
Abstract
Background
Prone sleeping is used in preterm infants undergoing intensive care to improve respiratory function, but evidence suggests that this position may compromise autonomic cardiovascular control. To test this hypothesis, this study assessed the effects of the prone sleeping position on cardiovascular control in preterm infants undergoing intensive care treatment during early postnatal life.
Methods
Fifty-six preterm infants, divided into extremely preterm (gestational age (GA) 24–28 weeks, n = 23) and very preterm (GA 29–34 weeks, n = 33) groups, were studied weekly for 3 weeks in prone and supine positions, during quiet and active sleep. Heart rate (HR) and non-invasive blood pressure (BP) were recorded and autonomic measures of HR variability (HRV), BP variability (BPV), and baroreflex sensitivity (BRS) using frequency analysis in low (LF) and high (HF) bands were assessed.
Results
During the first 3 weeks, prone sleeping increased HR, reduced BRS, and increased HF BPV compared to supine. LF and HF HRV were also lower prone compared to supine in very preterm infants. Extremely preterm infants had the lowest HRV and BRS measures, and the highest HF BPV.
Conclusions
Prone sleeping dampens cardiovascular control in early postnatal life in preterm infants, having potential implications for BP regulation in infants undergoing intensive care.
Similar content being viewed by others

Introduction
The baroreflex is the primary mechanism for the short-term regulation of blood pressure (BP),1 and operates via sympathetic and parasympathetic inputs to the heart and vasculature. Cardiovascular control is immature in infants born preterm, and this immaturity is inversely related to both gestational age (GA) at birth and chronological age.2,3 Cardiovascular dysfunction, characterized by low BP, cardiac output, and systemic blood flow, frequently occurs in preterm infants.4 In the first days and weeks after birth, low BP and blood flow may increase the risk of circulatory failure and low cerebral perfusion. Limited ability to control BP and to autoregulate cerebral blood flow,5,6 is a major mechanism for ischemic or hemorrhagic injury and long-term neurodevelopmental disabilities in preterm infants.7 Conversely, hypertensive periods within the first few weeks of life can cause end-organ damage or intracerebral hemorrhage.8 Therefore, adequate BP control is vital for minimizing morbidity and mortality in preterm infants.
Prone positioning is frequently employed to improve respiratory function in preterm infants in the neonatal intensive care unit (NICU).9 However, studies in term infants after hospital discharge demonstrate that prone sleeping, the major risk factor for Sudden Infant Death Syndrome, lowers BP,10 cerebral oxygenation,11 and impairs BP control12 and cerebrovascular control.13 These position-related effects are sleep state-dependent, with the prone position being associated with the lowest values of BP and cerebral oxygenation during quiet (QS) compared to active sleep (AS).10,11 Moreover, these effects are amplified in preterm compared to term-born infants after term-equivalent age.14,15 Recently, we demonstrated that despite improved cardiorespiratory stability,16 the prone position increases cerebral oxygen extraction, particularly within the early postnatal period, in extremely preterm infants.17 Some studies in preterm infants in the NICU suggest that similar to older discharged infants, prone sleeping may dampen autonomic control.18,19,20,21 However, these studies are based on heart rate (HR) alone. Currently, the effects of prone sleeping on BP control and how this is altered by GA at birth and chronological age in preterm infants whilst in the NICU remains unknown.
The aim of this study was to investigate the effects of prone sleeping, sleep state, and GA at birth on autonomic cardiovascular control in preterm infants undergoing intensive care across the first postnatal weeks. We hypothesized, that compared to sleeping supine, prone sleeping would impair autonomic control of HR and BP and the baroreflex, and greater position-related impairments would be evident in those infants born at earlier GAs.
Methods
Ethical approval
Ethical approval was obtained from the Monash Health and Monash University human research ethics committees. The project was carried out according to the National Statement on Ethical Conduct in Human Research (NHMRC, 2007) produced by the National Health and Medical Research Council of Australia and studies conformed to the standards set by the Declaration of Helsinki (2013). Written informed parental consent was obtained.
Subjects
Preterm infants born between 24 and 34 weeks’ GA at Monash Newborn were recruited. Exclusion criteria included intrauterine growth restriction, indwelling umbilical catheters, major congenital abnormalities, or major brain pathologies. All aspects of the clinical management were at the attending physician’s discretion.
