
Abstract
Purpose
To analyze the efficacy of modified tarsotomy for the management of severe cicatricial entropion.
Methods
Twenty-seven eyelids of 18 patients who underwent modified tarsotomy between March 2011 and July 2013 were retrospectively assessed. The data collected included patient demographics, etiology of cicatricial entropion, and surgical history. Outcome measures included surgical success rate, preoperative and postoperative eyelid position, and surgery-related complications.
Results
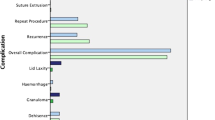
Mean follow-up time was 13.2 months (range, 6–25.4 months), and the success rate was 81.8% (22 of 27 eyelids). Complications included eyelid margin notching (n=1) and blepharoptosis secondary to avascular necrosis of the distal marginal fragment (n=1), both were corrected by minor surgical intervention.
Conclusions
The study findings suggest modified tarsotomy is effective for the correction of severe cicatricial entropion.
Similar content being viewed by others


Introduction
Entropion is inward turning of lid margin resulting in ciliocorneal contact and associated keratopathy. The causes for entropion may be congenital, involutional, or cicatricial. Cicatricial entropion is characterized by tarsoconjunctival scarring due to chronic blepharitis, ocular cicatricial pemphigoid, Stevens–Johnson syndrome, trachoma, longstanding use of topical glaucoma eyedrops, or previous surgeries.1, 2 Other signs include trichiasis, forniceal shortening and symblepharon formation. Cicatricial entropion is a challenging condition to manage and many surgical skills with variable success rates have been reported.
Treatment of cicatrical entropion requires optimizing the underlying systemic condition and surgical repair. Many surgical procedures have been reported with variable success rate, which means the definitive method does not exist. Kersten et al3 described transverse tarsotomy and lid margin rotation as a simple and reliable treatment with a success rate of 94% for mild to moderate cicatricial entropion, but a lower success rate (55%) for severe cicatricial entropion. The senior author (RCK) modified the transverse tarsotomy technique for severe cicatricial entropion, and herein, we present the method and the results of modified tarsotomy with lid margin rotation.
Subjects and methods
The case notes of all patients with cicatricial entropion that underwent modified tarsotomy and followed for at least 6 months at the Oculoplastic Service at the University of California, San Francisco between March 2011 and July 2013 were reviewed. The study was conducted in accordance with the Health Insurance Portability and Accountability Act and the guidelines issued by the Committee for Human Research. The University of California, San Francisco IRB qualified the study as exempt (IRB #13-11711). The study adhered to the tenets of the Declaration of Helsinki. This study represents consecutive patients whose eyelids met the definition of ‘severe cicatricial entropion’ at a tertiary teaching hospital, between March 2011 and July 2013. Severe cicatricial entropion patients were selected by case note review and using preoperative photographs. Severe entropion was defined as ‘gross entropion with tarsal deformity and conjunctival scarring’.1 Causative factors, operation records, postoperative complications, and follow-up ophthalmological evaluation results were reviewed. Success was defined as no eyelash–ocular surface contact and complete eyelid closure.
Surgical technique
Under monitored sedation and local anesthetic infiltration across the affected lid, a 4-0 silk traction suture was passed through the lid margin and used to evert the lid over a cotton-tipped applicator. A Supersharp eye knife was then used to incise the posterior lamella at a point 2 mm proximal to the lid margin and a full thickness tarsal incision was made with a Westcott scissors. The length of incision was about 2 mm longer than either side of the cicatrization. Two relaxing incisions were made medially and laterally at either ends of the transverse tarsal incision toward the lid margin perpendicular to the initial transverse tarsal incision. Meticulous dissection was then conducted between the distal tarsal island and orbicularis oculi muscle up to the lid margin, in order to allow full outfracture of distal tarsal fragment. Then rotational sutures with horizontal mattress 6-0 Vicryl sutures were passed through the proximal tarsus and out just above the lash line. As many everting sutures as needed were employed to secure rotation of the distal tarsus (Figures 1 and 2). If slight overcorrection could not be achieved, then the relaxing incisions were further anteriorized and edges secured with interrupted sutures.

