
Abstract
Data sources
The Cochrane Central Register of Controlled Trials (CENTRAL) and Medline (PubMed) together with handsearching of a range of relevant journals.
Study selection
Studies were screened by two authors and randomised clinical trials, prospective and retrospective cohort studies with a mean follow-up of at least three years were included. Articles published in English or German were considered.
Data extraction and synthesis
Information on the survival rates of the implants and of the implant-supported reconstructions as well as on the biological and technical complications was extracted and a qualitative synthesis conducted.
Results
Twelve studies were included of which six were randomised controlled trials. After three years there was no difference in implant survival rates between splinted and unsplinted design. Most of the included studies noted that the unsplinted design needs more prosthetic maintenance. No significant difference in the peri-implant outcome between splinted and unsplinted design was found. In more of the studies that considered patient satisfaction, no significant difference in the preference of the patients was reported.
Conclusions
Within the limits of this systematic review, it is concluded that there was no significant difference between the two different designs of implant-supported overdentures with respect to the soft tissue health status or patient satisfaction, although the bar-supported overdentures have been shown to need less prosthetic maintenance.
Similar content being viewed by others


Commentary
This is more than a traditional review, in the sense that the authors have tried to employ and document systematic methods. Therefore, this can be considered a very good literature review, rather than being a systematic review, because of methodological flaws and possible sources of bias that will be delineated below.
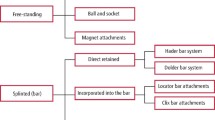
To start with, the aim of the review was clearly stated: to examine differences between splinted and unsplinted implants for implant-supported overdentures regarding 1) survival rates, 2) prosthetic / technical complications, 3) peri-implant parameters / biological complications and 4) patient satisfaction. So the reader will not have any difficulty understanding what the review was trying to achieve.
The literature search, however, was limited to two databases and two languages, potentially leading to publication and language biases, and missing the possibility of finding more studies that could have been of equal, or even better, quality and relevance than those included in this review. A manual search of a long list of journals and the reference lists of the included studies was also done.
The inclusion and exclusion criteria were eloquently stated. Nonetheless, the characteristics of eligible patients were not defined, leaving out information that may have its effect on the outcome. Another issue with the inclusion criteria was the type of the included studies where both randomised controlled trials and cohort studies (prospective and retrospective) were considered for inclusion. This is rather odd. Systematic reviews usually concentrate on one type of study design so that comparison and analysis is possible.
To their credit, the two authors independently reviewed the included studies to assess their conformity with the inclusion criteria. In the discussion, however, it was stated that ‘instead of performing a formal quality assessment of the included studies and sensitivity analysis, this review used stringent inclusion criteria.' So, validity (quality) assessment of the included studies, which is a very essential step in any systematic review, was not performed, as if it is up to us to change the way systematic reviews should be conducted. In reality, validity assessment is one of the main areas that differentiates a systematic review from a narrative review. Therefore, I respectfully disagree with authors that using 'stringent' criteria will suffice.
Taking the above issues into consideration, I conclude with two major points: 1) the findings of the review are still important; the design with which the implants are related to each other (splinted or unsplinted) does not significantly affect either the implants' survival rate or the peri-implant outcome. However, the unsplinted design needs more prosthetic maintenance. With respect to satisfaction, patients with the bar-clip are significantly more satisfied than patients with the other designs. Finally, although comparing maxillary and mandibular implant-supported overdentures was not one of the aims of the study, it is worth mentioning that only one fourth of the included studies had maxillary overdentures. So, inferring that the findings are as applicable to maxillary dentures as they are to mandibular dentures might be a point of question. 2) The quality of evidence presented by this review is considered of a low level and that is mainly due to the way the review was conducted. Had it been conducted using the proper methodology of systematic reviews, it may have resulted in a study with a better quality and, hence, potentially higher level of evidence.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Christos Stoumpis, Konitsis 12A, 15125 Maroussi, Athens, Greece. E-mail: christos.stoumpis@gmail.com
Stoumpis C, Kohal RJ. To splint or not to splint oral implants in the implant-supported overdenture therapy? A systematic literature review. J Oral Rehabil 2011; 38: 857–869.
Rights and permissions
About this article
Cite this article
Al-Ansari, A. No difference between splinted and unsplinted implants to support overdentures. Evid Based Dent 13, 54–55 (2012). https://doi.org/10.1038/sj.ebd.6400863
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400863
