
Abstract
Hyperhomocystemia has been reported to be associated with cardiovascular disease, especially stroke. The resistive index (RI) estimated by carotid ultrasound is an established variable for estimating the risk of cerebral infarction. The aim of this study was to evaluate the relationship between homocysteine concentration and carotid RI, a marker of cerebral vascular resistance in essential hypertensive patients. We measured serum total homocysteine and carotid RI in 261 patients. Multiple linear regression analysis was used to determine the association of homocysteine with carotid RI and intima media thickness (IMT). Age, sex, BMI, systolic blood pressure (SBP), homocysteine, total cholesterol, high density lipoprotein-cholesterol (HDL-C), uric acid, CRP, HbA1c, estimated glomerular filtration rate and use of antihypertensive agents were included as independent variables. Age, sex, use of antihypertensive agents, HDL-C and homocysteine levels were shown to be significant predictors of carotid RI, but not IMT. Multiple regression analysis in men older than 65 years showed homocysteine and SBP were associated significantly with carotid RI. In elderly male patients, homocysteine was the strongest predictor of carotid RI (B = 0.0068, CI = 0.0017–0.0120, P = 0.011) in the multivariate model. In conclusion, hyperhomocysteinemia is associated with carotid RI, a surrogate marker of cerebral vascular resistance, especially in elderly men.
Similar content being viewed by others


Introduction
Homocysteine is a naturally-occurring amino acid produced from a methyl donor, methionine and essential for intracellular metabolism1. Several epidemiological studies have shown that high levels of total homocysteine are associated with an increased risk of atherosclerotic disease2,3,4,5,6. However, the association between homocysteine and atherosclerosis has not been observed consistently7,8,9 and the mechanisms by which hyperhomocysteinemia increases cardiovascular risk in humans remains controversial10,11. Furthermore most clinical trials to lower homocysteine levels using folic acid or multivitamin treatment have failed to reduce cardiovascular events12,13,14.
Ultrasound of the carotid artery measures structural, functional and hemodynamic alterations and is used widely as a marker of atherosclerosis15,16. Prospective population-based studies in Europe and United States have reported that carotid intima media thickness (IMT) measured by ultrasound is associated positively with subsequent occurrence of stroke17,18. The resistive index (RI) calculated using carotid artery Doppler ultrasound is an established variable for estimating the risk of cerebral infarction as it reflects downstream arterial resistance19. We reported previously that changes in carotid hemodynamics of patients with essential hypertension were associated with asymptomatic white and gray matter lesions visualized on magnetic resonance imaging20 A recent study showed that homocysteine levels were also associated with aortic stiffness in elderly subjects, with this relationship being particularly strong in very elderly subjects21. Lim et al. reported an association between homocysteine and pulsatility index which has been used as an index of vascular resistance in the intracranial artery of patients with ischemic stroke22. To date, the relationship between serum homocysteine levels and vascular resistance in hypertensive patients remains unclear. This study evaluated the association between homocysteine concentration and cerebral vascular resistance estimated by carotid RI and IMT in patients with essential hypertension, with a special focus on elderly men.
Methods
Study population
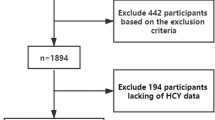
The study was a single-center, cross-sectional study of 261 consecutive patients with essential hypertension who attended an outpatient clinic at Ehime University Hospital. Hypertension was defined as a systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg, measured three times in the sitting position using a brachial sphygmomanometer, or taking an antihypertensive drug. Patients with a previous history of symptomatic cardiovascular disease, myocardial infarction, valvular heart disease, symptomatic cerebrovascular events, thyroid disease, glomerulonephritis, estimated glomerular filtration rate (eGFR) < 30 ml/min/1.73 m2, renovascular hypertension, or abnormalities in kidney structure were excluded from the study. Elderly was defined as aged ≥ 65 years and young as aged < 64 years. Increasing age and male sex are known strong determinants of serum homocysteine levels23 with elderly patients assumed to have a higher risk for asymptomatic, clinically significant, stenosis of carotid bifurcation. Accordingly, these patients are recommended to have imaging of the carotid bifurcation24. We therefore focused on elderly men in our study.