Surgical procedure. (a) Full thickness tarsal incision is made at a point 2 mm proximal to the lid margin. The length of incision is about 2 mm longer than either side of the cicatrization. Two relaxing incisions are made medially and laterally at either ends of the transverse tarsal incision toward the lid margin perpendicular to the initial transverse tarsal incision. Meticulous dissection is then conducted between the distal tarsal island and orbicularis oculi muscle up to the lid margin, in order to allow full outfracture of distal tarsal fragment. (b and c) Horizontal mattress suture with double-armed 6-0 Vicryl suture is passed through the proximal tarsus (b) and then out to skin through orbicularis just above the lash line of the distal lid fragment (c). (d) The suture is tied just above the eyelid margin for slight overcorrection.

Schematic drawing of the procedure. (a) Full thickness transverse tarsal incision is made at a point 2 mm proximal to the lid margin. (b) Two relaxing incisions are made medially and laterally at either ends of the transverse tarsal incision toward the lid margin perpendicular to the initial transverse tarsal incision. (c) Dissection is conducted between the distal tarsal island and orbicularis oculi muscle up to the lid margin, in order to allow full outfracture of distal tarsal fragment. (d) Horizontal mattress sutures with double-armed 6-0 Vicryl suture are passed through the proximal tarsus and then out to skin through orbicularis just above the lash line of the distal lid fragment. (e) Sagittal view is shown.
In the case of severe entropion related to ocular cicatricial pemphigoid, the distal tarsal conjunctiva and eyelid margin were preserved to result in adequate outfracture and rotation.
Results
The study included 27 eyelids (15 upper and 12 lower eyelids) of 18 patients (9 men and 9 women). Mean patient age was 68.7 years (range 42–90 years). Eleven patients had entropion of one eyelid. Two patients had unilateral upper and lower eyelid entropion, three patients showed entropion of both upper eyelids, and one patient had entropion of both lower eyelids. One male patient had severe cicatricial entropion of all four eyelids.
The causes of severe cicatricial entropion were secondary to longstanding antiglaucoma drops usage in seven eyelids, chronic blepharoconjunctivitis in six, postsurgical in four (one conjunctivo-mullerectomy, one lid reconstruction after basal cell carcinoma excision, one transconjunctival lower blepharoplasty, one ectropion repair), a chemical burn in three, a thermal burn in two, Steven–Johnson syndrome in two, ocular cicatricial pemphigoid in two, and iritis associated with ankylosing spondylitis in one eyelid.
Mean follow-up time was 13.2 months (range 6–25.4 months). Average extent of tarsotomy was 65.7% (range 33–100%) of horizontal eyelid length. Procedures combined with modified tarsotomy was upper blepharoplasty in one case.
Success was defined as the absence of eyelash–ocular surface contact in all directions of gaze and complete eye closure (Figure 3). Complete correction of entropion (the absence of eyelash–ocular surface contact in all directions of gaze) was achieved for 22 (81.48%) of the 27 eyelids. Success rates by cause of entropion were as follows; 71.4% (5/7 eyelids) for secondary to antiglaucomatous topicals, 66.7% (4/6 eyelids) for chronic blepharoconjunctivitis, 100% (4/4 eyelids) for postsurgical cases, 66.7% (2/3 eyelids) for a chemical burn, 2 of 2 eyelids for a thermal burn, ocular cicatricial pemphigoid, and for Steven–Johnson syndrome, and 1 of 1 for iritis associated with ankylosing spondylitis. Five (18.52%) of the 27 eyelids, they were considered as failure, developed a residual or recurrent symptom during follow-up and all 5 eyelids had residual trichiasis; 2 were treated by wedge excision and 3 by lid splitting and anterior lamellar recession with a buccal mucous membrane graft. Two patients had complications who required surgical intervention. One patient developed medial side blepharoptosis secondary to lid margin avascular necrosis requiring ptosis repair 6 months later. The other patient showed eyelid margin notching and partial ciliocorneal touch; after wedge excision the condition did not recur. No cases of eyelid retraction, pyogenic granuloma, eyelid retraction, or overcorrection were encountered.

