
Abstract
Study design:
Multicenter, prospective study.
Objectives:
To assess the occurrence and predictors of return to work after traumatic spinal cord injury (SCI).
Setting:
Italian rehabilitation centers.
Methods:
We evaluated patients previously included in the Italian Group for the Epidemiological Study of Spinal Cord Injuries study. A standardised telephone interview was used to collect data after a mean follow-up of 3.8 years. The main outcome measure was employment at the end of follow-up.
Results:
A total of 403 patients, 336 men and 67 women, with a mean age of 41.8±16.3 years, were included in the follow-up. In all, 42.1% of patients were employed at the moment of the interview, though 62% reported a worsening in their employment level. Predictors of employment were education (P<0.0001), bowel continence (P=0.02), independence in mobility (P=0.0004), ability to drive (P<0.0001), participating in the community (P=0.0001) and ability to live alone (P<0.0001) while age (P<0.0001), being married (P<0.0001), tetraplegia (P=0.03), occurrence of recent medical problems (P=0.002), re-hospitalization (P=0.02), presence of architectonic barriers (P=0.009) and having a public welfare subsidy (P<0.0001), predicted unemployment. On the basis of multivariate analysis, younger age, education, absence of tetraplegia, ability to drive, ability to live alone, previous employment were independent predictors of employment after SCI. Employment at follow-up was related to several indicators of quality of life.
Conclusion:
Employment after SCI was rather frequent and was related to several patient characteristics and social factors. Specific interventions on the patient and on the social environment may favor employment after SCI and improve quality of life.
Similar content being viewed by others


Introduction
Employment of disabled people is considered one of the best indicators of full independence, social integration and quality of life.1, 2, 3 For this reason rehabilitation teams consider return to work a primary indicator of successful treatment.4
Spinal cord injuries (SCI) often causes serious disability in young people with a severe impact on social activities and employment thus producing relevant lifelong social and economic costs.5 Indeed subjects with SCI are more likely than non disabled subjects to consider employment as an hallmark of personal satisfaction and of social achievement.4 However, apart from level of functioning, several factors may influence tendency to return to work and their identification may be particularly relevant to plan interventions that may increase the likelihood of employment after SCI.1, 6, 7, 8, 9, 10
Owing to physical limitations, patients with SCI are at risk of developing a hypoactive lifestyle with negative effects on physical fitness, social participation and quality of life, as well as on secondary health problems.7 Therefore, employment after SCI may have a relevant impact on perceived quality of life of such subjects.
The aim of this study was to assess occurrence and predictors of employment among subjects with SCI and to evaluate its impact on perceived quality of life.
Patients and methods
This multicenter, prospective study assessed long-term outcome of patients previously included in the GISEM (Italian Group for the Epidemiological Study of Spinal Cord Injuries) study.11 The study group included 24 SCI centers, 17 Italian rehabilitation centers, and 7 Spinal units.
Eligibility criteria for inclusion in the GISEM II study required that SCI was caused by a traumatic event, and patients were discharged between 1997 and 1999 from the Rehabilitation Center where they were admitted after SCI.11 As we were interested in any kind of employment after SCI, subjects were included regardless of their employment status at the time of the injury or of age at the time of study assessment. Written informed consent was obtained from each participant, according to the European Community Good Clinical Practice guidelines and local regulations.
Follow-up was planned after 4 years from inclusion, by means of a 24-items standardised telephone questionnaire whose reliability had been validated on a sample of SCI people.12 Items such as health status and management of clinical conditions, emotional relationships, perceived quality of life, autonomy, independence in mobility, employment, social integration were the items investigated in the questionnaire. The information regarding employment status included maintenance or loss of previous job, changes in job characteristics (job type, timetable, salary and other variables) and start of work for the first time. Every individual formally involved in any regular job, either self-employed or employed in any public or private organization, and subjects involved in any formal study course were considered as employed. Perceived quality of life was self-assessed on a numerical rating scale from 0 to 10 points. The subjects were all personally interviewed.