The study was approved by the ethical committee of Ehime University Hospital, with informed consent being obtained from each patient prior to enrolment. All experiments were performed in accordance with relevant guidelines and regulations.
Blood and urine sampling and laboratory measurements
A fasting blood sample was taken from the brachial vein after the patient had rested in the supine position for 30 min. Serum creatinine, total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C) uric acid and C-reactive protein (CRP) were measured using automatic enzyme immunoassays. Glycated hemoglobin (HbA1c) was analyzed by high-performance liquid chromatography (HPLC) on an Adams -A1c HA-8160 (Arkray Inc., Kyoto, Japan). Serum total homocysteine was measured using HPLC and was carried out by SRL Inc. (Tokyo, Japan). Estimated glomerular filtration rate (eGFR) was calculated using the Japanese equation for eGFR: 194 × Cr∧-1.094 × age∧-0.287 (×0.739 (female))25. Urinary albumin and Cr concentration were determined using an automated analyzer (Architect c8000; Toshiba, Inc) and the albumin to Cr ratio (uAlb/Cr) calculated to evaluate urinary albumin excretion.
Ultrasound evaluation
Ultrasound evaluation of the CCA was performed as described previously26 using an alpha-7 (Aloka Co., Tokyo Japan) that incorporated a 7.5-MHz probe equipped with a Doppler system. After the subjects had rested in the supine position for at least 10 min with their neck in a slightly hyperextended position, optimal visualization of the right CCA was performed. The IMT of the far wall was measured in the CCA at two sites, 1 and 2 cm proximal to the bulb from the anterior, lateral and posterior approaches. The mean IMT of the measurements was then calculated. Doppler evaluation was performed by scanning the right CCA in the anterior projection, with the sample volume at the center of the vessel determined using color-flow mapping. The carotid RI was calculated using the following formula: max velocity-minimum velocity/max velocity27. Two physicians carried out the ultrasound evaluation. The inter-observer coefficient of variation (CV) for mean IMT was 7.7% and intra-observer CV 6.2%. For the RI, inter-observer CV was 9.7% and intra-observer CV 5.5%.
Statistical analysis
All the analyses were performed using SPSS 18.0 (SPSS, Inc., IL, USA). All the data were expressed as mean ± standard deviation (SD), with the exception of CRP and uAlb/Cr which were expressed as median value and interquartile ranges (25% and 75% percentiles). Comparison of the clinical characteristics between the total study group and men aged ≥ 65 years was performed using unpaired t tests. The Mann-Whitney U test was used to compare CRP and uAlb/Cr in the two groups, while the χ2 test was used to analyze the distribution of drug use. The effect of independent parameters on carotid RI and mean IMT was examined by multivariate linear regression analysis, with age, sex, body mass index (BMI), SBP, serum levels of homocysteine, total cholesterol, HDL-C, uric acid, CRP and HbA1c, eGFR and use of antihypertensive agents included as the independent variables. M multiple regression analysis was also performed on men aged ≥ 65 years using the same independent variables, except for age and sex. Values of p < 0.05 were considered statistically significant.
Results
Patient characteristics
The clinical characteristics of the patients are summarized in Table 1. DBP, pulse rate, total cholesterol and eGFR were lower in men aged ≥ 65 years compared with the total group, whereas uric acid level, IMT and carotid RI were higher. The use of antihypertensive drugs, statins and antiplatelet drugs was similar in the two groups.
Association between clinical factors and carotid RI
A multivariable regression model of the carotid RI in the total study group showed that age, sex, serum levels of HDL-C, use of antihypertensive agents and homocysteine were associated significantly with carotid RI, whereas BMI, SBP, total cholesterol, HbA1c, eGFR, uric acid and CRP were not (Table 2). In the analysis of men aged ≥ 65 years, carotid RI was shown to be associated significantly with homocysteine and SBP, but not with BMI, total cholesterol, HDL-C, HbA1c, eGFR, uric acid, CRP or use of antihypertensive agents (Table 3). In elderly male patients, homocysteine was the strongest predictor of carotid RI in the multivariate model (B = 0.0068, 95% confidence interval = 0.0017–0.0120, P = 0.011).