Study protocol
Infants were studied longitudinally on a weekly basis, with the first study performed at the end of the first week of life, and continued until 3 weeks after birth. Each study was 2–4 h in duration with infants randomly placed both prone and supine for sleep. In the supine position, the head was maintained in the midline and when prone, the infant’s head was turned to one side. HR from electrocardiogram leads (Covidien, USA) and respiratory rate, using Respibands (ADInstruments, Australia) were recorded. BP was measured using a small photoplethysmographic cuff (FinometerTM, Finapres Medical Systems, Netherlands) placed around the infant’s wrist as previously validated in preterm infants.22 BP data were collected in 2-min epochs, with at least 4 min between cuff inflations to prevent venous pooling in the hand. All physiological parameters (HR, respiratory rate, and BP) were recorded via a Powerlab system (ADInstruments, Australia) at a sampling rate of 400 Hz. As minimal handling of the preterm infant is vitally important in the early postnatal period, bed-side scoring using behavioral criteria was utilized to determine sleep state;23 with cardiorespiratory measures (HR and respiration) validated as strong predictors of sleep state when compared to gold-standard methods (that is EEG combined with behavioral scoring).24 Sleep state was determined using established behavioral criteria including eye, facial, body, limb movements as well as respiratory and heart rate patterns noted at least every 10–30 s at the infants cot-side. QS was characterized by the absence of eye movements, regular respiratory and HR patterns, and absence of body movements. In contrast, AS was characterized by the presence of eye movements, irregular respiration HR, and frequent gross and small body movements.23 Data were recorded and analyzed using LabChart software (ADInstruments, Australia).
Data analysis
Artifact-free epochs that were longer than 55 s and up to 2 min in duration were selected when BP was recorded.25 Using maximum threshold detection, systolic blood pressure (SBP) was calculated. Spectral analysis methods were applied to assess HR variability (HRV), and BP variability (BPV) and baroreflex sensitivity (BRS) using MATLAB (Mathworks; Natick, Massachusetts, USA) software (described below). All data were averaged for each sleep state and position in each infant, at each chronological week.
Assessment of autonomic cardiovascular control
Assessment of autonomic cardiovascular control can be achieved via spectral analysis to quantify measures of HRV, BPV, and BRS.22,26,27,28 Spectral divisions of HRV and BPV reflect the relative contributions of both the sympathetic and parasympathetic nervous system, while transfer function analysis between SBP and R–R interval changes estimates BRS.
Spectral analysis of R–R interval and SBP was performed to reflect spontaneous changes in HRV and BPV, respectively. Power spectral analysis was performed to separate R–R interval and SBP time series into low frequency (LF) and high frequency (HF) components.29 For HRV, the LF oscillations are attributed to baroreflex-mediated changes and reflect both sympathetic and parasympathetic activity.30 HF oscillations are attributed to respiratory-related changes in HR and reflect parasympathetic activity.30,31 The LF component of BPV is thought to be predominantly a marker of sympathetic vasomotor regulation.30 The HF component is influenced by the mechanical effects of respiration acting directly on intrathoracic elements of the cardiovascular system. HF BPV is also reflective of the fast baroreflex-mediated changes influenced by variations in cardiac stroke volume and R–R interval that are affected by the parasympathetic activity of BRS.30
The LF and HF ranges were defined between 0.04 and 0.15 Hz and 0.4 and 1.5 Hz, respectively.32 LF, HF, total power (TP), and LF/HF ratio (LF/HF) for each epoch was calculated from the area under the power spectral density functions in each frequency band and represent the square of the amplitude of an oscillatory signal in the frequency range.
BRS was assessed using methods described previously.15,26 Transfer function and coherence analysis were estimated to determine the gain, phase shift, and coherence of the coupling between SBP (input signal) and R–R interval (output signal) changes. Gain, phase shift, and coherence were calculated between SBP and R–R interval changes. Gain (BRS) was chosen at the frequency of maximum coherence (the frequency at which there is a maximal coupling between SBP and R–R changes), within 0.04–0.15 Hz.
Statistical analysis
Statistical analysis was performed using SPSS software v24 (IBM SPSS, USA). To compare GA, infants were grouped into those born extremely preterm (defined as <29 weeks GA) and very preterm term (defined as >29 weeks GA). Data were averaged for demographic and clinical characteristics for each GA group (extremely and very preterm groups) at each study week (chronological age—weeks 1, 2, and 3 after birth). Continuous variables were compared using Student’s t-tests and categorical data via χ2 analysis.
