
Key Points
-
Highlights the importance of photography as a tool in the referral process in addition to a good quality referral letter.
-
Encourages dentists to consider photography in all suspicious and potentially sinister oral lesions.
-
Promotes the need for further research when referring patients into secondary care using the fast improving and increasingly accessible technology
Abstract
Objective To determine whether the use of referral letters with and without photography will make a difference to prioritising patients to the oral medicine department.
Design Retrospective analysis.
Setting Oral medicine department of Birmingham Dental Hospital.
Method Forty-eight photographs were randomly selected using a database of clinical photographs. This was whittled down to 25 photographs after exclusion criteria were met. Referral letters that corresponded to the photographs were found and anonymised. Ten clinicians of varying experience (from consultant level to house officers) then filled out three separate forms: the first form to prioritise patients with referral letters alone, the second to prioritise patients with both referral letters and their matching photographs and the third to prioritise patients with referral letters, photographs and the final diagnosis of the patient's condition.
Results It was found that photographs made a difference to the appointment prioritisation of a patient in 37% of cases on average. 8.6% of the time, on average, photographs led to an inappropriate appointment prioritisation being selected. On average, 41.1% of the time the most appropriate appointment priority was chosen regardless of whether photography was used or not; on average 21.2% of the time, the most appropriate appointment priority was chosen only as a direct result of the clinician viewing the patient photography. In cases of malignancy, regardless of the experience of the clinician, not a single clinician was misled into making an inappropriate appointment prioritisation by the presence of a photograph. There is evidence to suggest that photographs lead to an increase in patient prioritisation regardless of whether this was appropriate or not.
Conclusion From the results of this study the use of photographs in addition to a referral letter appears to be very useful in helping oral medicine consultants to prioritise new patient appointment for their initial consultation. This seems especially true in cases of oral cancer.
Similar content being viewed by others

Background
The oral medicine referral system at present is based upon an oral medicine specialist, in most cases, interpreting a primary care referral letter and using that information to place the patient into a certain referral category based on the perceived seriousness of their condition.
Although a fixed system for the prioritisation of patient appointments (ie referral urgency) does not exist, Birmingham Dental Hospital (where this study was carried out) has adopted a triage system. The categories (along with the hospital waiting times) are:
-
1
A patient with a condition/lesion that is perceived to pose a significant risk of mortality (for example, suspected oral malignancy) and/or morbidity (for example, trigeminal neuralgia) – to be seen within two weeks
-
2
A patient with no suspected oral malignancy but a condition/lesion that it is perceived may potentially pose a risk of mortality or morbidity – to be seen within four to six weeks
-
3
A patient with a 'routine' condition/lesion that is perceived not to pose any significant risk of mortality or morbidity – to be seen within 11-13 weeks.
In practice it can be difficult to assign the patient referral urgency as the referral system relies heavily upon the quality of the referral letter.1,2
Recent studies into the quality of oral medicine referrals by Navarro et al.,3,4 which compared the use of standard and non-standard referral letters to oral medicine specialists, found that standard letters were more complete and contained important information commonly absent in non-standard letters. However, the studies also revealed that regardless of the type of referral letter, much of the essential information that one would expect in any referral letter was generally omitted (eg the patient's age and address). This may potentially lead to delays in patient diagnosis and treatment.3,4
In considering how oral medicine referrals could be improved we have encountered the use of telemedicine as a potential solution in helping the referrer improve referral into the specialist arena. Telemedicine is a broad term that encompasses the use of telecommunication in doctor-patient as well as doctor-doctor interaction. It can be as simple as a dentist using a telephone to get advice from a specialist or as complex as the use of real-time video conferencing between specialists when deciding upon appropriate treatment for a patient.5
Telemedicine has been used in many medical specialities. It is most commonly used in the radiography setting to transfer radiographs digitally within and between hospitals and is often known as 'teleradiography'. Other specialities include cardiology, pathology and dermatology. Recently Oakley et al.6 examined the diagnostic value of written referral with and without the use of photography in the dermatology speciality. The study concluded that dermatologists were less confident in their ability to diagnose a skin lesion than would be the case with a face-to-face consultation and were therefore more likely to suggest an invasive procedure and/or follow up appointments.6
Telemedicine is still in its infancy within the dental setting and there have been few studies carried out on 'teledentistry'. A recent study looked at the use of digital photography as an aid for orthodontic referral with apparently positive results, suggesting that teledentistry could be a 'significant factor' in helping to reduce inappropriate referrals and encourage appropriate referral.7
From the above studies it can be noted that the efficacy of telemedicine, especially when considering referral and diagnosis, is quite ambiguous. From the literature available, a study evaluating the use of teledentistry in the oral medicine setting has not at present been carried out, and its impact on oral medicine referral and diagnosis is unknown. The aim of this study is therefore to find out what type of effect teledentistry would have upon oral medicine referral and diagnosis.
