
Abstract
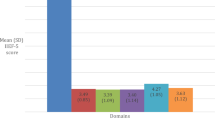
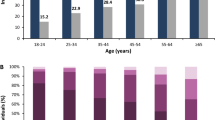
In order to assess the prevalence and associated factors for erectile dysfunction (ED) in primary care, a cross-sectional study was undertaken by questionnaire distributed to consecutive adult male attendees at 32 family practices. ED was assessed by the Korean five-item version of the International Index of Erectile Function (IIEF-5). In total, 3501 completed questionnaires were available for analysis. The prevalence of ED was severe (IIEF-5 score: 5–9) in 1.6% of cases, moderate (10–13) in 10.2%, mild (14–17) in 24.7%, and normal (18–25) in 63.4%. The prevalence of ED increased with age, lower educational status, heavy job-related physical activity, and lower income. ED prevalence was significantly higher in patients with chronic diseases such as diabetes, depression, and anxiety. These results suggest that the age-adjusted prevalence of ED among Korean men can be estimated as 32.2% (95% CI 30.6–33.7). Low socioeconomic status and several diseases such as diabetes, anxiety, and depression, as well as age, were associated with ED.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 8 print issues and online access
$259.00 per year
only $32.38 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
NIH Consensus Conference: impotence. NIH Consensus Development Panel on Impotence. JAMA 1993; 270: 83–90.
Benet AE, Melman A . The epidemiology of ED. Urol Clin North Am 1995; 22: 699–709.
Jønler M et al. The effect of age, ethnicity and geographical location on impotence and quality of life. Br J Urol 1995; 75: 651–655.
Laumann E, Paik A, Rosen RC . Sexual dysfunction in the United States: prevalence and predictors. JAMA 1999; 281: 537–544.
Melman A, Gingell JC . The epidemiology and pathophysiology of ED. J Urol 1999; 161: 511.
Read S, King M, Warson J . Sexual dysfunction in primary medical care: prevalence, characteristics and detection by general practitioner. J Public Health Med 1997; 19: 387–391.
Rosen RC et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for ED. Int J Impot Res 1999; 11: 319–326.
Ahn TY et al. Validation of an Abridged Korean Version of the International Index of Erectile Function (IIEF-5) as a Diagnostic Tool for Erectile Dysfunction. Korean J Urol 2001; 42: 535–540.
O'Leary MP et al. A brief male sexual function inventory for urology. Urology 1995; 46: 697–706.
Rosen RC et al. The International Index of Erectile Function (IIEF): a multidimensional scale for assessment of ED. Urology 1997; 49: 822–830.
Chung TG et al. The Korean Version of International Index of Erectile Function (IIEF): Reliability and Validation Study. Korean J Urol 1999; 40(10): 1334–1343.
Choi MA, Hong SS, Shin KR, Seo KO . Development of a quality of life questionnaire in erectile dysfunction patients culturally adapted to Korea. J Korean Soc 1998; 16: 175–185.
Chew KK, Earle CM, Stuckey BGA, Jamrozik K, Keogh EJ . Erectile dysfunction in general medicine practice: prevalence and clinical correlates. Int J Impot Res 2000; 12: 41–45.
Kim TH, Chung TG, Ahn TY . The relation between lower urinary tract symptoms and erectile dysfunction. J Korean Soc 1998; 16: 87–91.
Feldman HA et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994; 151: 54–61.
Marumo K, Nakashima J, Murai M . Age-related prevalence of erectile dysfunction in Japan: assessment by the International Index of Erectile Function. Int J Urol 2001; 8: 53–59.
Moreira Jr ED et al. Prevalence and correlates of erectile dysfunction: results of the Brazilian study of sexual behavior. Urology 2001; 58: 583–588.
Condra M et al. Prevalence and significance of tobacco smoking in impotence. Urology 1986; 27: 495–498.
Jeremy JY, Mikhailidis DP . Cigarette smoking and erectile dysfunction. J R Soc Health 1998; 118: 151–155.
Aytac IA et al. Socioeconomic factors and incidence of erectile dysfunction: findings of the longitudinal Massachusetts Male Aging Study. Soc Sci Med 2000; 51: 771–778.
Johannes CB et al. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol 2000; 163: 460–463.
Martin-Morales A et al. Prevalence and independent risk factors for erectile dysfunction in Spain: results of the epidemiologia de la disfuncion erectile masculina study. J Urol 2001; 166: 569–575.
Khan MA et al. Second consensus conference on cardiovascular risk factors and erectile dysfunction. Curr Med Res Opin 2002; 18: 33–35.
Rhew HY et al. The prevalence of benign prostatic hyperplasia in Busan city over age 40. Korean J Urol 2001; 42: 223–227.
Mak R, De Backer G, Kornitzer M, De Meyer JM . Prevalence and correlates of erectile dysfunction in a population-based study in Belgium. Eur Urol 2002; 41: 132–138.
Acknowledgements
This study is an add-on study of postmarketing surveillance for Sildenafil, which is supported by a grant from Pfizer Korea.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cho, B., Kim, Y., Choi, Y. et al. Prevalence and risk factors for erectile dysfuntion in primary care: results of a Korean study. Int J Impot Res 15, 323–328 (2003). https://doi.org/10.1038/sj.ijir.3901022
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijir.3901022
Keywords
This article is cited by
-
Alcohol intake and risk of erectile dysfunction: a dose–response meta-analysis of observational studies
International Journal of Impotence Research (2018)
-
Influence of socio-demographic characteristics on prevalence of erectile dysfunction in Nigeria
International Journal of Impotence Research (2013)
-
Prevalence and medical management of erectile dysfunction in Asia
Asian Journal of Andrology (2011)
-
Male sexual dysfunction in Asia
Asian Journal of Andrology (2011)
-
The effect of alcohol drinking on erectile dysfunction in Chinese men
International Journal of Impotence Research (2010)