(a) Preoperative appearance of patient with severe cicatricial entropion and trichiasis. Lower lid retraction and tarsal deformity with conjunctival scarring of the right eyelid are shown. (b and c) Postoperative appearance at postoperative 1 week (b) and 3 months (c).
Discussion
In this study, we investigated the success rate of modified tarsotomy with lid margin rotation for severe cicatricial entropion. The most common cause of severe cicatricial entropion was secondary to longstanding antiglaucoma drops. The success rate of our technique was 81.48% with 13.2 months mean follow-up time.
Shrinkage of the posterior lamella of the eyelid, usually due to one of several conjunctival diseases, can cause cicatricial entropion. Chronic blepharoconjunctivitis, Stevens–Johnson syndrome, herpes zoster, allergies, membranous or pseudomembranous conjunctivitis, and the long-term use of certain eyedrops, such as, idoxuridine, dipivefrin hydrochloride, or antiglaucoma topicals, are the causes of cicatricial entropion in the United States, although worldwide the most common cause of cicatricial entropion is trachoma.1, 2, 4–6 In the present study, the most common causative factor for cicatricial entropion was longstanding antiglaucoma eyedrops use. This condition is called ‘pseudopemphigoid’ because light microscopy, electron microscopy, and immunofluorescence microscopy demonstrate no differences between ocular cicatricial pemphigoid and a drug-induced pemphigoid-like condition. The infiltrations of inflammatory cells, such as, fibroblasts, macrophages, and lymphocytes, into conjunctival substantia propria are observed in long-term users of antiglaucoma agents or idoxuridine.6, 7
Severe cicatricial entropion is one of the most challenging oculoplastic problems. Several surgical techniques have been introduced for its treatment but success rates vary. The choice of surgical procedure for the management of eyelid cicatricial entropion is made based on considerations of severity and extent of entropion, degree of eyelid retraction, fornix and tarsal involvement, and keratinization, eyelid margin distortion, and underlying disease progression. Surgical approaches can be broadly classified into four categories: (1) grayline splitting of anterior and posterior lamellae; (2) posterior lamella lengthening; (3) eyelid margin rotation or eversion; and (4) a combination of these three methods. Grayline splitting of anterior and posterior lamellae includes lamellar splitting with anterior lamella recession or excision, posterior lamella advancement, and anterior lamella recession with posterior lamella advancement.8, 9, 10, 11, 12 However, this technique is not suitable in the presence of metaplastic lashes in the posterior lamella. Posterior lamella lengthening requires the use of posterior and middle lamella grafts to restore a smooth surface for globe contact and therefore might take more time.13, 14, 15, 16, 17
Our technique of tarsotomy is based on the principle of eyelid margin rotation or eversion. Transverse tarsotomy and lid margin rotation is a simple procedure that effectively repositions the entropic lid margin without external incisions or grafting. Tarsotomy was first reported in 1903 by Ewing and is commonly used for trachomatous cicatricial entropion of the upper eyelid.18 Kersten RC et al3 applied the tarsotomy technique to nontrachomatous cicatricial entropion of both upper and lower eyelids, and reported a high success rate (94%) for mild to moderate cicatricial entropion, but a lower success rate (55%) for severe cicatricial entropion. On the basis of their technique, we placed a horizontal incision paralleling the lid margin posteriorly through the full thickness of conjunctiva and tarsus 2 mm proximal to the lid margin. Sharp dissection was done in the postorbicular fascial plane with a Wescott scissors to release any scarring between anterior and posterior lamellae and to allow the eyelid to assume its natural position. A double-armed 5-0 Vicryl suture was then passed through the proximal cut edge of the tarsus. Each arm of this suture was then passed distally between the orbicularis and tarsus of the distal lid margin fragment and brought out through skin just proximal to the anterior lash line. To improve the success rate of tarsotomy for severe cicatricial entropion, we introduced a simple modification involving ‘two backcuts’ at both ends of the transverse tarsotomy. These backcuts allow the distal tarsal fragment to move more freely and we believe they increase the success rate in cases of severe cicatricial entropion.
