
Abstract
Background:
Preterm infants are at increased risk of sudden infant death syndrome (SIDS). Use of a dummy/pacifier is thought to be protective against SIDS; accordingly, we assessed the effects of dummy/pacifier use on blood pressure, cerebral oxygenation, and heart rate control over the first 6 mo of life after term corrected age (CA) when SIDS risk is greatest.
Methods:
Thirty-five preterm infants were studied longitudinally at 2–4 wk, 2–3 mo, and 5–6 mo CA. Cardiac control was assessed from spectral indices of heart rate variability (HRV) in the low frequency (LF) and the high frequency (HF) range, and the ratio of HF/LF indicating sympathovagal balance was calculated.
Results:
Overall, at 2–3 mo, mean arterial pressure was significantly higher in the supine position in dummy/pacifier users in both quiet sleep (70 ± 2 vs. 60 ± 2 mm Hg; P < 0.05) and active sleep (74 ± 3 vs. 69 ± 2 mm Hg; P < 0.05). Dummy/pacifier users had higher LF HRV and LF/HF ratio and lower HF HRV.
Conclusion:
Dummy/pacifier use increased blood pressure during sleep, at the age of greatest SIDS risk. Overall, LF HRV was elevated and HF HRV reduced in dummy/pacifier users, suggesting that dummy use alters cardiac control in preterm infants.
Similar content being viewed by others

Main
The rates of preterm birth are increasing and now account for over 10% of live births annually worldwide (1). Preterm infants are at significantly increased risk of the sudden infant death syndrome (SIDS) (2,3), with 29% of SIDS victims being born preterm (4). SIDS is believed to involve an uncompensated cardiovascular event during sleep, in conjunction with failure of the life-saving arousal response (5,6). We have previously shown that preterm infants exhibit immature control of heart rate (HR) and blood pressure which persists for 6 mo past term-equivalent age and have suggested that this may underlie their increased risk for SIDS (7,8,9). Furthermore, we have recently reported that blood pressure and cerebral oxygenation are reduced in preterm compared with age-matched term infants, and this is most marked when they sleep prone (10), the major risk factor for SIDS.
Epidemiological studies have consistently shown that infants who regularly use a dummy or pacifier are at a lower risk for SIDS (11) even in prone sleeping infants (12). Reflecting the strength of this evidence, the American Academy of Pediatrics has recommended that dummy/pacifiers are offered to infants during sleep after breastfeeding has been established (13). However, this recommendation has not been adopted by all countries (11). In part, the reluctance to recommend dummy/pacifier use has been due to the lack of evidence of the mechanism underpinning the protective effects, particularly as the dummy/pacifier falls out of the mouth soon after sleep onset (14,15). Furthermore, there are concerns that dummy/pacifier use may adversely impact on breastfeeding (16).
In term-born infants, early studies have demonstrated that sucking on a dummy/pacifier was associated with increased sympathetic activation during sleep (17). Recently, we have shown that term infants who regularly use a dummy/pacifier have a higher blood pressure and increased heart rate variability (HRV), indicating increased sympathetic tone, which may serve as a protective mechanism against possible hypotension during sleep and thus be protective against SIDS (18). To date, no studies have examined the effects of dummy/pacifier use on blood pressure, cardiovascular control, and cerebral oxygenation in preterm infants across the age when SIDS risk is greatest.
Thus, we aimed to assess heart rate, blood pressure, and cerebral oxygenation and heart rate control during prone and supine sleep in preterm infants who regularly used a dummy/pacifier and those who did not across the first 6 mo after term-equivalent age when most SIDS deaths occur. We hypothesized that blood pressure and cerebral oxygenation would be elevated and that heart rate control would be improved in dummy/pacifier users, and these effects would be most marked in the prone sleeping position.
Results
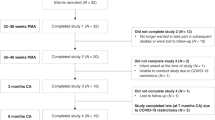
Infants were divided into two groups: those who regularly used a dummy/pacifier (n = 19 at 2–4 wk; n = 22 at 2–3 mo; n = 19 at 5–6 mo) and those who did not (n = 12 at 2–4 wk; n = 6 at 2–3 mo; n = 9 at 5–6 mo). Two dummy/pacifier users were excluded at study 1 and one dummy/pacifier was excluded from study 2 due to lack of suitable data. There were 14 infants who consistently used a dummy/pacifier and 4 infants who consistently did not use a dummy/pacifier at all three studies.