Aims and objectives
The aim of this project was to distinguish if there is any change in appointment prioritisation of a patient when comparing the patient's referral letter with and without a photograph of that patient's oral lesion.
Method
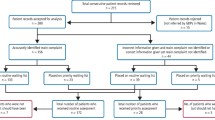
Forty-eight patients seen at the oral medicine department of Birmingham Dental Hospital were found using a database of clinical photographs. At this stage any conditions where a photograph was of no clinical use (eg burning mouth syndrome, atypical facial pain) were excluded from the study. Photography showing the faces of patients were also excluded at this stage.
The clinical notes of the remaining patients were then requested. Patients were excluded at this stage if any of the following occurred:
-
The clinical notes could not be located
-
The referral letter (to the oral medicine specialist) could not be found in the patient notes
-
The referral letter was not related to the photograph of the oral lesion
-
The clinical notes did not reveal a final diagnosis of the oral lesion.
Ultimately, 25 appropriate patients were found.
Referral letters from each patient were scanned using a Hewlett Packard ScanJet 4300C and converted into JPEG files. The referral letters were then anonymised using Microsoft Paint® to black out details of the patient's name and address and the referrer's name and address. The anonymised referral letters were each given a number from 1-25 and were matched with their complementary colour photograph. The 25 patients were then divided into two groups. This was simply done to reduce the workload of any one clinician at any one particular time. Group 1 consisted of patients 1-13 and Group 2 consisted of patients 14-25.
Four types of CDs were then created:
-
CD1a – referral letters of patients 1-13
-
CD1b – referral letters and photographs of patients 1-13
-
CD2a – referral letters of patients 14-25
-
CD2b – referral letters and photographs of patients 14-25.
All participating clinicians were given CD1a and CD1b first and were subsequently given the option of completing the second half of the study (ie Group 2 patients) if they chose to do so. The clinicians were asked to fill in Form A using CD1a only and Form B using CD1b. Finally Form C (part one) was filled using CD1b, where the final diagnosis was revealed and the clinicians decided on the actual level of urgency and the actual usefulness of the photographs. These steps were repeated for patients 14-25 using CD2a and CD2b and using Form C (part two). Clinicians were given a step-by-step guide sheet to ensure that the three forms above were completed in the correct order. Copies of the forms can be found in appendices 1-4.
The 25 photographs selected were all colour photos taken by the hospital photographic department. The photos were of a good quality and resolution ranged from 500 × 500 dpi (dots per inch) to 1,350 × 1,350 dpi. All participating clinicians viewed the images on PC/laptop monitors using Windows Photo Gallery® software. To preserve the anonymity of the ten clinicians involved in the study, the following letters were assigned to the group of clinicians:
-
Senior oral medicine staff: Clinician A, Clinician B, and Clinician C
-
Junior oral medicine staff: Clinician Q, Clinician R, and Clinician S
-
Senior house officers (SHOs): Clinicians X, Clinician Y, and Clinician Z (Clinicians X represents two clinicians who chose to complete the forms jointly).
Results
Of the ten clinicians participating in the project, all answered questions from Forms A, B and C for patients 1-13 and two senior clinicians (Clinicians A and B) additionally answered questions regarding patients 14-25.
Comparing referral urgency with and without photography
By comparing the referral urgency before and after the availability of a photograph it is possible to find out if the photograph led to a change in the referral urgency, as can be illustrated by Figure 1. On average, photographs led to the greatest change in referral urgency in the senior clinicians group, with 46.2% changing; this was followed by the SHO group (41.0%). The junior staff showed least change with 23.1%. Figure 1 shows that on average, 37% of the time, the patient photographs made a difference to the referral urgency. However it does not illustrate whether the referral urgency was improved or worsened by the photograph.

Graph illustrating whether there was a change in referral urgency when comparing referral letters alone to the same referral letter with its corresponding photograph
From Forms A, B and C, clinicians were asked the following regarding the referral urgency:
-
Using the referral letter ONLY, select the degree of referral urgency (Form A)
-
Using the referral letter and photograph, select the degree of referral urgency (Form B)
-
With respect to the final diagnosis, select the degree of referral urgency (Form C).