The majority of reports on the surgical success rate of cicatricial entropion did not divide patients according to severity and included all cases regardless of severity. However, success rates depend on disease severity, for example, Kersten et al3 reported a tarsotomy success rate of 94% for mild to moderate cicatricial entropion, but of only 55% for severe cicatricial entropion. Furthermore, relatively few studies have been undertaken on severe cicatricial entropion.11, 13, 14, 17 In the present study, we only included patients with severe cicatricial entropion, defined as ‘gross entropion with tarsal deformity and conjunctival scarring’ by Kemp and Collin.1 Entropion is considered mild if the tarsal plate appears grossly to be in a normal position but with conjunctivalization of the lid margin and lash/globe contact only when gaze is directed toward the involved eyelid. Entropion is considered moderate when there is more significant conjunctivalization of the lid margin approaching the base of the eyelashes and lash/globe contact is present in the primary position.1
A few studies have reported the surgical success rate for severe cicatricial entropion. Kadyan et al reported anterior lamellar excision with spontaneous granulation in seven ocular cicatricial pemphigoid patients was a simple, effective procedure, but residual lashes in three patients.10 Wu et al11 reported lamellar splitting with eyelash resection procedure’s functional success rate was 90.5% for severe, recurrent, segmental cicatricial entropion. However, this lamellar splitting technique is not suitable in the presence of metaplastic lashes in the posterior lamella. Goldberg et al reported a shared mucosal graft, based on posterior lamellar lengthening, was successful in 12 of 15 eyes (80%) with severe cicatricial entropion.14 Terminal tarsal rotation and posterior lamellar eyelid reconstruction with acellular dermis allograft for severe cicatricial entropion was successful in 14 of 16 eyelids.13 This technique is similar to our technique except it is combined with posterior lamellar lengthening with acellular dermis allograft but takes more time. Seiff et al19 reported a functional success rate of 100% for upper eyelid tarsal margin rotation and extended posterior lamellae superadvancement, which is based on a combination of eyelid margin rotation and lamellar splitting of anterior and posterior lamellae. Yagci and Palamar reported the long-term functional success of tarsal margin rotation and extended posterior lamellae advancement for upper eyelid cicatricial entropion due to end-stage trachoma was 100%.20 However, although the functional success of this technique was reported to be 100%, it is complex and introduces the possibilities of excessive hemorrhage during dissection along Muller’s muscle and fibrovascular adhesions between lamellae as Seiff et al mentioned. Furthermore, it may not be cosmetically satisfactory nor appropriate for vertically shorter lower eyelid due to possibility of tarsal buckling. Although the success rate of our modified tarsotomy is about 81%, and not 100%, it is much simpler to perform, produces cosmetically excellent results, and can be applied for both upper and lower eyelid.
Our technique’s success rate for severe cicatricial entropion was 81.48% (22 of the 27 eyelids). Five (18.52%) of the 27 eyelids, they were considered as failure, developed a residual or recurrent symptom during follow-up due to residual trichiasis. Two of them were treated by wedge excision and three were managed by lid splitting and anterior lamellar recession with a buccal mucous membrane graft.
Complications after modified tarsotomy were few. We experienced one patient that developed medial side blepharoptosis secondary to lid margin avascular necrosis requiring ptosis repair 6 months after surgery. This patient underwent upper blepharoplasty at the time of modified tarsotomy on the medial side of the upper eyelid. Furthermore, in this patient, the marginal arcade may have been sacrificed during relaxing incisions after transverse tarsal incision and the peripheral arcade may have been disrupted by blepharoplasty. Disruption of both marginal and peripheral arcades might have induced avascular necrosis and segmental blepharoptosis in the region of tarsal fracture. This case cautions that combined procedures like blepharoplasty for possible peripheral arcade disruption should be avoided. The other patient showed eyelid margin notching after modified tarsotomy and was managed by simple wedge excision.
In conclusion, the described modified tarsotomy technique is a simple procedure with a reasonable success rate for severe cicatricial entropion. We recommend this method be considered as a primary treatment option for severe cicatricial entropion due to its reliability, low morbidity, and repeatability.

References
Kemp EG, Collin JRO . Surgical management of upper lid entropion. Br J Ophthalmol 1986; 70: 575–579.