Demographics of the infants studied are presented in Table 1 . There were no differences in the gestational age (GA) at birth, GA, or weight between groups at the time of the three studies. Socioeconomic status was derived from the Australian Bureau of Statistics Index of Relative Socio-economic Advantage/Disadvantage (SEIFA) 2011 national census data based on postal code (19).The SEIFA score has a mean of 1,000 with an SD of 100 and is presented as a raw score, with a higher score being indicative of higher income, education, employment, occupation, and housing. At 2–4 wk and 5–6 mo, those infants who routinely used a dummy came from a higher socioeconomic status. The majority of infants were breastfed in both groups in all three studies; at 5–6 mo, all were receiving solids. Method of feeding was not associated with the use of a dummy/pacifier at any study. There was no difference in total sleep time or time spent awake between the two groups at any age studied.
Effects of Dummy/Pacifier Use on HR, Blood Pressure, and Cerebral Oxygenation
Including all the epochs in dummy/pacifier users at 2–4 wk corrected age (CA) and 5–6 mo CA, there were no differences identified in HR, systolic arterial pressure, mean arterial pressure, diastolic arterial pressure, or tissue oxygenation index (TOI) between infants who regularly used a dummy/pacifier and those who did not in either sleep state or position ( Figure 1 ). At 2–3 mo CA, there was a pattern for dummy/pacifier users to have a lower HR; however, this failed to reach statistical significance in either the prone or supine (P = 0.078) position. Mean arterial pressure was significantly higher at 2–3 mo CA in the supine position in those infants who used a dummy/pacifier compared with those infants who did not in both quiet sleep (QS) (70 ± 2 vs. 60 ± 2 mm Hg; P < 0.05) and active sleep (AS) (74 ± 3 vs. 69 ± 2 mm Hg; P < 0.05). Similarly, systolic arterial pressure and diastolic arterial pressure were also significantly higher (P < 0.05) in the supine position in those infants who used a dummy/pacifier compared with those infants who did not. TOI was not different between the groups in either sleep state or position.

Mean values in active sleep and quiet sleep in the prone and supine positions for heart rate at (a) 2–4 wk, (d) 2–3 mo, and (g) 5–6 mo; mean arterial pressure at (b) 2–4 wk, (e) 2–3 mo, and (h) 5–6 mo; and cerebral oxygenation at (c) 2–4 wk, (f) 2–3 mo, and (i) 5–6 mo corrected age. Dummy/pacifier users are indicated by the black bars and nondummy/pacifier users by the white bars. Values are mean ± SEM. *P < 0.05.
At 2–4 wk and 2–3 mo, sleep state had an effect on mean arterial pressure which was significantly higher in AS compared with QS in both the prone and supine positions in both groups. There were no effects of sleep state on HR or TOI at any age.
When data for the nonsucking epochs only in the dummy/pacifier users were compared with those in nondummy/pacifier users, results were similar with the additional finding that overall HR was also lower in the dummy/pacifier users at 2–4 wk ( Table 2 ).
Effects of Dummy/Pacifier Use on HR Control
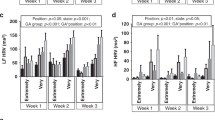
When all epochs were analyzed in dummy users, at 2–4 wk CA, LF HRV and total power were higher in dummy/pacifier users in QS in both the supine and prone positions (P < 0.001 and P < 0.01, respectively) ( Figure 2 ). Additionally, the LF/HF ratio was also higher in dummy/pacifier users in the prone position (P < 0.05). No differences were identified between groups in AS.