The main outcome measure was status and level of employment at the end of follow-up. Independent variables were demographic and clinical characteristics recorded at admission to Hospital in the acute phase, as well as factors related to autonomy, independence in mobility, ability to live alone, defined as having been home alone for at least 3 days or thinking of being able to do so, social integration and perceived quality of life at follow-up. A full list of variables and definitions has been reported elsewhere.12
Statistical analysis
χ2 test and analysis of variance were used to compare subjects with or without employment, as appropriate. The association between employment at follow-up and independent variables was evaluated at the univariate analysis by means of odds ratios (OR) and 95% confidence intervals (CI) according to the Mantel–Haenszel method. Logistic regression analysis was used to asses independent predictors of employment at multivariate analysis.
Results
Participants and follow-up
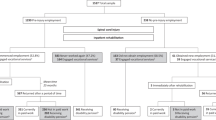
Out of 608 subjects included in the GISEM study between 1997 and 1999, 403 (72.2%) completed the interview (336 men and 67 women); 72 refused to participate, 36 had died and 97 were irretrievable. The mean age of the included patients was 41.8±16.3 years. Baseline characteristics at admission in Hospital in acute phase are reported in Table 1. Most patients suffered from a severe spinal cord lesion (65%) graded as ASIA scale level A (50.1%) or B (12.7%) and 36.8% had a tetraplegia according to the ASIA International neurological standard. The etiology of SCI in this traumatic population was represented in great majority by road accidents (229, 56.9%), followed by accidental falls (88, 21.9%), sport accidents (38, 9.4%), attempted suicide (11, 2.7%) and violence (6, 1.4%). In the remaining 31 cases (7.7%) the SCI was due to a miscellaneous of causes or unknown.
The mean duration of follow-up was 3.8 years (range, 2.7–5.2). Employment status at the end of follow-up and changes on employment characteristics are reported in Table 2. No relationship was found between length of time from hospital discharge and employment status (P=0.50). Almost half of the subjects (42.1%) were employed as workers (34.7%), students (7.2%) or both (0.2%): 149 subjects (43.7%) had lost their previous employment, whereas 4 subjects (2.0%) had gained a position of employment for the first time in their life. Furthermore, among employed subjects, many workers had changed job type, job timetable or other job characteristics, while few students reported changes in their study behavior (Table 2). Considering the income, 250 (62.0%) subjects referred a worsening in their employment position.
Among the subjects who were unemployed, the main causes were difficulty to find a suitable job (31.9%), public welfare subsidy (31.0%) and industrial accident insurance (34.1). The source of economic livelihood was welfare subsidy in 61.3% of subjects and salary in 34.7%, even though many subjects reported an underpaid job (15.1%).
Predictors of post-injury employment
Subjects who were employed at follow-up were younger (33.8±11.5 years) than those who remained unemployed (47.6±16.8 years; OR 0.94; 95% CI 0.92–0.95), had an education of 8–13 years (76.5% vs 62.2%; OR 4.2; 95% CI 2.7–6.6) or >13 years (14.1% vs 3.4%; OR 8.6; 95% CI 3.7–20.5) and were less often married (21.8% vs 57.9%; OR 0.2; 95% CI 0.1–0.3; Table 3).
Patients with a tetraplegia were more often unemployed than those with lower spinal lesions (OR 0.6; 95% CI 0.4–0.9). Functional status was relevant to employment because subjects with bowel continence (OR 1.8; 95% CI 1.1–2.9), independence in mobility (OR 3.0; 95% CI 1.7–5.6), ability to drive (OR 4.9; 95% CI 2.9–8.3), participating in the community (OR 2.5; 95% CI 1.5–4.0) and those able to live alone (OR 3.6; 95% CI 2.3–5.6) are more often employed. Occurrence of medical problems (OR 0.5; 95% CI 0.4–0.8) and of re-hospitalization (OR 0.6; 95% CI 0.4–0.9) in the last 6 months predicted unemployment, as well as house architectonic barriers (OR 0.5; 95% CI 0.3–0.8). Among social factors, previous employment (OR 15.4; 95% CI 5.5–43.2) was strongly related to employment while having a welfare subsidy (OR 0.1; 95% CI 0.05–0.2) was related to unemployment.