To compare the effects of sleep position, sleep state, chronological age, and GA, a mixed model was performed on each outcome variable (SBP, HR, and all spectral indices). Two models were used with the following fixed effects: (1) position, sleep state, chronological age, GA group, position × chronological age interaction, and (2) position, sleep state, chronological age, GA group, position × GA group interaction. The subject was entered as a random effect and position, sleep state, and chronological age were entered as repeated measures. To adjust for the potential confounder of respiratory support on cardiovascular dynamics, the type of respiratory support (supplemental oxygen (O2), high flow, continuous positive airway pressure (CPAP), intermittent positive-pressure ventilation, or no respiratory support) was entered as a covariate in each model. Multiple comparisons were adjusted using Benjamini Hochberg’s procedures.
Results
Demographics
Demographic details for the population as a whole and in the two GA groups are presented in Table 1. As per study design, GA at birth, birth weight, and postmenstrual age at each weekly study were significantly lower in the extremely preterm group. During the study period, all infants were clinically stable, and none were receiving inotropic medications. The extremely preterm group consistently had more infants who required respiratory support (including intermittent positive-pressure ventilation, continuous positive airway pressure, and high flow) at each weekly study compared to the very preterm group.
For ease of interpretation, Table 2 summarizes the significant main effects of sleeping position, sleep state, gestational and chronological age on autonomic control in preterm infants undergoing intensive care within the first three weeks of life. Overall, the prone sleeping position increased HR, reduced BRS, and increased HF BPV compared to the supine sleeping position. LF and HF HRV were also lower during prone compared to supine sleeping in very preterm infants. Extremely preterm infants had lower HRV and BRS measures, and higher HF BPV compared to very preterm infants.
Effect of sleep position
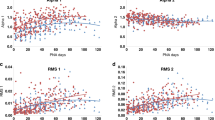
The effects of sleeping position across the first 3 weeks on HRV, BPV, and BRS indices are presented in Figs. 1, 2 and 3, respectively. Overall, autonomic cardiovascular control was altered in the prone compared to the supine position. In the prone position, R–R interval was shorter (i.e., increased HR) (main effect, P < 0.01) (Fig. 1a), and TP HRV, LF HRV, and HF HRV were all reduced (main effect, P < 0.01 for TP and HF, and P < 0.05 for LF) (Fig. 1b–d). There was no significant effect of position on LF/HF HRV (Fig. 1e). For TP, LF, and HF HRV, there was a significant interaction (position × GA group, P < 0.01 for TP and LF, and P < 0.001 for HF) (Fig. 1b–d) and post-hoc analysis identified all indices were lower in the prone compared to the supine position only in the very preterm group.

Effects of sleep position, sleep state, chronological age, gestational age (GA) group, and GA × position interaction on heart rate variability (HRV) spectral indices (a–e) recorded during the first 3 weeks of life in prone – quiet sleep (QS) (black bars), supine – QS (black hashed bars), prone – active sleep (AS) (gray bars) and supine – AS (gray hashed bars). TP total power, LF low frequency, HF high frequency. P-values represent overall significant differences for fixed effects entered into the mixed model. Where there was a significant interaction, post-hoc analysis identified all indices were lower in the prone compared to the supine position only in the very preterm group.

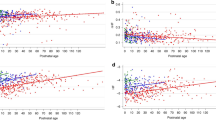
Effects of sleep position, sleep state, chronological age, gestational age (GA) group, and GA x position interaction on blood pressure variability (BPV) spectral indices (a–e) recorded during the first 3 weeks of life in prone – quiet sleep (QS) (black bars), supine – QS (black hashed bars), prone – active sleep (AS) (gray bars) and supine – AS (gray hashed bars). TP total power, LF low frequency, HF high frequency. P-values represent overall significant differences for fixed effects entered into the mixed model. Where there was a significant interaction, post-hoc analyses identified LF/HF BPV was lower in the prone compared to the supine position only in the very preterm infants.

Effects of sleep position, sleep state, chronological age, gestational age (GA) group, and GA × position interaction on baroreflex sensitivity (BRS) recorded during the first 3 weeks of life in prone – quiet sleep (QS) (black bars), supine – QS (black hashed bars), prone – active sleep (AS) (gray bars) and supine – AS (gray hashed bars). P-values represent overall significant differences for fixed effects entered into the mixed model.
For BPV, there was no effect of position on SBP, TP BPV, or LF BPV (Fig. 2a–c). HF BPV was higher (main effect P < 0.05) (Fig. 2d) and LF/HF BPV was lower in the prone compared to the supine position (main effect, P ≤ 0.05) (Fig. 2e). For LF/HF BPV, there was a significant interaction (position × GA group, P < 0.05) (Fig. 2e), and post-hoc analyses identified LF/HF BPV was lower in the prone compared to the supine position only in the very preterm infants.
