
Abstract
Purpose
To ascertain the feasibility of pars plana vitrectomy (PPV) through a permanent Boston Keratoprosthesis type 1 (KPro) without the use of a temporary KPro.
Methods
A retrospective interventional case series. Eyes implanted with Boston KPro type 1 between 2008 and 2011 requiring PPV for vitreoretinal complications were included. Feasibility of PPV through the KPro, its anatomical and functional success were studied.
Results
Five out of 70 patients required PPV for vitreoretinal complications post-KPro surgery resulting in an incidence of 7%. PPV was feasible through the Boston KPro with no deleterious effects on the corneal carrier or the KPro itself. Repeat PPV was necessary in some cases. Although anatomical repair of the vitreoretinal complications was achieved in most cases, post PPV visual acuity remained poor in the majority.
Conclusion
Our study suggests that although PPV through the Boston KPro is a viable approach for vitreoretinal disease repair, visual rehabilitation remains poor.
Similar content being viewed by others

Introduction
Vitreoretinal complications after Boston Keratoprosthesis (KPro) implantation, specifically retinal detachment, may lead to severe visual loss.1 Attempts at repair pose unique surgical challenges. The standard treatment of vitreoretinal disease in patients with opaque corneas precluding adequate visualization of the fundus has been pars plana vitrectomy (PPV) through a Temporary KPro (TKPro). This technique’s short2 and long3, 4 term outcomes have shown variable degrees of success. However, data on PPV for posterior segment disease in patients with permanent Boston KPro is scarce.2, 5, 6, 7 Hence, the purpose of this study was to evaluate its feasibility and its outcomes.
Materials and methods
The research ethics committee approved this retrospective chart review. Of the 70 eyes implanted with the Boston KPro type 1 since 2008, all eyes that underwent PPV for a posterior segment complication were included. Patients’ ocular condition necessitating the implantation of the Boston KPro type 1, the vitreoretinal complication and the details of the PPV were described. Visual acuity (VA) was compared at different time points.
Surgical technique
All PPV were performed by one surgeon (MS) under local retrobulbar anesthesia. Transconjunctival oblique tunnel-like 20 gauge sclerotomies were performed as previously described.8 The standard reference point for sclerotomy placement was 3.5 mm posterior to the limbus. A 6-mm infusion cannula was inserted infero-temporally at the pars plana. The two other ports were placed supero-nasally and supero-temporally. PPV was then performed with visualization through the optical cylinder of the KPro front plate. The binocular indirect ophthalmomicroscope (BIOM) provided an anatomical field of view beyond the equator and improved vision through the small aperture of the KPro. Scleral depression was used as needed to improve visualization. Depending on the retinal pathology, PPV was supplemented with scleral buckling, PVR membrane removal, and silicone oil injection. Sclerotomies were not sutured unless leakage was observed, or silicone oil tamponnade was used.
Results
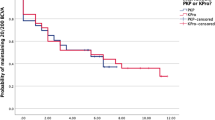
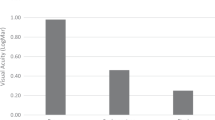
The mean age of the 70 patients implanted with Boston KPro type 1 was 59 years with 59% male. Indications for surgery were aniridia and failed grafts in 69%, infectious keratitis in 19%, chemical burn in 7%, and autoimmune disease in 5% of patients. Five eyes (7% incidence) developed posterior segment complication requiring PPV at a mean of 7.6 months post-KPro. Follow-up post-PPV was on average 13.4 months with no patient lost to follow-up. Although anatomical success was achieved in 80%, unfortunately there was limited gain in vision. Only 40% of patients had an improvement of VA albeit less than post-KPro gain, and the others had a marked drop of VA. (Table 1).