Reacher MH, Munoz B, Alghassany A, Daar AS, Elbualy M, Taylor HR . A controlled trial of surgery for trachomatous trichiasis of the upper lid. Arch Ophthalmol 1992; 110: 667–674.
Kersten RC, Kleiner FP, Dulwin DR . Tarsotomy for the treatment of cicatricial entropion with trichiasis. Arch Ophthalmol 1992; 110: 714–717.
Burnstine MA, Putterman AM, Sugar J . Cicatricial entropion caused by asymptomatic allergic conjunctivitis. Orbit 1999; 18: 211–215.
Lass JH, Thoft RA, Dohlman CH . Idoxuridine-induced conjunctival cicatrization. Arch Ophthalmol 1983; 101: 747–750.
D’Ostroph AO, Dailey RA . Cicatricial entropion associated with chronic dipivefrin application. Ophthal Plast Reconstr Surg 2001; 17: 328–331.
Patten JT, Cavanagh HD, Allansmith MR . Induced ocular pseudopemphigoid. Am J Ophthalmol. 1976; 82: 272–276.
Choi YJ, Jin HC, Choi JH, Lee MJ, Kim N, Choung HK et al. Correction of lower eyelid marginal entropion by eyelid margin splitting and anterior lamellar repositioning. Ophthal Plast Reconstr Surg 2014; 30: 51–56.
Malhotra R, Yau C, Norris JH . Outcomes of lower eyelid cicatricial entropion with grey-line split, retractor recession, lateral-horn lysis, and anterior lamella repositioning. Ophthal Plast Reconstr Surg 2012; 28: 134–139.
Kadyan A, Barry R, Murray A . Anterior lamellar excision and laissez-faire healing for aberrant lashes in ocular cicatricial pemphigoid. Eye 2010; 24: 990–993.
Wu AY, Thakker MM, Wladis EJ, Weinberg DA . Eyelash resection procedure for severe, recurrent, or segmental cicatricial entropion. Ophthal Plast Reconstr Surg 2010; 26: 112–116.
Baylis HI, Silkiss RZ . A structural oriented approach to the repair of cicatricial entropion. Ophthal Plast Reconstr Surg 1987; 3: 17–20.
Gu J, Wnag Z, Sun M, Yuan J, Chen J . Posterior lamellar eyelid reconstruction with acellular dermis allograft in severe cicatricial entropion. Ann Plast Surg 2009; 62: 268–274.
Goldberg RA, Joshi AR, McCann JD, Shorr N . Management of severe cicatricial entropion using shared mucosal grafts. Arch Ophthalmol 1999; 117: 1255–1259.
Yoon MK, McCulley TJ . Autologous dermal grafts as posterior lamellar spacers in the management of lower eyelid retraction. Ophthal Plast Reconstr Surg 2014; 30: 64–68.
Kakizaki H, Zako M, Iwaki M . Lower eyelid lengthening surgery targeting the posterior layer of the lower eyelid retractors via a transcutaneous approach. Clin Ophthalmol 2007; 1: 141–147.
Sakamoto Y, Nakajima H, Tamada I, Uchikawa Y, Kishi K . A backflip flap: a new surgical correction for severe cicatricial entropion. Plast Reconstr Surg 2010; 126: 179e–180e.
Ewing LE . An operation for atrophic(cicaricial) entropion of the lower eyelid. Am J Ophthalmol 1903; 20: 39–40.
Seiff SR, Carter SR, Tovilla y Canales JL, Choo PH . Tarsal margin rotation with posterior lamella superadvancement for the management of cicatricial entropion of the upper eyelid. Am J Ophthalmol 1999; 127: 67–71.
Yagci A, Palamar M . Long-term results of tarsal margin rotation and extended posterior lamellae advancement for end stage trachoma. Ophthal Plast Reconstr Surg 2012; 28: 11–13.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Chi, M., Kim, H., Vagefi, R. et al. Modified tarsotomy for the treatment of severe cicatricial entropion. Eye 30, 992–997 (2016). https://doi.org/10.1038/eye.2016.77
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2016.77