Mean values for heart rate variability in the prone and supine positions in active sleep and quiet sleep for low frequency (LF) at (a) 2–4 wk, (e) 2–3 mo, and (i) 5–6 mo; high frequency (HF) at (b) 2–4 wk, (f) 2–3 mo, and (j) 5–6 mo; HF/LF ratio at (c) 2–4 wk, (g) 2–3 mo, and (k) 5–6 mo; and total power at (d) 2–4 wk, (h) 2–3 mo, and (l) 5–6 mo corrected age. Dummy/pacifier users are indicated by the black bars and nondummy/pacifier users by the white bars. Values are mean ± SEM. *P < 0.05; **P < 0.01; †P < 0.001.
At 2–3 mo CA, HF HRV was lower in dummy/pacifier users in QS, reaching significance in the prone position (P < 0.05). The LF/HF ratio was higher in dummy/pacifier users in QS in both the prone (P < 0.05) and supine (P < 0.01) positions. Again, there were no differences between groups in AS.
At 5–6 mo, LF HRV was elevated in the supine position in QS in dummy/pacifier users (P < 0.05). HF HRV was lower in dummy/pacifier users in QS in both positions. Overall, the LF/HF ratio was also elevated in dummy/pacifier users, reaching statistical significance in QS in both the supine and prone positions and in AS in the supine position (P < 0.05 for all).
When data for the nonsucking epochs only in the dummy/pacifier users were compared with those in nondummy/pacifier users, results were similar ( Table 3 ); however, post hoc analysis could not identify where the differences lay. Specifically, at 2–4 wk, overall LF power, LF/HF, and total power were significantly greater in dummy/pacifier users compared with nondummy users in both AS and QS. There were no differences at 2–3 mo. At 5–6 mo, overall HF was significantly lower in dummy/pacifier users compared with nondummy/pacifier users in both the prone (P < 0.001) and supine (P < 0.05) positions, and the LF/HF power ratio overall was significantly greater in dummy/pacifier users compared with nondummy/pacifier users in both the prone (P < 0.05) and supine (P < 0.001) positions.
Discussion
Regular dummy/pacifier use has consistently been shown to be associated with a reduced SIDS risk in epidemiological studies; however, the mechanism for this reduced risk is currently unknown. Preterm infants are at increased risk for SIDS compared with term-born infants. This was the first study to investigate blood pressure, HR, and cerebral oxygenation and heart rate control in preterm infants who regularly used a dummy/pacifier and those who did not. We had hypothesized that to be protective, use of a dummy/pacifier would increase blood pressure, HR, and cerebral oxygenation and improve heart rate control, and this would be most marked in the prone sleeping position. We identified that at 2–3 mo of age, blood pressure was overall significantly higher in both sleep states by 5–10 mm Hg in those infants who regularly used a dummy/pacifier. In contrast, heart rate tended to be lower in dummy/pacifier users, and there was no overall difference in cerebral TOI. Overall, LF HRV was elevated and HF HRV reduced in infants who used a dummy/pacifier, suggesting that dummy/pacifier use alters cardiac control in preterm infants. These findings suggest that use of a dummy/pacifier may be protective through increases in blood pressure and improvement in autonomic control of heart rate. Analysis of our data only during periods of nonsucking in the dummy/pacifier users was consistent with the data when both sucking and nonsucking epochs were included, suggesting that the effects of dummy/pacifier use are not simply related to sucking epochs.
The mechanism responsible for higher blood pressure in dummy/pacifier users is unclear; however, it is possible that active dummy/pacifier sucking may increase overall sympathetic vascular tone contributing to increased vascular resistance and thus elevated blood pressure. It is also possible that increased oscillations in blood pressure due to active sucking may improve baroreflex sensitivity keeping blood pressure within tighter limits. In term infants, we have previously identified that baroreflex sensitivity tended to be higher in conjunction with elevated blood pressure at 2–4 wk of age in those infants who used a dummy/pacifier (18). We have also identified that preterm infants have lower blood pressure and cerebral oxygenation compared with age-matched term-born infants across the first 6 mo of life, and this was most marked when infants slept prone (10). Any factor which increases blood pressure may act to protect preterm infants from any adverse cardiovascular event during sleep. We had hypothesized that dummy/pacifier use would also increase cerebral oxygenation; however, we did not identify any differences between groups at any age studied.