BRS was lower in the prone compared to the supine position (main effect, P ≤ 0.01) (Fig. 3) and there was no significant interaction between position and GA group.
There was no significant interaction between position and chronological age in any of the parameters analyzed.
Effect of sleep state
Overall, HRV and BPV were reduced during QS compared to AS. The effects of sleep state across the first 3 weeks of life on HRV, BPV, and BRS indices are also presented in Figs. 1, 2 and 3, respectively. There was no significant effect of sleep state on R–R interval (Fig. 1a) or SBP (Fig. 2a). During QS, TP, LF, HF, and LF/HF HRV were all reduced compared to AS (main effect, P < 0.001 for TP and LF, and p < 0.01 for HF and LF/HF) (Fig. 1b–e).
BPV was also affected by sleep state, with TP, LF and HF BPV all reduced during QS when compared to AS (main effect for all P < 0.001) (Fig. 2b–d). There was no effect of sleep state on LF/HF BPV (Fig. 2e) or BRS (Fig. 3).
There were no significant interactions between position and state in any of the parameters analyzed.
Effect of gestational and chronological ages
As expected, extremely preterm infants had lower HRV and BRS compared to very preterm infants. TP, LF, and HF HRV were reduced in the extremely preterm group compared to the very preterm group (main effect, P < 0.001 for all) (Figs. 1b–d and 3). In contrast, in the extremely preterm group when compared to the very preterm group, TP and HF BPV were higher (main effect, P < 0.05 for TP, and P < 0.001 for HF) (Fig. 2b, d) and LF/HF BPV was reduced (main effect, P < 0.001) (Fig. 2e). There was no effect of the GA group on R–R interval, LF/HF HRV, SBP, or LF BPV.
Chronological age had minimal effects on autonomic control indices, with the exception of R–R interval that was shortened (i.e., increased HR) (main effect, P < 0.001) (Fig. 1a), and SBP that was increased (main effect, P < 0.01) (Fig. 2a) with increasing chronological age. Post-hoc analysis identified that R–R intervals were shorter (higher HR) at week 3 compared to weeks 1 and 2, and SBP was higher at week 3 compared with week 1. There was no effect of increasing chronological age on any of the HRV, BPV, or BRS indices.
Discussion
This is the first study to assess the effects of sleep position, while taking sleep state into account, on autonomic control of HR and BP in preterm infants during their first 3 weeks in the NICU, when the risks of cardiovascular compromise are greatest. When sleeping prone, HR was higher, BRS was lower and HF BPV was higher compared to sleeping in the supine position in both extremely and very preterm infants. In addition, in the very preterm group only, the prone position reduced HRV. As predicted, autonomic control was dependent on sleep state, with HRV and BPV being lower during QS compared to AS, confirming the predominance of parasympathetic activity in QS,33 and the importance of taking sleep state into account when evaluating autonomic control in preterm infants. Importantly, we identified no interaction between sleeping position and sleep state, or between sleeping position and chronological age, indicating that infants may be vulnerable to these position-related changes at all times during sleep and across the first three weeks of the neonatal period.
Prone positioning
Notably, the majority of studies investigating autonomic control in the prone position in the NICU have examined HR alone. A strength of our study was the ability to assess control of both HR and BP to gain a greater insight into baroreflex function. For the first time, this study showed that the prone position reduced BRS in preterm infants undergoing intensive care across the first 3 weeks of life. Furthermore, we confirmed previous studies showing that HRV is reduced and HR increased in the prone position in very preterm infants,18,20,34 suggestive of parasympathetic withdrawal. Reduced BRS during prone sleeping indicates potential impairment of BP control in this position, possibly caused by dampened HR responses (particularly in the very preterm group) to changes in BP. Interestingly, the prone sleeping position also increased HF BPV. This increase in HF BP fluctuations is likely due to larger respiratory-related swings in BP, mediated by the higher tidal volume in this position.9 We speculate that increased HF BPV in the prone position may also be a product of the dampened BRS in this position. Pagani et al., report that HF BPV is buffered by the baroreflex via the fast-acting parasympathetic inputs to the heart. Accordingly, with lower BRS in the prone position, HF BP changes may not be completely buffered by the baroreflex response, leading to larger fluctuations in BP in this position.35 In support of this speculation, we found the HF HRV (reflecting parasympathetic activity) was also reduced when prone. Taken together, and in line with our hypothesis, these results suggest the prone position is associated with dampened baroreflex functioning and HR control. This dampening of autonomic control could potentially render the preterm infant vulnerable to hypotensive and hypertensive events.36 However, further studies (e.g., a randomized controlled trial) with a larger number of infants are required to assess the impact of position-related dampened autonomic control on blood pressure fluctuations and the neonatal brain, as well as long-term neurodevelopmental outcomes to determine the clinical significance of these findings.