Association between clinical factors and mean IMT
In contrast to the above results, multivariate regression analysis of the total study group showed age, serum levels of HDL-C were independent significant variables of mean IMT, whereas sex, BMI, SBP, total cholesterol, HbA1c, eGFR, uric acid, CRP, homocysteine and use of antihypertensive agents were not (Table 4). In elderly male patients, no variable reached statistical significance (Table 5).
Discussion
This study used carotid RI as a surrogate marker of cerebral peripheral artery resistance and showed that the index was associated significantly with homocysteine levels in patients with essential hypertension, especially elderly male patients.
A high RI is associated with a large difference in velocity between the systolic and diastolic phases detected by pulse-wave Doppler ultrasound19. This difference in flow velocities reflects downstream resistance, which could, in part, depend on the degree of stiffness of the peripheral arteries. Staub et al. reported the carotid RI was a predictor of cardiovascular mortality and morbidity, at least comparable to the well-established IMT19. We also demonstrated an association between carotid hemodynamics such as diastolic perfusion rate and asymptomatic white and gray matter lesions in patients with essential hypertension20. Taken together, these reports suggest that carotid hemodynamic indices such as RI and diastolic perfusion rate are markers of cerebrovascular stiffness. The data of the present study also showed that carotid RI is associated independently with age, sex, HDL-C, use of anti-hypertensive medication and homocysteine levels. This finding suggests that hyperhomocysteinemia is a risk factor for cerebrovascular stiffness.
Interestingly, the factors associated significantly with mean IMT were age and HDL-C, but not serum homocysteine levels. We reported previously that carotid RI was associated with increased serum levels of IL-6 and CRP in hypertensive patients, whereas mean IMT was not. We also reported that treatment of hypertensive patients with an angiotensin II receptor blocker for 24 months improved carotid hemodynamics and diastolic perfusion rate, but not mean IMT28. Taken together, these findings indicate the carotid RI is a useful marker of arterial stiffness, while mean IMT is a useful marker of atherosclerosis.
In other words, carotid RI and arterial stiffness may be influenced and altered by inflammation (IL-6 and CRP), oxidative stress (homocysteine29) and medications. In our study, HDL-C showed an independent, negative association with mean IMT but a positive association with carotid RI. The reason for this difference could not be determined, but may have been due to the different nature of the two parameters, one being hemodynamic and the other a result of structural alterations.
An association between hyperhomocysteinemia and atherosclerotic disease was first suggested more than 40 years ago30. Subsequently, numerous cross-sectional and case control studies have demonstrated a clear association between total serum homocysteine and the presence of coronary, carotid and peripheral vascular disease2,3,4,5,6. However, a systemic review of 12 randomized controlled trials involving 47,429 participants showed that homocysteine-lowering interventions compared with placebo did not significantly affect non-fatal or fatal myocardial infarction, stroke or death by any cause31,32,33. Clinical benefit of homocysteine lowering therapy is very controversial topics. One possible reason why these therapies were ineffective for preventing cardiovascular diseases is thought to be related to confounding factors such as anti-hypertensive drugs, statins and antiplatelet drugs34. In the homocysteine-lowering trials, anti-hypertensive drugs, statins and antiplatelet drugs were used by 30–70%, 60–80% and 80–90% of participants, respectively. Another possible reason why homocysteine-lowering multivitamin therapy appears to be ineffective for preventing cardiovascular diseases may be related to the age of study participants. The present study showed that serum homocysteine levels in elderly male patients showed a marked and highly significant association with carotid RI. This suggests that high serum homocysteine may be a marker of an increase in RI in these elderly patients, who are at an even greater risk of stroke. However, to date there have been no randomized clinical trials on homocysteine-lowering therapy in patients older than 65 years. Further randomized clinical trials are therefore needed to evaluate the effect of homocysteine –lowering therapy on cardiovascular disease in elderly hypertensive patients.
