
Key Points
-
Ameloblastoma presenting in a patient with Gardner's Syndrome, not previously reported.
-
Importance of early diagnosis, treatment and histological examination as it can mimic dentigerous cysts.
-
Treatment by enucleation and curettage and not more radical excision with margin of bone.
Abstract
An unusual case of a unicystic Ameloblastoma mimicking a dentigerous cyst in a 14-year-old patient with Gardner's Syndrome is described. Gardner's Syndrome is associated with multiple tumours and dental anomalies.
Similar content being viewed by others

Introduction
A 14 year old patient with Gardner's Syndrome presented with an ameloblastoma mimicking a dentigerous cyst. Gardner's Syndrome has well established associations with tumours of the bowel, skin and central nervous system with numerous dental anomalies such as multiple osteomas, compound odontomes and unerupted teeth.1,2 However Ameloblastoma has not previously been reported with this condition.
Case report
A 14-year-old male Caucasian patient was referred to the Norfolk and Norwich University Hospital with a two week history of a slowly enlarging swelling on the right side of the mandible. The patient had a complicated medical history, suffering from Gardner's Syndrome, hypopituitism and had previously undergone surgery and cranio-spinal radiotherapy for a medulloblastoma. The drug regime included thyroxin and growth hormone.
On extraoral examination there was no facial asymmetry or lymphadenopathy. Intraoral examination revealed a right sided unilateral soft swelling, extending from the first permanent molar to the permanent canine. There was considerable bucco-lingual expansion of the bone.
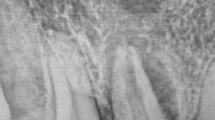
An OPT radiograph showed a large radiolucency centred on the unerupted lower right second permanent premolar extending close to the erupting lower right permanent first premolar and first permanent molar. There was erosion of the mesial root of the lower right first molar. (Fig. 1)

OPT showing large radiolucency centred on lower right premolar
A lower occlusal radiograph was also taken to assess the bucco-lingual expansion. The lower border of the mandible and lingual cortex appeared to be intact. (Fig. 2)

Lower occlusal showing lingual expansion
A provisional diagnosis of a dentigerous cyst was made. Under endotracheal general anaesthesia, the deciduous first molar along with the permanent first and second premolars and first molar were extracted as they were intimately involved with the lesion. The cystic lesion was enucleated and dissected off the buccal mucosa, the bony cavity was then curetted thoroughly. The specimen measuring 4 cm by 2.4 cm was sent to histopathology for definitive diagnosis.
Histopathology reported a plexiform ameloblastoma, which appeared to arise in a dentigerous cyst. There was no evidence of invasion of the surrounding tissues and it appeared to be contained within the cystic lining.
Follow up and review
The patient has been followed up clinically and radiographically at six monthly intervals for a year and a half. There have been no signs of recurrence and bony infill can be seen on the follow up radiograph taken one year postoperatively. (Fig. 3)