The mechanism/s underlying the position-related autonomic responses in preterm infants are not yet fully understood. One potential mechanism may relate to a thermoregulatory-mediated response. The prone position is associated with a decreased ability to dissipate heat,37 leading to peripheral vasodilation in order to promote heat loss. This vasodilation is thought to cause a compensatory rise in HR by the baroreflex to maintain adequate BP and organ perfusion.10,38 In our study, we did not measure skin or core body temperature, however, there was an increase in HR in the prone compared to the supine position, while SBP was maintained between positions. The changes in HRV measures in the prone position in this study are also in line with the physiological response to an increase in body temperature. Studies show that higher body temperature decreases both LF and HF HRV together with an increase in HR.19 It is believed that these changes reflect both an increase in sympathetic activity and parasympathetic withdrawal.36 In contrast to this contention, other studies have identified that skin blood flow is reduced in the prone position in preterm infants via increased systemic vascular resistance, which is thought to be a compensatory response to reduced cardiac output in the prone position as a result of increased in intrathoracic pressure in this position.39,40 The reduced cardiac output during prone sleeping could also underpin the higher HR, which serves to maintain SBP. Alternatively, reduced BRS in the prone position and with lower GA may be caused by cerebral hemodynamic mechanisms. We have previously shown that prone sleeping increased cerebral fractional oxygen extraction in extremely preterm infants in the first week of life, suggesting reduced cerebral blood flow in this position in the youngest infants.17 To confirm this, further studies investigating the relationship between autonomic activity and cerebral oxygenation in preterm infants still in NICU are required.
Gestational age
This study also found that GA at birth had an effect on position-related differences on autonomic control parameters, with prone sleeping reducing HRV and LF/HF BPV in the very preterm group only. Our findings are consistent with a number of cross-sectional studies, which also found that the prone position increases HR and reduces HRV in very preterm infants.18,20,34,36 To our knowledge, no other studies have investigated the effects of sleeping position on HRV in extremely preterm infants during the early postnatal period. Notably, in the extremely preterm group, we found very low HRV values, a finding consistent with the well-established concept that preterm birth has a significant effect on autonomic control with preterm infants born at the earliest GAs having lower HRV41,42 and lower BRS.43,44 Therefore, in extremely preterm infants, who already manifest very low values of HRV, position-related changes may not be apparent, as autonomic control may be functionally immature and/or at minimal levels, and hence cannot be altered further. As a result, it is possible that the baroreflex is limited in extremely preterm infants by their very low HRV, due to immaturity of the autonomic nervous system and its central regulation.
This immaturity of the autonomic nervous system was also reflected by BPV indices. We found TP and HF BPV were higher and LF/HF BPV was lower in the extreme compared to the very preterm group. These changes may be a consequence of the lower HF HRV and lower BRS in the extremely preterm infants. Previous studies have also identified reduced HR control in preterm infants, with a marked reduction in HF HRV in those born at the earliest GAs,3,25,45 suggesting reduced parasympathetic input. Animal studies show that the sympathetic limb of the baroreflex develops early in fetal life and decreases during postnatal maturation, whereas the parasympathetic limb develops in late gestation and increases postnatally.46,47 Therefore, extremely preterm birth, which occurs before/during important maturation of the parasympathetic branch in late gestation, may significantly impact parasympathetic cardiovascular control. In addition, the respiratory effects on BP may be more marked in extremely preterm infants who have a worse respiratory function and receive higher levels of respiratory support. Increased respiratory dysfunction, and type and level of respiratory support (e.g., mechanical ventilation) in the extremely preterm group, may lead to higher fluctuations in tidal volumes and contribute to greater HF oscillations in BP, albeit the same GA differences were observed after adjusting for type of respiratory support. Accordingly, these respiratory-induced influences on BP, together with limited BRS and diminished parasympathetic responses in BRS, HR, and cardiac output may contribute to cardiovascular instability in the extremely preterm infants.