On the basis of multivariate analysis, education, ability to drive, ability to live alone and previous employment were independent predictors of employment at follow-up, while older age and tetraplegia predicted unemployment (Table 4).
Perceived quality of life
Patients who were employed had an overall better perceived quality of life (mean numerical rating scale score of 6.9±2. 2 vs 5.3±2.8; P<0.0001). They reported a more satisfying sex life (P=0.02), were more likely to leave home for leisureliness (P<0.0001), and practised more hobbies (P=0.002) and sports (P<0.0001), despite complaining of fewer social contacts in leisure time (P=0.007; Table 5).
Discussion
In this follow-up study almost half of the subjects were employed after 4 years of follow-up, although 43.7% of the subjects reported loss of previous job many workers had changed job characteristics, and 62% reported a worsening of their previous income level as a consequence of the trauma. Several factors related to demographic characteristics, clinical status and social factors predicted employment, but only younger age, education, absence of tetraplegia, ability to drive, ability to live alone and previous employment were independent predictors of employment at the multivariate analysis.
The importance of this study rely on the lack of data on employment after SCI in Italy where regulations and job availability are rather different from other European countries. The study included a cohort of subjects treated in specialised centers, most of which were Spinal Units. Although we used phone interview for follow-up evaluation, all subjects were contacted in person and reliability of outcome assessment with the structured questionnaire was high, because an ad hoc study reported a global agreement ranging between 79 and 100% for most of the items.12
Our results match well with those of previous studies in which the percentages of vocational reintegration after SCI varied from 25 to 65% of cases and increased with time from hospital discharge.1, 4, 10, 13, 14, 15 Actually, the proportion of employment of our patients (42.1%) was in the range of other studies, even though the mean age of our population was rather high, the majority of patients had a cervical lesion, and the duration of follow-up was of 4 years. In our opinion this should be considered a good result, considering that at the time of the study, in Italy was very difficult to find a job for people who had lost an employment at advanced age, mostly when disabled.6 The lack of correlation between length of time from hospital discharge and employment status in our study probably indicates that follow-up was long enough to allow employment of subjects capable of working or studying and that the rate of employment was unlikely to increase further. In a recent study, 50% of subjects who returned to work after SCI had done so by 4 years and employment, mostly when due to return to pre-injury employer, was associated with early return.
Age and cervical spinal cord lesions are among the most important predictors of post-injury employment.6, 13 Because they are un-modifiable factors in affected patients, and they are likely to produce high economic and social costs, prevention programs should be implemented to prevent subjects from remaining severely dependent for many years. Moreover, as the occurrence of medical problems, re-hospitalization and frequency of follow-up visits also predicted unemployment, probably as a consequence of frequent attendance of medical services, dedicated medical routes should be adopted to reduce time spent for medical assistance.16
In our study, education was a strong independent predictor of employment after SCI, with a clear increasing trend, according to the length of education period. The explanation for this impressive association probably depends on the larger availability of job for intellectual work and the lower impact of physical disabilities on intellectual activities.4, 6, 15 Subjects with high educational level may also have more autonomy, more motivation and more positive personal expectations.17 On the other hand, the Italian welfare system, although important for economic support of patients with SCI, is mainly focused on compensation rather than on facilitating employment of subjects with disabilities.18 Therefore, welfare policies should be amended and work preparation programs should be adopted in order to favor employment of patients with SCI.18
Patients who were able to live alone were more likely to be employed, as well as those unmarried suggesting that stimulating a patient's attitude toward self-sufficiency may favor employment. However, architectonic barriers influencing the patient's ability to leave home alone, and ability to drive, helping to reach work place, are also relevant for employment after SCI. Thus, building policies aimed to reduce any kind of architectonic barriers may be of great relevance for employment of disabled patients.19 Moreover, rehabilitation programs should also focus on abilities to drive, use of public transportations and of any device helpful to overcome any kind of barrier to independence in mobility.