The present study had several limitations including a relatively small study population. In addition, because of its cross-sectional design we could not determine the mechanism for the relationship we observed between homocysteine and carotid RI, especially in elderly male patients with hypertension.
In conclusion, this study shows that serum homocysteine level in elderly male patients with essential hypertension is a strong predictor of carotid RI, a surrogate marker of cerebral peripheral artery resistance.
References
Mudd, S. H. et al. Homocysteine and its disulfide derivatives: A suggested consensus terminology. Arterioscler Thromb Vasc Biol. 20, 1704–1706 (2002).
Nyfard, O. et al. Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med. 337, 230–236 (1997).
Soinio, M. et al. Elevated plasma homocysteine level is an independent predictor of coronary heart disease events in patients with type 2 diabetes mellitus. Ann Intern Med. 140, 94–100 (2004).
Cheng, S. W., Ting, A. C. & Wong, J. Fasting total plasma homocysteine and atherosclerotic peripheral vascular disease. Ann Vasc Surg. 11, 217–223 (1997).
Perry, I. J. et al. Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged British men. Lancet. 346, 1395–1398 (1995).
Towfighi, A., Saver, J. L., Engelhardt, R. & Ovbiagele, B. Factors associated with the steep increase in late-midlife stroke occurrence among US men. J Stroke Cerebrovasc Dis. 17, 165–168 (2008).
Selhub, J. et al. Association between plasma homocysteine concentrations and extracranial carotid-artery stenosis. N Engl J Med. 332, 286–291 (1995).
McQuillan, B. M., Beilby, J. P., Nidorf, M., Thompson, P. L. & Hung, J. Hyperhomocysteinemia but not the c677t mutation of methylenetetrahydrofolate reductase is an independent risk determinant of carotid wall thickening. The perth carotid ultrasound disease assessment study (cudas). Circulation. 99, 2383–2388 (1999).
Kim, S. J. et al. Biomarkers of asymptomatic carotid stenosis in patients undergoing coronary artery bypass grafting. Stroke. 42, 734–739 (2011).
Maron, B. A. & Loscalzo, J. The treatment of hyperhomocystenemia. Annu Rev Med. 60, 39–54 (2009).
Loscalzo, J. Homocysteine-mediated thrombosis and angiostasis in vascular pathobiology. J Clin Invest. 119, 3203–3205 (2009).
Toole, J. F. et al. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction and death: The vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA 291, 565–575 (2004).
Lonn, E. et al. Heart outcomes Prevention Evaluation (HOPE) 2 Investigators: Homocysteine lowering with folic acid and B vitamins in vascular disease. N Engl J Med. 354, 1567–1577 (2006).
Bønaa, K. H. et al. NORVIT Trial Investigators: Homocysteine lowering and cardiovascular events after acute myocardial infarction. N Engl J Med. 354, 1578–1588 (2006).
Cardoso, C. R. et al. Factors associated with carotid intima-media thickness and carotid plaques in type 2 diabetic patients. J Hypertens. 30, 940–947 (2012).
Simon, A. et al. Intima-media thickness: a new tool for diagnosis and treatment of cardiovascular risk. J Hypertens. 20, 159–169 (2002).
O'Leary, D. H. et al. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med 340, 14–22 (1999).
Chambless, L. E. et al. Carotid wall thickness is predictive of incident clinical stroke. The Atherosclerosis Risk in Communities (ARIC) study. Am J Epidemiol 151, 478–487 (2000).
Staub, D. et al. Prediction of cardiovascular morbidity and mortality: comparison of the internal carotid artery resistive index with the common carotid artery intima-media thickness. Stroke. 37, 800–805 (2006).
Kurata, M., Okura, T., Watanabe, S. & Higaki, J. Association between carotid hemodynamics and asymptomatic white and gray matter lesions in patients with essential hypertension. Hypertens Res. 28, 797–803 (2005).
van Dijk, S. C. et al. Homocysteine level is associated with aortic stiffness in elderly: cross-sectional results from the B-PROOF study. J Hypertens. 31, 952–959 (2013).