Our finding of an overall elevated LF HRV and total HRV power in dummy/pacifier users at 2–4 wk and increased LF/HF ratio at all three ages particularly in QS suggests that dummy/pacifier users had altered autonomic control of heart rate. The finding of elevated LF HRV suggests that dummy/pacifier users had increased sympathetic activation. At 2–3 and 5–6 mo, these infants also had lower HF HRV indicating reduced parasympathetic activation and a resultant increased LF/HF ratio. In contrast, Franco et al. (17) found that dummy/pacifier users had decreased sympathetic activation and increased parasympathetic activation of HR compared with infants who had never used a dummy/pacifier. We know that postnatal age has a significant effect on autonomic control of HR (8,20) so the differences between our findings and those of Franco et al. may have been due to the wide age range (6–18 wk) of infants they studied. In a similarly designed study in term infants, we have previously shown that HRV was elevated in the supine position but only at 2–4 wk of age (18). The differences in findings between these studies may be due to the innate differences in autonomic control between preterm born infants and those born at term which we have previously reported (8).
A novel aspect of this study was that we followed the infants longitudinally across the first 6 mo of life when 90% of SIDS infants die. Interestingly, we found that dummy/pacifier use was not consistent across the ages, with only 14 infants consistently using a pacifier and 4 infants consistently not using a dummy/pacifier at all three studies. The majority of epidemiological studies have identified that the consistency of pacifier use is important for any protective effect (11). Our analysis took this into account by grouping infants at each age into those who were regularly using a dummy/pacifier at the time of the study and those who did not.
Nonnutritive sucking is a normal reflex in both the fetus and newborn infant, and the pacifier has been used to fulfill this innate desire for more than 2,000 y. It is estimated that about 75% of children in Western countries are offered a dummy/pacifier at some time (21). Surprisingly, the infants from more socioeconomically advantaged families were more likely to be given a dummy/pacifier. However, it must be noted that although this was statistically significant, the differences between the groups were within one SD so were not of any clinical significance. The major reason that infants are given a dummy/pacifier is to soothe them with the aim of increasing sleep time (22). In our study, we found no difference in sleep or awake time between the two groups of infants. Consistent with our findings, previous studies in term-born infants have also found no differences in sleep duration between dummy/pacifier users and nonusers in either overnight (14) or daytime sleep studies (15,23).
In this study, the majority of infants were breastfed at 2–4 wk (23/31) and at 2–3 mo (19/28). Even at 5–6 mo, when all infants had commenced solids, 13 out of 28 infants continued to be breastfed. Concerns have been raised that giving an infant a dummy/pacifier will have adverse effects on the initiation and maintenance of breastfeeding. However, a recent Cochrane review in 1,302 healthy full-term newborns who had initiated breastfeeding found no significant effects of dummy/pacifier use on the duration of breastfeeding (24). Although a small study, our data also suggest that dummy/pacifier use is not detrimental to the initiation or maintenance of breastfeeding.
We acknowledge that there are limitations to this study which may have affected our results. Firstly, the group of infants studied was small, and pacifier use varied across the ages, with few infants not using a pacifier at 2–3 mo of age. Secondly, all the infants studied, despite being born preterm, were at low risk for SIDS, they all routinely slept supine at home, had not been exposed to maternal smoking either before or after birth, and the majority were breastfed. Thirdly, our studies were carried out during the daytime. In young infants, sleep times are scheduled around feeding, and the infants in this study had both a morning and afternoon sleep interrupted by a midday feed when sleeping position was changed. The infants recruited were not clinical subjects referred for a diagnostic sleep study, and carrying out overnight polysomnography would have severely restricted recruitment. Finally, epidemiological studies have identified that the peak in SIDS deaths occurs at a slightly earlier postterm CA, 7–9 wk CA depending on GA at birth, for preterm compared with term infants (25). In this study, we chose to investigate term and preterm infants at similar postterm CAs to enable comparison at equivalent developmental ages (10). It may be that the cardiovascular differences we observed were in fact underestimated as our infants were studied at a slightly older age than that of peak SIDS risk in preterm infants.