Limitations
Our study has several limitations. The study population included infants who were clinically stable, without significant intraventricular hemorrhage, had relatively mild respiratory dysfunction as evidenced by their oxygen requirement of <40%, and no infants were receiving inotropic support. Further studies are needed to verify our findings in clinically unstable infants with hemodynamic and respiratory instability, who are most often slept in the prone position. In addition, we analyzed HR and BP epochs that were free of apneas and desaturations, as our aim was to analyze responses primarily due to the baroreflex rather than responses driven by either hypoxia and/ or respiratory events. Studies investigating the effect of these respiratory events on autonomic function may prove to be important as many preterm infants experience respiratory distress and this may have lasting effects on central and peripheral mechanisms that control HR and BP. Using a longitudinal design, we evaluated position, state, and age-related changes during the first 3 weeks of life. What remains unknown is the long-term impacts of prone positioning and the effects on neurodevelopmental and respiratory outcomes, which should be assessed in a randomized control trial setting.
Clinical implications
Prone positioning is widely used in NICUs as it improves respiratory function, however, our study showed that prone positioning dampens autonomic cardiovascular control. As a legacy of their premature birth, preterm infants have immature cardiovascular control and the risk of circulatory failure and low cerebral perfusion is high in the early postnatal weeks. Placing a preterm infant in the prone position may further amplify impairment of cardiovascular control by favoring parasympathetic withdrawal and dampening the cardio-vagal baroreflex. Reduced BRS could potentially pre-dispose an infant to hypotensive or hypertensive events, as changes in BP may not be buffered appropriately. As such, the preterm infant may experience periods of cardiovascular instability, including both low and high BP, as well as larger fluctuations in BP, which could increase the risk of hyper- and hypo-perfusion, particularly to the brain. However, we acknowledge that these findings only demonstrate dampened cardiovascular control in the prone position and the clinical significance of these position-related changes is unknown. On the other hand, the short-term respiratory benefits of prone sleeping in the NICU are well-reported and clinically relevant. Therefore, further studies are required to determine (1) whether dampened cardiovascular control in the prone position affects cerebral perfusion in clinically unstable infants (2) which and when infants are most vulnerable and (3) whether there are any adverse effects on neonatal brain structure and function. This information would provide important evidence on both the clinical advantages and disadvantages (if any) of the prone sleeping position for best practice in the NICU.
Conclusions
This is the first study to investigate position-related effects on both HR and BP control in infants born extremely and very preterm and demonstrated that the prone position increased HR, reduced BRS, and increased HF BPV across the first 3 weeks of life. Prone positioning dampened autonomic control of HR in only the very preterm infants. In addition, extremely preterm infants had immature autonomic control with reduced autonomic heart rate activity, impaired baroreflex, and larger fluctuations in BP compared to very preterm infants. These results reveal both the prone position and early GA at birth impair autonomic control in the first 3 weeks of life. Further studies are required to determine the clinical significance of impaired autonomic control in the prone position and the association with cardiovascular instability in preterm infants during the early neonatal period.
References
Andriessen, P. et al. Noninvasive assessment of blood pressure variability in preterm infants. Pediatr. Res. 55, 220–223 (2004).
Hsu, K. H. et al. Hemodynamic reference for neonates of different age and weight: a pilot study with electrical cardiometry. J. Perinatol. 36, 481–485 (2016).
Yiallourou, S. R., Witcombe, N. B., Sands, S. A., Walker, A. M. & Horne, R. S. The development of autonomic cardiovascular control is altered by preterm birth. Early Hum. Dev. 89, 145–152 (2013).
Seri, I. Management of hypotension and low systemic blood flow in the very low birth weight neonate during the first postnatal week. J. Perinatol 26(Suppl 1), S8–S13 (2006).
Wong, F. Y. et al. Impaired autoregulation in preterm infants identified by using spatially resolved spectroscopy. Pediatrics 121, e604–e611 (2008).
Wong, F. Y., Silas, R., Hew, S., Samarasinghe, T. & Walker, A. M. Cerebral oxygenation is highly sensitive to blood pressure variability in sick preterm infants. PLoS ONE 7, e43165 (2012).
Volpe, J. J. Brain injury in premature infants: a complex amalgam of destructive and developmental disturbances. Lancet Neurol. 8, 110–124 (2009).
Dionne, J. M. & Flynn, J. T. Management of severe hypertension in the newborn. Arch. Dis. Child. 102, 1176–1179 (2017).
