
Abstract
Study design:
Prospective study.
Objectives:
To assess and quantify Rossolimo reflexes using an electrophysiological test, and correlate the findings with the severity of spinal cord dysfunction in cervical and thoracic spondylotic myelopathy (CTSM).
Setting:
A university neurorehabilitation center.
Methods:
We enlisted 42 patients with CTSM between the fifth cervical and the ninth thoracic cord levels. Using electrophysiological assessments, Rossolimo reflexes were evaluated in all patients. Conduction latencies and amplitude of muscle action potentials (MAPs) of the reflexes were measured, analyzed and compared with the grading of spinal cord dysfunction and the cord compression ratios.
Results:
We found a high diagnostic sensitivity of quantified Rossolimo reflex in patients with CTSM. A positive correlation exists between the MAP amplitude of Rossolimo reflexes and the different grades of spinal cord dysfunction. A negative linear relationship was found between the MAP amplitude of Rossolimo reflexes and the cord compression ratios in CTSM patients.
Conclusion:
Rossolimo reflexes can be measured by electrophysiological assessments, and we demonstrate a quantification method for an established neurological sign. Not only is the Rossolimo reflex found to be a highly sensitive test in clinical neurological examination but the electrophysiological assessment for this reflex can also serve as an objective marker for evaluation of the severity of spinal cord dysfunction in CTSM.
Similar content being viewed by others


Introduction
The Rossolimo reflex is flexion of the toes responding to tapping or flicking the tips of the underside of the toes.1 Its synonyms are plantar muscle reflex and Rossolimo sign, which have been described as tapping of the plantar surface from the second to fifth toes and causing flexion of toes.2 Named after the Russian neurologist,3 Grigorii Ivanovich Rossolimo (1860–1928), the Rossolimo reflex is commonly used for neurological examinations for upper motor neuron lesions and has been recognized as a sign for pyramidal tract lesions.
Conventional studies of Rossolimo reflexes describe the presence or absence of this response and show a range of assessments in percentage of appearance,4 although the stimulation for eliciting this response cannot be standardized or quantified. However, we hypothesize that this reflex could be measured and quantified by electrophysiological assessments. Therefore, this study aims to evaluate and quantify Rossolimo reflexes by an electrophysiological test, and correlate it with the severity of spinal cord dysfunction in patients with cervical and thoracic spondylotic myelopathy (CTSM).
Materials and methods
Subjects
For this study, we enlisted 42 patients with a clinical diagnosis of CTSM. These patients included 27 men and 15 women with a mean age of 61.3 years (range 52–74) years. A total of 30 age-matched healthy individuals recruited from patient spouses served as controls. Clinical diagnostic criteria for CTSM included sensory impairments, muscular weakness and associated hyper-reflexia in upper and lower extremities. Each patient underwent routine spinal roentgenography and magnetic resonance imaging examinations of the cervical and thoracic spinal canals. The radiological findings, accompanied by the clinical signs and features of cord compression, made the diagnosis of CTSM. The etiologies of spinal cord compression included degenerative changes in the inter-vertebral discs, osteophyte formation of the vertebral bodies, hypertrophied facets and laminal arches, hypertrophied posterior longitudinal ligament, buckling ligmentum flavum, spinal subluxation and stenosis. Durations of their disease from the onset of myelopathic symptoms to electrophysiological evaluation ranged between 3 months and 2 years. The neurological lesion levels in these patients were between the fifth cervical and the ninth thoracic cords. Cord compression ratios were measured in all patients. The cord compression ratio was defined as the antero-posterior diameter divided by the transverse diameter of the cord measured in magnetic resonance image at the most prominent compressed cord level. In addition, we categorized spinal cord dysfunction of CTSM patients into three grades, as listed in Table 1. We then graded patients according to the evaluating signs of cord involvement, ambulation and degree of dependence in activities of daily living, as modified from Nurick's Functional Scales for cervical spondylotic myelopathy.5
All CTSM patients were recruited by the same physician at random from neurorehabilitation clinics. They were then referred to the neurophysiological laboratory of a university teaching hospital for electrophysiological assessments during the period from October 2008 through December 2009. By exclusion, no patient had any history of foot deformity, toe joint contracture, tibial neuropathy, lumbosacral radiculopathy, diabetes mellitus or uremia. We also excluded other spinal cord lesion causes, such as trauma, infection, collagen diseases or malignant disease with spinal metastasis. During the study, no medication, such as anti-spasmodic or anti-convulsive drugs was given.
This study was approved by the university ethics committee in accordance with the international ethical standards of the 1964 Declaration of Helsinki. All patients accepted an informed consent before the study.
Quantification of Rossolimo reflexes
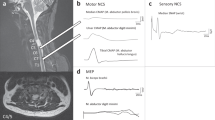
We assessed CTSM patients and controls in supine position and relaxed condition with eyes gently closed and slight flexion of the knees. In this way, we could minimize the actual motivational and emotional stress. Rossolimo reflexes were performed with a reflex hammer containing a built-in switch (Patella Hammer, Medelec, Surrey, UK), which was connected to an EMG machine signal trigger (Synergy System, Medelec, Surrey, UK). To elicit the reflexes, we applied the hammer for tapping on the plantar surface of skin on the second metatarso-phalangeal joint. An estimate of the skin area touched was 0.5 cm2, and the tapping force was 1.2 N measured by a digital force indicator (CentorT Star, Com-Ten Industries, Pinellas Park, FL, USA). We then placed the recording electrodes (Neuroline710, Ambu Medicotest, Olsykke, Denmark) on the flexor digitorum brevis muscle with a standard belly-tendon method, and placed the grounding electrode on the medial aspect of ankle (Figure 1). Each Rossolimo reflex was tested six times. To minimize the habitual reaction of the reflex, we allowed an interval of 15 s between trials. We then recorded the shortest onset conduction latency and the maximum peak-to-peak amplitude of muscle action potentials (MAPs). An example of the test is shown in Figure 2. During electrophysiological tests, the room temperature was controlled between 23 and 25 °C. Skin temperature of the foot was kept constant above 30 °C, with assistance of an infrared lamp if necessary.