OPT showing good bony infill one year post operatively
Discussion
Gardner's Syndrome is a genetic condition demonstrating an autosomal dominant trait and is characterised by multiple lesions affecting skin, bone and the colon, with an incidence of 1: 8000. The skin lesions can be one or a combination of fibromas, desmoid tumours, epidermoid cysts or lipomas.
Multiple osteomas appear in adolescence and mainly involve the jaws, facial skeleton and frontal bone but can involve any bone. Compound odontomes and dental anomalies such as multiple unerupted teeth and osteomas may also be found in the jaws.1,2
Multiple polyps of the colon and rectum invariably become malignant and colonic resection is usually required. Desmoid tumours also arise in the abdominal wall scar. Thyroid, adrenal and biliary carcinomas along with Medulloblastoma, a common benign intra-cranial tumour3 are all associated with the syndrome. Ameloblastomas however, have not been reported as an associated tumour with Gardner's Syndrome.4
Dentigerous cysts arise from the follicle of an unerupted tooth and are regarded as cystic if the follicular space exceeds 3 mm, however diagnosis can only be made histologically.5
In addition to their potential for attaining large size, dentigerous cysts are noteworthy for their tendency to resorb the roots of adjacent teeth, and for the occasional development of neoplastic change such as plexiform ameloblastoma or carcinoma within an isolated segment of the cyst wall.4,6
The distinction between an area of proliferating odontogenic epithelium in the wall of a dentigerous cyst and early ameloblastoma may be difficult to make, and studies of lectins and other cell markers on proliferating epithelial cells have to date failed to identify those lesions most likely to develop into an ameloblastoma.4
Aetiology
Ameloblastomas are reported to arise in the second and third decades of life. Eighty percent of ameloblastomas present in the mandible of which 70 percent occur in the posterior molar region.7,8,9 These lesions can be locally aggressive if left untreated and thus early diagnosis is vital to minimise the extent of surgery
Aetiology is uncertain; it has however been suggested that they may arise in dentigerous cysts, within remnants of the dental lamina or the basal layer of the oral mucosal epithelium.10,11
Suggested predisposing factors have included irritation in the form of extractions, caries, trauma, infection, tooth eruption, nutritional deficits and viral infection especially Human Papilloma Virus (HPV).10,11
Radiation produces both stochastic and non-stochastic effects. The genetic stochastic effects have not been previously reported with ameloblastoma.
The Unicystic Ameloblastoma has been described as a variant of ameloblastoma as it displays a less aggressive course of progression and a lower rate of recurrence after treatment.10,12
Treatment of ameloblastoma
It has been suggested that the treatment of ameloblastoma in general should incorporate excision of the lesion with a margin of sound tissue. However since Unicystic Ameloblastoma seems less aggressive and has a lower incidence of recurrence12 it can be treated more conservatively by enucleation and curettage followed by regular clinical and radiological review. Regular follow up of these tumours is essential since they have the potential to recur and become large and destructive.13 Marsupulisation of such lesions is not recommended because of the potential for recurrence and the destructive nature of the lesion if left untreated. However the general consensus of opinion is that the Unicystic Ameloblastoma may be managed conservatively with regular long term follow up.
The relationship of Ameloblastoma with Gardner's Syndrome is not established. The syndrome is associated with numerous tumours and dental anomalies. Ameloblastomas occurring within the jaws have not been reported previously. This may be a coincidental finding or a new tumour related with the condition.
References
Scully C, Cawson R A . Medical problems in dentistry. 3rd ed. pp 527–528. London: Wright, 1993.
O'Reilly M, O'Reilly P, Todd CE, Altman K, Schafler K . An assessment of the aggressive potential of radiolucencies related to the mandibular molar teeth. Clinical Radiology 2000; 55: 292–295.
Leblanc R . Familial adenomatous polyposis and benign intracranial tumors: a new variant of Gardner's syndrome. Can J Neurol Sci 2000; 27: 341–346.
Lynch MA, Brightman VJ, Greenberg MS . Burkets oral medicine diagnosis and treatment. 9th ed. pp 156, 163, 171–174. USA: J. B. Lippincott Company, 1994.
Whaites E . Essentials of dental radiography and radiology. 2nd ed. pp 284. UK: Churchill Livingstone, 1996.
Gulbranson SH, Wolfey JD, Raines JM, McNally BP . Squamous cell carcinoma arising in a dentigerous cyst in a 16-month-old girl. Otolaryngol Head Neck Surg 2002; 127: 463–464.
Welbury R . Paediatric dentistry. pp 331. Oxford: University Press, 1997.
Cawson RA, O'Dell EW . Essentials of oral pathology and oral medicine. 6th ed. pp 117. UK: Churchill Livingstone, 1998.
Sousa FB, Etges A, Correa L, Mesquita RA, de Araujo NS . Pediatric oral lesions: a 15-year review from Sao Paulo, Brazil. J Clin Pediatr Dent 2002; 26: 413–418.
Kahn MA . Ameloblastoma in young persons: a clinicopathologic analysis and etiologic investigation. Oral Surg Oral Med Oral Path 1989; 67: 705–715.
Shear M, Singh S . Age-standardized incidence rates of Ameloblastoma and dentigerous cyst on the Witwatersrand, South Africa. Community Dent Oral Epidemiol 1978; 6: 195–199.
Tanaka N, Murata A, Yamaguchi A, Kohama G . Clinical features and management of oral and maxillofacial tumors in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88: 11–5(7).
Rosentein T, Pogrel MA, Smith RA, Regezi JA . Cystic Ameloblastoma—behavior and treatment of 21 cases. J Oral Maxillofac Surg 2001; 59: 1311–1316; discussion 1316–8(8).
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Patel, H., Rees, R. Unicystic Ameloblastoma presenting in Gardner's Syndrome: A case report. Br Dent J 198, 747–748 (2005). https://doi.org/10.1038/sj.bdj.4812413
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4812413
This article is cited by
-
Conservative Management of Unicystic Ameloblastoma in Young Patients: A Prospective Single-Center Trial and Review of Literature
Journal of Maxillofacial and Oral Surgery (2017)
-
Orthokeratinized Odontogenic Cyst with an Associated Keratocystic Odontogenic Tumor Component and Ghost Cell Keratinization and Calcifications in a Patient with Gardner Syndrome
Head and Neck Pathology (2017)