Rivas-Fernandez, M., Roque, I. F. M., Diez-Izquierdo, A., Escribano, J. & Balaguer, A. Infant position in neonates receiving mechanical ventilation. Cochrane Database Syst. Rev. 11, CD003668 (2016).
Yiallourou, S. R., Walker, A. M. & Horne, R. S. C. Effects of sleeping position on development of infant cardiovascular control. Arch. Dis. Child. 93, 868–872 (2008).
Wong, F. Y. et al. Cerebral oxygenation is depressed during sleep in healthy term infants when they sleep prone. Pediatrics 127, E558–E565 (2011).
Yiallourou, S. R., Walker, A. M. & Horne, R. S. Prone sleeping impairs circulatory control during sleep in healthy term infants: implications for SIDS. Sleep 31, 1139–1146 (2008).
Wong, F. et al. Cerebrovascular control is altered in healthy term infants when they sleep prone. Sleep 36, 1911–1918 (2013).
Fyfe, K. L. et al. Cerebral oxygenation in preterm infants. Pediatrics 134, 435–445 (2014).
Fyfe, K. L. et al. Gestational age at birth affects maturation of baroreflex control. J. Pediatr. 166, 559–565 (2015).
Shepherd, K. L. et al. When does prone sleeping improve cardiorespiratory status in preterm infants in the NICU? Sleep 43, zsz256 (2019).
Shepherd, K. L. et al. Effects of prone sleeping on cerebral oxygenation in preterm infants. J. Pediatr. 204, 103–110 (2019).
Sahni, R. et al. Body position, sleep states, and cardiorespiratory activity in developing low birth weight infants. Early Hum. Dev. 54, 197–206 (1999).
Ammari, A. et al. Effects of body position on thermal, cardiorespiratory and metabolic activity in low birth weight infants. Early Hum. Dev. 85, 497–501 (2009).
Fifer, W. P. et al. Interactions between sleeping position and feeding on cardiorespiratory activity in preterm infants. Dev. Psychobiol. 47, 288–296 (2005).
Jean-Louis, M. et al. Power spectral analysis of heart rate in relation to sleep position. Biol. Neonate 86, 81–84 (2004).
Yiallourou, S. R., Walker, A. M. & Horne, R. S. Validation of a new noninvasive method to measure blood pressure and assess baroreflex sensitivity in preterm infants during sleep. Sleep 29, 1083–1088 (2006).
Curzi-Dascalova, L. & Mirmiran, M. Manual of Methods of Recording and Analyzing Sleep-Wakefulness States in Preterm and Full-term Infants (INSERM, Paris, 1996).
Scher, M. S. et al. Computer classification of sleep in preterm and full-term neonates at similar postconceptional term ages. Sleep 19, 18–25 (1996).
Fyfe, K. L. et al. The effect of gestational age at birth on post-term maturation of heart rate variability. Sleep 38, 1635–1644 (2015).
Yiallourou, S. R., Sands, S. A., Walker, A. M. & Horne, R. S. C. Postnatal development of baroreflex sensitivity in infancy. J. Physiol. 588, 2193–2203 (2010).
Yiallourou, S. R., Sands, S. A., Walker, A. M. & Horne, R. S. C. Baroreflex sensitivity during sleep in infants: impact of sleeping position and sleep state. Sleep 34, 725–732 (2011).
Witcombe, N. B., Yiallourou, S. R., Sands, S. A., Walker, A. M. & Horne, R. S. Preterm birth alters the maturation of baroreflex sensitivity in sleeping infants. Pediatrics 129, e89–e96 (2012).
Yiallourou, S. R. et al. Sleep: a window into autonomic control in children born preterm and growth restricted. Sleep 40, zsx048 (2017).
Pagani, M. et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circul. Res. 59, 178–193 (1986).
Malliani, A., Lombardi, F. & Pagani, M. Power spectrum analysis of heart rate variability: a tool to explore neural regulatory mechanisms. Br. Heart J. 71, 1–2 (1994).
Cohen, E. et al. Fetal-growth-restricted preterm infants display compromised autonomic cardiovascular control on the first postnatal day but not during infancy. Pediatr. Res. 82, 474–482 (2017).
Reulecke, S., Schulz, S. & Voss, A. Autonomic regulation during quiet and active sleep states in very preterm neonates. Front. Physiol. 3, 61 (2012).
Goto, K. et al. More awakenings and heart rate variability during supine sleep in preterm infants. Pediatrics 103, 603–609 (1999).