From these three questions it is possible to assess whether the patient photographs led to the ideal referral urgency for the seriousness of that patient's condition. However in order to answer this question the 'ideal' referral urgency needs to be defined. Depending on the individual clinicians' personal experiences it is possible that two different clinicians could select two different referral categories for the same patient, even though they have both read the same referral letter and seen the same photograph. Also there are very few guidelines as to which conditions merit rapid consultation (with the exception of oral cancer) and which conditions do not.
In light of the above it is difficult to justify the use of the referral urgency that the author would deem to be the most suitable for each of the 25 patients. Instead the referral urgency selected in Form C when the clinician has seen the referral letter and the photograph and knows the final diagnosis would seem to be the most appropriate referral urgency. This set 'ideal' referral urgency can then be compared to the referral urgencies selected by using the referral letter alone and the letter with a photo. By using this fixed reference point it is possible to see if the photograph has led to a more urgent or less urgent referral for each patient.
Figure 2 illustrates the comparison of the referral urgencies using the referral letter with and without the photograph to the post-diagnosis referral urgency. To understand the method by which the data has been correlated into four groups in Figure 2, Table 1 illustrates examples for each group. In the red group the referral letter led to the most appropriate referral urgency being selected, however the presence of the photograph led to an inappropriate urgency being selected. When comparing between the groups of clinicians, in the SHO group there were 5 out of 39 (12.8%) occasions were the photograph lead to an inappropriate referral urgency being selected. There was little difference between the junior clinicians (5.1%) and senior clinicians (7.9%). Of the 12 occasions (from a potential 141) where the photograph led to the incorrect referral urgency being selected, 11 patients' referral urgency was inappropriately increased so that the patients would be seen sooner.

Red group: the referral letter led to the 'ideal' referral urgency being selected but the photo led to the wrong referral urgency being selected. Yellow group: the referral letter with and without the photo led to the 'ideal' referral urgency being selected. Green group: the referral letter led to the wrong referral urgency being selected but with the photo the 'ideal' referral urgency was selected. Blue group: the referral letter with or without the photo led to a referral urgency other than the 'ideal' being selected
In the yellow group, the referral letter both with and without photography led to the ideal referral urgency being selected. Junior staff had the most cases of this with 46.2%, followed by the senior (41.3%) and SHO (35.9%) groups. These results should be interpreted with care as the 'ideal' referral urgency was selected after the referral letter was read – meaning that the photograph may have played little part in the subsequent referral urgency selection with the photograph or that the photograph was important in confirming the original referral urgency selection. However, taking into account the '...how useful was the photograph in helping you select the referral category?' question on Form B, which generally scored highly, it is most probable that the photos were an important factor in confirming the referral urgency.
In the green group, photography was crucial in selecting the ideal referral category. There was more variation between the clinicians regarding these results, with senior staff scoring the highest (30.2%), followed by SHO (23.1%) and junior staff (10.3%). In this group of patients, when analysing how the referral urgency changed due to the photographs it can be noted that in 22 out of 32 cases the photograph led to the patient being seen sooner, and in 10 out of 32 cases photography led to a downgrading of the referral urgency.
There were occasions where all clinicians (regardless of their experience) were unable to select the ideal referral urgency either with the referral letter alone or with the referral letter and the photograph.
Malignancy cases only
There were three cases of malignancy in each of Groups 1 and 2. Figure 3 shows the results for only the cases presenting with a very significant mortality risk (ie cancer). From the graph it can be seen that regardless of the experience of the clinician, not a single clinician was misled by the presence of the photograph and no clinician downgraded the referral urgency of a patient that was subsequently found to have a malignancy. Conversely, on 14 occasions the presence of the photograph led to an increased suspicion of the subsequent malignant lesion (which would not have been possible with the referral letter alone). Of these fourteen occasions where the referral urgency was upgraded to 'within 2 weeks' as a direct result of the photograph, five were upgraded from the 11-13 weeks referral urgency list and nine were upgraded from the 4-6 week referral urgency list.

The key is the same as in Figure 2. In oral cancer the ideal referral category is always 'Within 2 weeks'
Senior clinicians were the only group where all patients subsequently diagnosed with oral cancer were initially allocated to the 'within 2 weeks' referral urgency category either after referral letters alone were seen (yellow group) or after referral letters and photos were seen (green group).