In conclusion, dummy/pacifier use in preterm-born infants increased blood pressure during sleep, at the age of greatest SIDS risk. Overall, LF HRV was elevated, HF HRV reduced, and the LF/HF ratio increased in infants who used a dummy suggesting that dummy/pacifier use alters cardiac control in preterm infants. An elevated blood pressure and improved control of heart rate may protect preterm infants from possible hypotension during sleep and thus may play a protective role in the fatal event of SIDS.
Methods
Subjects
Ethical approval was obtained from the Monash Health and Monash University human research ethics committees. Written parental consent was obtained, and no monetary incentive was provided for participation.
Thirty-five preterm infants (21 male, 14 female) born at 26–36 wk of GA (mean GA: 31.2 ± 0.4, mean birth weight: 1,697 ± 92 g) with Apgar scores ranging from 2 to 9 (median: 6) at 1 min and 7 to 9 (median: 9) at 5 min were recruited. Infants were not recruited if they were intrauterine growth restricted and had major congenital abnormalities, a hemodynamically significant patent ductus arteriosus, significant intraventricular hemorrhage (grade III or IV), or chronic lung disease requiring ongoing respiratory stimulant medication or oxygen therapy at term-equivalent age. All infants were appropriately grown for GA, born to nonsmoking mothers, had no family history of SIDS, and routinely slept supine at home.
Twenty-four infants were studied on three occasions at 2–4 wk, 2–3 mo, and 5–6 mo postterm CA; 7 were studied at only 2–4 wk CA, and 4 were studied only at 2–3 mo and 5–6 mo CA.
Protocol
Infants were studied with daytime polysomnography performed between 0900 and 1700 h in a sleep laboratory with constant temperature (22–23 °C), dim lighting, and quiet conditions. Infants slept both prone and supine with sleep position changed following a midday feed, and the initial sleep position randomized between infants and studies.
Electrodes including electroencephalogram (C4/A1 and O2/A1), electrooculogram, submental electromyogram, electrocardiogram, thoracic and abdominal respiratory movements (Resp-ez bands; EPM Systems, Midlothian, VA), and arterial oxygen saturation (Masimo, Frenchs Forest, NSW, Australia) were applied during a morning feed. In addition, blood pressure was measured noninvasively in 1–2-min epochs using a photoplethysmographic cuff (Finapres Medical Systems, Amsterdam, The Netherlands) placed around the infant’s wrist (26). Cerebral TOI % was also measured continuously using near-infrared spectroscopy (NIRO-200 spectrophotometer; Hamamatsu Photonics KK, Tokyo, Japan). Near-infrared spectroscopy enables calculation of cerebral TOI using continuous-wave light emission and detection measured over the frontal region of the infant’s brain, with the detection probe placed 4 cm away from the emission probe. TOI was computed continuously using a spatially resolved spectroscopy algorithm (27) and represents mixed oxygen saturations of all cerebral vascular compartments. Analysis of cerebral TOI was performed on the 1–2-min epochs during which blood pressure was concurrently recorded.
Studies were video recorded and signals were recorded using an E-series sleep recording system with Profusion software (Compumedics, Abbotsford, VIC, Australia) with a sampling rate of 512 Hz.
Data Analysis
In dummy/pacifier users, sucking was confirmed via video recordings and defined if (i) the dummy/pacifier was in the infant’s mouth and (ii) there was a clear increase in EMG during each sucking event. At the completion of each study, data were transferred to LabChart7 software (ADInstruments, Sydney, NSW, Australia) for analysis. Sleep state was defined as either QS or AS according to standard guidelines (28). Beat-to-beat values were calculated for cerebral TOI, blood pressure, and HR; data were averaged for each epoch and pooled for each sleep state and position within each infant. An average of six epochs were analyzed in each sleep state and position for each infant. Data containing movement artifact and epochs where mean arterial pressure lay 1.5 times the interquartile range outside the first and third quartiles were excluded from further analysis (29). Firstly, all available epochs were analyzed in dummy/pacifier users and then subsequently only nonsucking epochs in dummy/pacifier users were analyzed and compared with epochs in nondummy/pacifier users.