Metsala, T., Siimes, A., Antila, K. & Valimaki, I. Association of breathing movements to the variability of heart rate and blood pressure in foetal lambs. Acta Physiol. Scand. 147, 213–219 (1993).
Sahni, R. et al. Postural differences in cardiac dynamics during quiet and active sleep in low birthweight infants. Acta Paediatr. 88, 1396–1401 (1999).
Skadberg, B. T. & Markestad, T. Behaviour and physiological responses during prone and supine sleep in early infancy. Arch. Dis. Child. 76, 320–324 (1997).
Chong, A., Murphy, N. & Matthews, T. Effect of prone sleeping on circulatory control in infants. Arch. Dis. Child. 82, 253–256 (2000).
Ma, M. et al. Prone positioning decreases cardiac output and increases systemic vascular resistance in neonates. J. Perinatol. 35, 424–427 (2015).
Wu, T. W., Lien, R. I., Seri, I. & Noori, S. Changes in cardiac output and cerebral oxygenation during prone and supine sleep positioning in healthy term infants. Arch. Dis. Child Fetal Neonatal Ed. 102, F483–F489 (2017).
Golder, V., Hepponstall, M., Yiallourou, S. R., Odoi, A. & Horne, R. S. Autonomic cardiovascular control in hypotensive critically ill preterm infants is impaired during the first days of life. Early Hum. Dev. 89, 419–423 (2013).
Van Ravenswaaij-Arts, C., Hopman, J., Kollee, L., Stoelinga, G., Van & Geijn, H. Spectral analysis of heart rate variability in spontaneously breathing very preterm infants. Acta Paediatr. 83, 473–480 (1994).
Gournay, V., Drouin, E. & Roze, J. Development of baroreflex control of heart rate in preterm and full term infants. Arch. Dis. Child. Fetal Neonatal Ed. 86, F151–F154 (2002).
Mazursky, J. E., Birkett, C. L., Bedell, K. A., Ben-Haim, S. A. & Segar, J. L. Development of baroreflex influences on heart rate variability in preterm infants. Early Hum. Dev. 53, 37–52 (1998).
Andriessen, P. et al. Baroreceptor reflex sensitivity in human neonates: the effect of postmenstrual age. J. Physiol. 568(Pt 1), 333–341 (2005).
Blanco, C. E., Dawes, G. S., Hanson, M. A. & McCooke, H. B. Carotid baroreceptors in fetal and newborn sheep. Pediatr. Res. 24, 342–346 (1988).
Segar, J. L. Ontogeny of the arterial and cardiopulmonary baroreflex during fetal and postnatal life. Am. J. Physiol. 273(2 Pt 2), R457–R471 (1997).
Acknowledgements
We would like to thank all the parents and their infants who participated in the study, and the nursing staff of Monash Newborn where the studies were carried out. We especially would like to acknowledge Dr. Nadine Brew, Ph.D., Ms. Stacey Willis, Ms. Kristy Elsayed, Dr. Hannah Cooney, Dr. Brenda Thonissen, and Dr. Margy Zuluaga Fernandez for their help with data acquisition and preliminary analysis. This work was supported by the project grant funding from the National Health and Medical Research Council (NHMRC) of Australia (Project No. 1083026), The Scottish Cot Death Trust, Clive and Vera Ramaciotti Foundation, and the Victorian Government’s Operational Infrastructure Support Program; Dr. Kelsee Shepherd is supported by an Australian Government Research Training Program Scholarship; A/Prof Flora Wong is supported by NHMRC Career Development Fellowships 1084254 and 1159120. Dr. Stephanie Yiallourou is supported by the Alice Baker and Eleanor Shaw Gender Equity Fellowship.
Author information
Authors and Affiliations
Contributions
K.S. contributed to acquisition of data, data analysis, interpretation of data, and drafting of the manuscript; S.Y., F.W., and R.S.C.H. made substantial contributions to conception and design, acquisition of data and interpretation of data, and drafting of the manuscript; E.Y. made contributed to acquisition of data and A.O. contributed to the acquisition of data and analysis. All authors contributed to revising the manuscripts critically for important intellectual content, and final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
Written informed parental consent was obtained for all infants studied and approved by the Monash Health and Monash University human research ethics committees.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shepherd, K.L., Wong, F.Y., Odoi, A. et al. Prone sleeping affects cardiovascular control in preterm infants in NICU. Pediatr Res 90, 197–204 (2021). https://doi.org/10.1038/s41390-020-01254-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-01254-z
