brison RJ . Traumatic spinal cord injury in Ontario, Canada. J Trauma 2003; 55: 1070–1076.
Furlan JC, Sakakibara BM, Miller WC, Krassioukov AV . Global incidence and prevalence of traumatic spinal cord injury. Can J Neurol Sci 2013; 40: 456–464.
Bakhtiyari M, Mehmandar MR, Mirbagheri B, Hariri GR, Delpisheh A, Soori H . An epidemiological survey on road traffic crashes in Iran: application of the two logistic regression models. Int J Inj Contr Saf Promot 2014; 21: 103–109.
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O'Connor KC et al. Traumatic spinal cord injury in the United States, 1993-2012. Jama 2015; 313: 2236–2243.
Aito S, Tucci L, Zidarich V, Werhagen L . Traumatic spinal cord injuries: evidence from 30 years in a single centre. Spinal Cord 2014; 52: 268–271.
Botterell EH, Jousse AT, Kraus AS, Thompson MG, WynneJones M, Geisler WO . A model for the future care of acute spinal cord injuries. Can J Neurol Sci 1975; 2: 361–380.
Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH . Review paper: epidemiology of traumatic spinal cord injury: comparisons between developed and developing countries. Asia Pacific J Public Health 2010; 22: 9–18.
Noonan VK, Kwon BK, Soril L, Fehlings MG, Hurlbert RJ, Townson A et al. The Rick Hansen Spinal Cord Injury Registry (RHSCIR): a national patient-registry. Spinal Cord 2012; 50: 22–27.
Rahimi-Movaghar V, Saadat S, Rasouli MR, Ganji S, Ghahramani M, Zarei MR et al. Prevalence of spinal cord injury in Tehran, Iran. J Spinal Cord Med 2009; 32: 428–431.
DeVivo MJ . Causes and costs of spinal cord injury in the United States. Spinal Cord 1997; 35: 809–813.
Johnson RL, Brooks CA, Whiteneck GG . Cost of traumatic spinal cord injury in a population-based registry. Spinal Cord 1996; 34: 470–480.
Post MW, Adriaansen JJ, Charlifue S, Biering-Sorensen F, van Asbeck FW . Good validity of the international spinal cord injury quality of life basic data set. Spinal Cord 2015 (e-pub ahead of print 23 June 2015; doi: 10.1038/sc.2015.9).
Powell-Cope G, Moore DH, Weaver FM, Thomason S . Perceptions of practice guidelines for people with spinal cord injury. Rehabil Nurs 2015; 40: 100–110.
Kattail D, Furlan JC, Fehlings MG . Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma 2009; 67: 936–943.
Chiu WT, Dearwater SR, McCarty DJ, Songer TJ, LaPorte RE . Establishment of accurate incidence rates for head and spinal cord injuries in developing and developed countries: a capture-recapture approach. J Trauma 1993; 35: 206–211.
Patel AA, Dailey A, Brodke DS, Daubs M, Anderson PA, Hurlbert RJ et al. Subaxial cervical spine trauma classification: the Subaxial Injury Classification system and case examples. Neurosurg Focus 2008; 25: E8.
Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R et al. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disorders Techniques 2005; 18: 209–215.
Wyndaele JJ . Standardization of reporting data in the 'Spinal cord' journal. Spinal Cord 2012; 50: 483.
Burns S, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M et al. International standards for neurological classification of spinal cord injury, revised 2011. Topics Spinal Cord Inj Rehabil 2012; 18: 85–99.
McCammon JR, Ethans K . Spinal cord injury in Manitoba: a provincial epidemiological study. J Spinal Cord Med 2011; 34: 6–10.
National Spinal Cord Injury Statistical Center. Spinal Cord Injury Facts and Figures at a Glance. J Spinal Cord Med 2013; 36: 1–2.
van den Berg ME, Castellote JM, Mahillo-Fernandez I, de Pedro-Cuesta J . Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology 2010; 34: 184–192.
Pickett GE, Campos-Benitez M, Keller JL, Duggal N . Epidemiology of traumatic spinal cord injury in Canada. Spine (Phila Pa 1976) 2006; 31: 799–805.
Chen Y, Tang Y, Allen V, DeVivo MJ . Fall-induced spinal cord injury: External causes and implications for prevention. J Spinal Cord Med 2015.
Alshahri SS, Cripps RA, Lee BB, Al-Jadid MS . Traumatic spinal cord injury in Saudi Arabia: an epidemiological estimate from Riyadh. Spinal Cord 2012; 50: 882–884.
Mena Quinones PO NM, Al Bader Kl, Al Muraikhi AE, Al Kahlout SR . Traumatic spinal cord injury in Qatar: an epidemiological study. Middle East J Emerg Med 2002; 2: 1–4.
Raibulet TFS, Khamees MF, Eyadeh AA . Spinal Cord Injury Patients in the Physical Medicine and Rehbilitation Hospital, Kuwait - A nine-year retrospective study. Kuwait Med J 2001; 33: 211–215.