Quality of life after SCI has been addressed in a few studies showing that it was independently associated with employment status in the long-term period.7, 20 Our study confirmed that employment after SCI was strongly correlated with perceived quality of life, and social activities such as practicing a sport or a hobby, leaving home in leisure and more satisfying sex life, although social contacts in leisure time were reduced by work activities. Of course, the main explanation for these associations rely on the functional status of the patients, which is very relevant to both ability to work and quality of social contacts. However, some leisure and social activities, such as sport, can also favor employment while the latter may in turn favor social contacts, physical activities, hobbies and entertainment.20 Therefore, we should consider that most of programs put into practice to improve employment after SCI may also improve perceived quality of life and thus should be strongly favored.
In conclusion, our study strongly support the view that several interventions may favor employment after SCI. Rehabilitation programs should go beyond the approach focused on in-house activities and bridge to occupational therapy and social reintegration. On the other hand, although welfare subsidy is of great public relevance, social policies should also focus on educational training and work preparation programs to favor employment and improve quality of life.
Data Archiving
There were no data to deposit.
References
MacKenzie EJ, Shapiro S, Smith RT, Siegel JH, Moody M, Pitt A . Factors influencing return to work following hospitalization for traumatic injury. Am J Public Health 1987; 77: 329–334.
Noreau L, Dion SA, Vachon J, Gervais M, Laramée MT . Productivity outcomes of individuals with spinal cord. Spinal Cord 1999; 37: 730–736.
Krause JS, Coker JL . Aging after spinal cord injury: a 30-year longitudinal study. J Spinal Cord Med 2006; 29: 371–376.
Schönherr MC, Groothoff JW, Mulder GA, Schoppen T, Eisma WH . Vocational reintegration following spinal cord injury: expectations, partecipation and interventions. Spinal Cord 2004; 42: 177–184.
Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC, Wuermser LA, Ho CH . Spinal cord injury medicine. 6. economic and societal issues in spinal cord injury. Arch Phys Med Rehabil 2007; 88 (3 Suppl 1): S84–S88.
Pflaum C, McCollister G, Strauss DJ, Shavelle RM, DeVivo MJ . Worklife after traumatic spinal cord injury. J Spinal Cord Med 2006; 29: 377–386.
Lidal IB, Hjeltnes N, Røislien J, Stanghelle JK, Biering-Sørensen F . Employment of persons with spinal cord lesions injured more than 20 years ago. Disabil Rehabil 2009; 31: 2174–2184.
Krause JS, Terza JV, Saunders LL, Dismuke CE . Delayed entry into employment after spinal cord injury: factors related to time to first job. Spinal Cord 2010; 48: 487–491.
Anzai K, Young J, McCallum J, Miller B, Jongbloed L . Factors influencing discharge location following high lesion spinal cord injury rehabilitation in British Columbia, Canada. Spinal Cord 2006; 44: 11–18.
Lin MR, Hwang HF, Yu WY, Chen CY . A prospective study of factors influencing return to work after traumatic spinal cord injury in Taiwan. Arch Phys Med Rehabil 2009; 90: 1716–1722.
Pagliacci MC, Celani MG, Spizzichino L, Zampolini M, Aito S, Citterio A et al. on behalf of GISEM Spinal Cord Lesion management in Italy: two years survey. Spinal Cord 2003; 41: 620–628.
Franceschini M, Di Clemente B, Citterio A, Pagliacci MC . Follow-up in persons with traumatic spinal cord injury: questionnaire reliability. Eura Medicophys 2006; 42: 211–218.
DeVivo MJ, Rutt RD, Stover SL, Fine PR . Employment after spinal cord injury. Arch Phys Med Rehabil 1987; 68: 494–498.
Tomassen PCD, Post MWM, van Asbeck FW . Return to work after spinal cord injury. Spinal Cord 2000; 38: 51–55.
Ramakrishnan K, Mazlan M, Julia PE, Abdul Latif L . Return to work after spinal cord injury: factors related to time to first job. Spinal Cord 2011; 49: 1–4.