Assessment of autonomic control. Spectral analysis techniques were used to assess HRV. The autonomic nervous system mediates oscillations in HR predominantly in the LF and HF frequency spectral ranges. LF changes in HR reflect both sympathetic and parasympathetic activation, whereas vagal (parasympathetic) activity is a major contributor to the HF component. The ratio between the LF and HF spectral power (LF/HF) provides a measure of sympatho-vagal balance (30,31). For HRV the LF (0.04–0.15 Hz) power, reflecting baroreflex activity, the HF power (individualised for each infant depending on respiratory frequency), and total power were calculated (32).
Statistical Analysis
Statistical analysis was performed using SigmaPlot 12.0 analysis software (Systat Software, Chicago, IL). Data were first tested for normality and equal variance. HRV data were not normally distributed, and data were log transformed for statistical analysis. Two-way ANOVA with Student–Newman–Keuls post hoc analysis was used to compare the effects of dummy/pacifier use on HR, blood pressure, TOI, and HRV separately in AS and QS in each sleeping position at each postnatal age. The relationship between method of feeding and dummy/pacifier use was tested with the χ2 analysis. Data are presented as mean ± SEM with significance taken at P < 0.05.
Statement of Financial Support
Funding for this study was provided by The National Health and Medical Research Council of Australia grant 1006647, The Lullaby Trust (UK), and the Victorian Government Infrastructure Support Program.
References
Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012;379:2162–72.
Blair PS, Platt MW, Smith IJ, Fleming PJ ; CESDI SUDI Research Group. Sudden infant death syndrome and sleeping position in pre-term and low birth weight infants: an opportunity for targeted intervention. Arch Dis Child 2006;91:101–6.
Blair PS, Sidebotham P, Berry PJ, Evans M, Fleming PJ. Major epidemiological changes in sudden infant death syndrome: a 20-year population-based study in the UK. Lancet 2006;367:314–9.
Trachtenberg FL, Haas EA, Kinney HC, Stanley C, Krous HF. Risk factor changes for sudden infant death syndrome after initiation of Back-to-Sleep campaign. Pediatrics 2012;129:630–8.
Moon RY, Horne RS, Hauck FR. Sudden infant death syndrome. Lancet 2007;370:1578–87.
Kinney HC, Thach BT. The sudden infant death syndrome. N Engl J Med 2009;361:795–805.
Witcombe NB, Yiallourou SR, Walker AM, Horne RS. Blood pressure and heart rate patterns during sleep are altered in preterm-born infants: implications for sudden infant death syndrome. Pediatrics 2008;122:e1242–8.
Yiallourou SR, Witcombe NB, Sands SA, Walker AM, Horne RS. The development of autonomic cardiovascular control is altered by preterm birth. Early Hum Dev 2013;89:145–52.
Horne RS. Effects of prematurity on heart rate control: implications for sudden infant death syndrome. Expert Rev Cardiovasc Ther 2006;4:335–43.
Fyfe KL, Yiallourou SR, Wong FY, Odoi A, Walker AM, Horne RS. Cerebral oxygenation in preterm infants. Pediatrics 2014;134:435–45.
Horne RS, Hauck FR, Moon RY, L’hoir MP, Blair PS ; Physiology and Epidemiology Working Groups of the International Society for the Study and Prevention of Perinatal and Infant Death. Dummy (pacifier) use and sudden infant death syndrome: potential advantages and disadvantages. J Paediatr Child Health 2014;50:170–4.
Vennemann MM, Bajanowski T, Brinkmann B, Jorch G, Sauerland C, Mitchell EA ; GeSID Study Group. Sleep environment risk factors for sudden infant death syndrome: the German Sudden Infant Death Syndrome Study. Pediatrics 2009;123:1162–70.
American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome, Moon RY. Policy statement - SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment. Pediatrics 2011;128:1030–9.
Franco P, Scaillet S, Wermenbol V, Valente F, Groswasser J, Kahn A. The influence of a pacifier on infants’ arousals from sleep. J Pediatr 2000;136:775–9.
Hanzer M, Zotter H, Sauseng W, Pfurtscheller K, Müller W, Kerbl R. Pacifier use does not alter the frequency or duration of spontaneous arousals in sleeping infants. Sleep Med 2009;10:464–70.