Lim, M. H., Cho, Y. I. & Jeong, S. K. Homocysteine and pulsatility index of cerebral arteries. Stroke 40, 3216–3220 (2009).
Jacques, P. F. et al. Serum total homocysteine concentrations in adolescent and adult Americans: results from the third National Health and Nutrition Examination Survey. Am J Clin Nutr. 69, 482–489 (1999).
Ricotta, J. J. et al. Up dated society for vascular surgery guidelines for management of extracranial carotid disease. J Vasc Surg. 54, e1–e31 (2011).
Matsuo, S. et al. Collaborators developing the Japanese equation for estimated GFR: Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 53, 982–992 (2009).
Manabe, S., Okura, T., Watanabe, S. & Higaki, J. Association between carotid haemodynamics and inflammation in patients with essential hypertension. J Hum Hypertens. 19, 787–791 (2005).
Rifkin, M. D. et al. Evaluation of renal transplant rejection by duplex Doppler examination: value of the resistive index. Am J Roentgenol. 148, 759–762 (1987).
Okura, T. et al. Long-term effects of angiotensin II receptor blockade with valsartan on carotid arterial stiffness and hemodynamic alterations in patients with essential hypertension. Clin Exp Hypertens. 30, 415–422 (2008).
Hoffman, M. Hypothesis: hyperhomocysteinemia is an indicator of oxidative stress. Med Hypotheses. 77, 1088–1093 (2011).
McCully, K. S. & Ragsdale, B. D. Production of arteriosclerosis by homocysteinemia. Am J Pathol. 61, 1–11 (1970).
Marti-Carvajal, A. J. et al. Homocysteine-lowering interventions for preventing cardiovascular events. Cochrane Database Syst Rev. 1, CD006612 (2013).
Spence, J. D. & Stampfer, M. J. Understanding the complexity of homocysteine lowering with vitamins: The potential role of subgroup analyses. JAMA. 306, 2610–2611 (2011).
Spence, J. D. B vitamin therapy for homocysteine: Renal function and vitamin B12 determine cardiovascular outcomes. Clin Chem Lab Med. 51, 633–637 (2013).
Debreceni, B. & Debreceni, L. Why do homocysteine-lowering B vitamin and antioxidant E vitamin supplementations appear to be ineffective in the prevention of cardiovascular diseases? Cardiovasc Ther. 30, 227–233 (2012).
Author information
Authors and Affiliations
Contributions
T.O. and J.H. wrote the main manuscript text. K.M., J.I., D.E., T.N., M.K., A.T., K.K. and Z.P. carried out performing carotid ultrasound. All authors read and reviewed the manuscript.
Ethics declarations
Competing interests
Dr. Higaki received research grants and speaker honoraria from Pfizer Inc., Asteras Co., Takeda Pharm Co., Beringer-Ingerheim Japan Co., Daiichi-Sankyo Co., MSD Co., Mochida Pharm Co., Novartis Pharm. Co. and DaiNihon-Sumitomo Co. The other authors have indicated that they have no conflicts of interest with regards to the contents of this article.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Okura, T., Miyoshi, Ki., Irita, J. et al. Hyperhomocysteinemia is one of the risk factors associated with cerebrovascular stiffness in hypertensive patients, especially elderly males. Sci Rep 4, 5663 (2014). https://doi.org/10.1038/srep05663
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep05663
This article is cited by
-
The association of homocysteine level with the risk of diabetic nephropathy and diabetic retinopathy in NHANES
Acta Diabetologica (2023)
-
Association of homocysteine with carotid atherosclerosis in hypertension
Journal of Human Hypertension (2022)
-
Association between homocysteine and conventional predisposing factors on risk of stroke in patients with hypertension
Scientific Reports (2018)
-
Association between H-type Hypertension and Asymptomatic Extracranial Artery Stenosis
Scientific Reports (2018)
-
Link between Homocysteine and Cardiovascular Diseases
Current Pharmacology Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