Donnelly C, McColl MA, Charlifue S, Glass C, O'Brien P, Savic G et al. Utilization, access and satisfaction with primary care among people with spinal cord injuries: a comparison of three countries. Spinal Cord 2007; 45: 25–36.
Ottomanelli L, Lind L . Spinal cord injury:implications for research and vocational services. J Spinal Cord Med 2009; 32: 503–531.
Pillastrini P, Mugnai R, Bonfiglioli R, Curti S, Mattioli S, Maioli MG et al. Evaluation of an occupational therapy program for patients with Spinal Cord Injury. Spinal Cord 2008; 46: 78–81.
Whiteneck G, Meade MA, Dijkers M, Tate DG, Bushnik T, Forchheimer MB . Environmental factors and their role in partecipation and life satisfaction after spinal cord injury. Arch Phys Med Rehabil 2004; 85: 1793–1803.
Anneken V, Hanssen-Doose A, Hirschfeld S, Thietje R . Influence of physical exercise on quality of life in individuals with spinal cord injury. Spinal Cord 2010; 48: 393–399.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Appendix
Appendix
The GISEM group included the following investigators and centers: Ceravolo MG, Clinica di Neuroriabilitazione, Ancona; Nardulli R, Centro Medico Cassano Murge - IRCCS, Cassano Murge; Aito S, Unità Spinale CTO, Firenze; Cellotto N, Centro Riabilitazione ‘Villa Beretta’, Costamasnaga; Zucchi AG, Sezione Mielolesi, Magenta; Manera C, Unità Spinale Unipolare Osp. Niguarda, Milano; Bava A, Divisione Paraplegici CTO, Milano; Ghislandi I, SRRF Ospedale di Bergamo – Sez. Mozzo, Mozzo; Ortolani M, Servizio di Riabilitazione Ortopedica, Padova; Taricco MA, Ospedale Casati, Passirana di Rho; Pistarini C, Centro Medico Montescano, Pavia; Mosetti A, Ospedale Villa Rosa - CRF, Pergine Valsugana; Pagliacci MC, Unità Spinale Unipolare Osp. Silvestrini, Perugia; Gatta G, SRRF Ospedale S. M. delle Croci, Ravenna; Scivoletto G, IRCCS Santa Lucia, Roma; Trigila A, Unità Spinale Unipolare CTO, Roma; Occhi E, Unità Spinale, Sondalo; Loria D, Unità Spinale, Torino; Zampolini M, U.O. di Riabilitazione Intensiva Neuromotoria, Trevi; Di Benedetto P, Centro di Riabilitazione, Trieste; Cordioli Z, Reparto di RRF Ospedale Sacro Cuore - Don Calabria - Negrar, Verona; Leucci M, UORRF Unità Spinale Osp. S. Bartolo, Vicenza; Lotta S, Centro di R.R.F., Villanova d'Arda; Strazzabosco C, Istituto Riabilitazione Neuromotoria, Mezzaselva di Roana.
Rights and permissions
About this article
Cite this article
Franceschini, M., Pagliacci, M., Russo, T. et al. Occurrence and predictors of employment after traumatic spinal cord injury: the GISEM Study. Spinal Cord 50, 238–242 (2012). https://doi.org/10.1038/sc.2011.131
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.131
Keywords
This article is cited by
-
Return to work after traumatic spinal fractures and spinal cord injuries: a retrospective cohort study
Scientific Reports (2023)
-
Spinal cord injury and work challenges: an analysis of paid work status and pathways of return to work in Brazil
Spinal Cord (2021)
-
Promoting factors and barriers to participation in working life for people with spinal cord injury
Journal of Occupational Medicine and Toxicology (2020)
-
Relationships between type of pain and work participation in people with long-standing spinal cord injury: results from a cross-sectional study
Spinal Cord (2018)
-
Return-to-work intentions during spinal cord injury rehabilitation: an audit of employment outcomes
Spinal Cord (2016)