Discussion
Consultants in oral medicine have the responsibility of prioritising patient referrals. Although a range of clinicians of varying experience in oral medicine participated in this study, arguably the results obtained for the senior oral medicine staff should be seen to be the most significant, as these are the individuals that will decide how urgently a patient should be seen at the oral medicine department. An important finding that appears to promote the argument to include photos as part of a GDP's referral letter is the fact that senior clinicians were responsible for the highest proportion of the ideal referral urgencies selected as a direct result of a photograph of the patient's intra-oral lesion.
Perhaps the most significant finding from this study is regarding the use of photography for lesions subsequently found to be oral cancer. All clinicians (regardless of experience) recognised from the photographs that such a lesion should be seen as soon as possible. On 14 occasions it was only when the clinicians were shown the photograph of the lesion that they suspected it, as the referral letter raised little or no concern of a potential malignancy. Encouragingly, all the senior clinicians were able to correctly categorise patients subsequently found to have oral cancer to the 'within 2 weeks' referral urgency group in all the cases where a photograph of such a lesion was made available.
The comments by clinicians participating in the study were generally positive and they regarded photography as a useful addition to a referral letter:
'Photos of all these cases greatly enhanced differential diagnosis [and] referral category selection.'
'The photos help to narrow the possible diagnosis.'
However, there appears to be a general trend of photographs leading to the upgrading of the referral urgency, regardless of whether this led to the 'ideal' referral urgency or not. In circumstances where the photo led to an inappropriate referral urgency selection, 92% of patients were upgraded. Conversely, the referral urgency of two-thirds of patients was upgraded to the most appropriate referral urgency with the use of photography.
Conclusion
-
From the results of this study, the use of photographs would appear to be a very useful referral addition in helping oral medicine consultants prioritise new patient appointments for their initial consultation. This seems to be especially true in cases of oral cancer
-
From the findings of this study it would seem appropriate for all referring GDPs to consider including photographs of all suspicious lesions, especially where there is concern that the lesion could be sinister
-
Although photography seems useful, it is not a substitute for a referral letter and a good quality referral letter is still the most important factor in ensuring prompt referral. It is also important to note that the images used in this study were of a good quality. GDPs should be wary of sending inferior quality photographs with their referrals as this may hinder rather than help in prioritising patients
-
More research into this subject is required to produce a firm conclusion on the use of photography in oral medicine referral. This study has shown that its use may be of significant benefit to oral medicine consultants and therefore in the efficient treatment of patients.




References
McAndrew R, Potts A J, McAndrew M, Adam S . Opinions of dental consultants on the standard of referral letters in dentistry. Br Dent J 1997; 182: 22–25.
Marinker M, Wilkin D, Metcalfe D H . Referral to hospital: can we do better? BMJ 1988; 297: 461–464.
Navarro C M, Miranda I A N, Onofre M A, Sposto M R . Referral letters in oral medicine: standard versus non-standard letters. Int J Oral Maxillofac Surg 2002; 31: 537–543.
Navarro C M, Onofre M A, Sposto M R . Referral letters in oral medicine: an approach for the general dental practitioner. Int J Oral Maxillofac Surg 2001; 30: 448–451.
Wootton R. Telemedicine. BMJ 2001; 323: 557–560.
Oakley A M, Reeves F, Bennett J, Holmes S H, Wickham H . Diagnostic value of written referral and/or images for skin lesions. J Telemed Telecare 2006; 12: 151–158.
Mandall N A, O'Brien K D, Brady J, Worthington H V, Harvey L . Teledentistry for screening new patient orthodontic referrals. Part 1: a randomised control trial. Br Dent J 2005; 199: 659–662.
Acknowledgements
Thank you to the following people who made this project possible: Andrea Richards, Susan Roche, Michael Betteridge, Harriet Anstey, Daniel Saund, Ingrid Hughes, Arijit Ray-Chaudhuri, Naveen Karir, Martin Ling, Shekha Bhuva and Norma Williams.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Aslam, A., Hamburger, J. Does the use of photography help to prioritise patients when referring to the oral medicine department?. Br Dent J 208, E16 (2010). https://doi.org/10.1038/sj.bdj.2010.396
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2010.396
This article is cited by
-
Remote dental screening by dental therapists
BDJ Team (2016)
-
Validity and reliability of remote dental screening by different oral health professionals using a store-and-forward telehealth model
British Dental Journal (2016)
-
Summary of: Does the use of photography help to prioritise patients when referring to the oral medicine department?
British Dental Journal (2010)