Lofvenmark I, Norrbrink C, Nilsson-Wikmar L, Hultling C, Chakandinakira S, Hasselberg M . Traumatic spinal cord injury in Botswana: characteristics, aetiology and mortality. Spinal Cord 2015; 53: 150–154.
Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO . Profile of spinal injuries in Lagos, Nigeria. Spinal Cord 2009; 47: 134–137.
Knutsdottir S, Thorisdottir H, Sigvaldason K, Jonsson H Jr., Bjornsson A, Ingvarsson P . Epidemiology of traumatic spinal cord injuries in Iceland from 1975 to 2009. Spinal Cord 2012; 50: 123–126.
Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M . A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010; 48: 313–318.
Perez K, Novoa AM, Santamarina-Rubio E, Narvaez Y, Arrufat V, Borrell C et al. Incidence trends of traumatic spinal cord injury and traumatic brain injury in Spain, 2000-2009. Accid Analy Prev 2012; 46: 37–44.
Mathur N, Jain S, Kumar N, Srivastava A, Purohit N, Patni A . Spinal cord injury: scenario in an Indian state. Spinal Cord 2015; 53: 349–352.
Hoque MF, Grangeon C, Reed K . Spinal cord lesions in Bangladesh: an epidemiological study 1994 - 1995. Spinal Cord 1999; 37: 858–861.
Yousefzadeh Chabok S, Safaee M, Alizadeh A, Ahmadi Dafchahi M, Taghinnejadi O, Koochakinejad L . Epidemiology of traumatic spinal injury: a descriptive study. Acta Med Iran 2010; 48: 308–311.
Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX . Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. J Spinal Cord Med 2011; 34: 388–394.
Nijendijk JH, Post MW, van Asbeck FW . Epidemiology of traumatic spinal cord injuries in The Netherlands in 2010. Spinal Cord 2014; 52: 258–263.
Bellucci CH, de Castro Filho JE, Gomes CM, de Bessa J Jr., Battistella LR, Rubio de Souza D et al. Contemporary trends in the epidemiology of traumatic spinal cord injury: changes in age and etiology. Neuroepidemiology 2015; 44: 85–90.
Krause JS, Zhai Y, Saunders LL, Carter RE . Risk of mortality after spinal cord injury: an 8-year prospective study. Arch Phys Med Rehabil 2009; 90: 1708–1715.
Wilson JR, Vaccaro A, Harrop JS, Aarabi B, Shaffrey C, Dvorak M et al. The impact of facet dislocation on clinical outcomes after cervical spinal cord injury: results of a multicenter North American prospective cohort study. Spine (Phila Pa 1976) 2013; 38: 97–103.
Cardenas DD, Hoffman JM, Kirshblum S, McKinley W . Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil 2004; 85: 1757–1763.
Mann R, Schaefer C, Sadosky A, Bergstrom F, Baik R, Parsons B et al. Burden of spinal cord injury-related neuropathic pain in the United States: retrospective chart review and cross-sectional survey. Spinal Cord 2013; 51: 564–570.
Rekand T, Hagen EM, Gronning M . Spasticity following spinal cord injury. Tidsskr Nor Laegeforen 2012; 132: 970–973.
Jetha A, Dumont FS, Noreau L, Leblond J . A life course perspective to spinal cord injury and employment participation in Canada. Top Spinal Cord Inj Rehabil 2014; 20: 310–320.
Murphy G, Middleton J, Quirk R, De Wolf A, Cameron ID . Prediction of employment status one year post-discharge from rehabilitation following traumatic spinal cord injury: an exploratory analysis of participation and environmental variables. J Rehabil Med 2009; 41: 1074–1079.
Acknowledgements
We thank ‘Protection Center of Spinal Cord Disabled of Iran’ for their kind support of the study. Also, we thank Dr Ahmad Audeh, Asal Derakhshanrad, MSc, and Dr Shadi Derakhshanrad for their kind contribution to the program. Also, our thanks go to Dr Abolghassem Nikfallah, Dr Mohsen Maghari, Dr Amirhossein Tavakkoli, Dr Seyed Hassan Emami Razavi and Dr Abbas Norouzi Javdan for their participation in the multidisciplinary team and their contributions to the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Derakhshanrad, N., Yekaninejad, M., Vosoughi, F. et al. Epidemiological study of traumatic spinal cord injuries: experience from a specialized spine center in Iran. Spinal Cord 54, 901–907 (2016). https://doi.org/10.1038/sc.2016.10
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.10
This article is cited by
-
Adopting and adapting clinical practice guidelines for timing of decompressive surgery in acute spinal cord injury from a developed world context to a developing region
Acta Neurochirurgica (2023)
-
A systematic review and meta-analysis of the global epidemiology of pediatric traumatic spinal cord injuries
European Journal of Pediatrics (2023)
-
Development of Persian version of the Spinal Cord Independence Measure III assessed by interview: a psychometric study
Spinal Cord (2018)
-
Incidence of acute spinal cord injury in the Czech Republic: a prospective epidemiological study 2006–2015
Spinal Cord (2017)