Discussion
Literature on the feasibility of PPV through a previously implanted Boston KPro is rare. The first study treating posterior segment complications without the use of TKPro showed promising outcomes.3 Our study shows that performing PPV through the Boston KPro does not cause deleterious effects on the corneal carrier or the KPro itself. It may be useful as it allows patients to benefit from a PPV without having to undergo Boston KPro removal, TKPro implantation, and then re-implantation of the Boston KPro. This shortens operative time, decreases the complexity of the surgery, and prevents further complications.
Of note, the Boston KPro tolerates fluid–gas exchange well without excessive fogging. The use of the BIOM allowed a large visual field extending to the equator. The non-contact aspect of the BIOM made surgery easier for KPro eyes that have irregular surfaces. It also permitted very delicate manipulations such as membrane dissection and delamination. Contact lenses for peeling procedures were not used nor were they required. Although 20 gauge Vitrectomy was used as per the technique already described,8 it is both transconjunctival and sutureless and therefore comparable to 25 gauge techniques. In addition, a sclera buckle was used only in those cases where it was felt to be essential to retinal reattachment. In no case was a previous glaucoma surgery compromised by buckling surgery.
Our patients suffered severe vitreoretinal disease needing multiple PPV in the majority of cases. The retina remained attached in 80%, however, the VA gained was poor and did not reach the level gained post-KPro.
This study adds to the current literature on the treatment of vitreoretinal complications post-KPro and suggests that PPV through the Boston KPro is a reasonable treatment option. Ideally, a prospective randomized controlled trial with a larger sample, evaluating long-term effects is desirable to further substantiate the benefits of this surgery. Further studies are needed to determine whether the use of smaller gauge instrumentation offer advantages over our 20 gauge technique.

References
Ray S, Khan BF, Dohlman CH, D’Amico DJ . Management of vitreoretinal complications in eyes with permanent keratoprosthesis. Arch Ophthalmol 2002; 120: 559–566.
Garcia-Valenzuela E, Blair NP, Shapiro MJ, Gieser JP, Resnick KI, Solomon MJ et al. Outcome of vitreoretinal surgery and penetrating keratoplasty using temporary keratoprosthesis. Retina 1999; 19 (5): 424–429.
Dong X, Wang W, Xie L, Chiu AM . Long-term outcome of combined penetrating keratoplasty and vitreoretinal surgery using temporary keratoprosthesis. Eye 2006; 20 (1): 59–63.
Khouri AS, Vaccaro A, Zarbin MA, Chu DS . Clinical results with the use of a temporary keratoprosthesis in combined penetrating keratoplasty and vitreoretinal surgery. Eur J Ophthalmol 2010; 20 (5): 885–891.
Chan CC, Holland EJ, Sawyer WI, Neff KD, Petersen MR, Riemann CD . Boston type 1 keratoprosthesis combined with silicone oil for treatment of hypotony in prephthisical eyes. Cornea 2011; 30 (10): 1105–1109.
Utine CA, Gehlbach PL, Zimmer-Galler I, Akpek EK . Permanent keratoprosthesis combined with pars plana vitrectomy and silicone oil injection for visual rehabilitation of chronic hypotony and corneal opacity. Cornea 2010; 29 (12): 1401–1405.
Georgalas I, Kanelopoulos AJ, Petrou P, Ladas I, Gotzaridis E . Presumed endophthalmitis following Boston keratoprosthesis treated with 25 gauge vitrectomy: a report of three cases. Graefes Arch Clin Exp Ophthalmol 2010; 248 (3): 447–450.
Stanescu-Segall D, Sebag M, Jackson T, Elagouz M . Modified 20-gauge transconjunctival pars plana vitrectomy. Retina 2011; 31 (5): 982–987.
Acknowledgements
This study was supported by the ‘Fonds de la Recherche en Ophtalmologie de l’Université de Montréal’ (FROUM).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Harissi-Dagher, M., Durr, G., Biernacki, K. et al. Pars plana vitrectomy through the Boston Keratoprosthesis type 1. Eye 27, 767–769 (2013). https://doi.org/10.1038/eye.2013.58
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2013.58