Howard CR, Howard FM, Lanphear B, et al. Randomized clinical trial of pacifier use and bottle-feeding or cupfeeding and their effect on breastfeeding. Pediatrics 2003;111:511–8.
Franco P, Chabanski S, Scaillet S, Groswasser J, Kahn A. Pacifier use modifies infant’s cardiac autonomic controls during sleep. Early Hum Dev 2004;77:99–108.
Yiallourou SR, Poole H, Prathivadi P, Odoi A, Wong FY, Horne RS. The effects of dummy/pacifier use on infant blood pressure and autonomic activity during sleep. Sleep Med 2014;15:1508–16.
Australian Bureau of Statistics. Socio-economic Indexes for Areas (SEIFA). Technical paper. 2011. (http://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/22CEDA8038AF7A0DCA257B3B00116E34/$File/2033.0.55.001%20seifa%202011%20technical%20paper.pdf).
Yiallourou SR, Sands SA, Walker AM, Horne RS. Maturation of heart rate and blood pressure variability during sleep in term-born infants. Sleep 2012;35:177–86.
Niemelä M, Pihakari O, Pokka T, Uhari M. Pacifier as a risk factor for acute otitis media: a randomized, controlled trial of parental counseling. Pediatrics 2000;106:483–8.
Mauch CE, Scott JA, Magarey AM, Daniels LA. Predictors of and reasons for pacifier use in first-time mothers: an observational study. BMC Pediatr 2012;12:7.
Odoi A, Andrew S, Wong FY, Yiallourou SR, Horne RS. Pacifier use does not alter sleep and spontaneous arousal patterns in healthy term-born infants. Acta Paediatr 2014;103:1244–50.
Jaafar SH, Jahanfar S, Angolkar M, Ho JJ. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev 2011;CD007202.
Malloy MH. Prematurity and sudden infant death syndrome: United States 2005-2007. J Perinatol 2013;33:470–5.
Yiallourou SR, Walker AM, Horne RS. Validation of a new noninvasive method to measure blood pressure and assess baroreflex sensitivity in preterm infants during sleep. Sleep 2006;29:1083–8.
Suzuki S, Takasaki S, Ozaki T, Kobayashi Y. Tissue oxygenation monitor using nir spatially resolved spectroscopy. Proc SPIE 1999;582–92.
Anders T, Emde RN, Parmelee AH ; University of California LABIS 1971. A Manual of Standardized Terminology, Techniques and Criteria for Scoring of States of Sleep and Wakefulness in Newborn Infants. Los Angeles, CA: UCLA Brain Information Service/BRI, 1971.
Brase CH, Brase CP. Understandable Statistics: Concepts and Methods. Melbourne, Australia: Cengage Learning, 2011.
Rosenstock EG, Cassuto Y, Zmora E. Heart rate variability in the neonate and infant: analytical methods, physiological and clinical observations. Acta Paediatr 1999;88:477–82.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996;93:1043–65.
deBoer RW, Karemaker JM, Strackee J. Hemodynamic fluctuations and baroreflex sensitivity in humans: a beat-to-beat model. Am J Physiol 1987;253:H680–9.
Acknowledgements
The authors would like to thank all the parents and their infants who participated in this study and the staff of the Melbourne Children’s Sleep Centre where the studies were carried out.
Author information
Authors and Affiliations
Corresponding author
PowerPoint slides
Rights and permissions
About this article

Cite this article
Horne, R., Fyfe, K., Odoi, A. et al. Dummy/pacifier use in preterm infants increases blood pressure and improves heart rate control. Pediatr Res 79, 325–332 (2016). https://doi.org/10.1038/pr.2015.212
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2015.212
This article is cited by
-
Autonomic development in preterm infants is associated with morbidity of prematurity
Pediatric Research (2022)
-
Cerebral cortical autonomic connectivity in low-risk term newborns
Clinical Autonomic Research (2021)
-
Autonomic nervous system development and its impact on neuropsychiatric outcome
Pediatric Research (2019)