Test of the Rossolimo reflex with a reflex hammer. Ra, active recording electrode; Rr, reference recording electrode; G, ground electrode.

Example of the Rossolimo reflex elicited in a patient with cervical spondylotic myelopathy. The shortest conduction latency was 52.4 ms, and the maximum amplitude of muscle action potential was 600 μV. St, stimulation.
Statistical analyses
We performed statistical analyses for comparing data among patient groups using the Kruskal–Wallis tests. The relationship between the MAP amplitude of Rossolimo reflexes and the grades of spinal cord dysfunctions, and that between the MAP amplitude of Rossolimo reflexes and the cord compression ratios in CTSM patients were analyzed with Pearson's correlation tests. Significance level was set at 0.05. All statistical analyses were performed with SPSS version 15.0 (SPSS Inc., Chicago, IL, USA) for Windows.
Results
Table 2 shows the cord compression ratios measured in CTSM patients and the results of Rossolimo reflex studies in all subjects. As can be seen, the appearance rate of Rossolimo reflexes elicited by manual tests was 85.7% (36 out of 42) in the patients. However, Rossolimo reflexes elicited by electrophysiological tests appeared in all CTSM patients. No Rossolimo reflex appeared in controls. Mean cord compression ratios showed a significant difference among the three grading groups of CTSM patients (P=0.012, Kruskal–Wallis test). In a correlation study of reflexes and cord compression ratios, we found a negative linear relationship (Figure 3) between the MAP amplitude of Rossolimo reflexes and the cord compression ratios in CTSM patients (R2=0.2235, P=0.017, Pearson's correlation test). Patients with increased MAP amplitude of Rossolimo reflexes tend to have more serious spinal cord compression in CTSM.

Correlation of cord compression ratios with the muscle action potential (MAP) amplitudes of the Rossolimo reflexes in patients with cervical and thoracic spondylotic myelopathy (CTSM).
In electrophysiological studies of Rossolimo reflexes, there were no significant differences in conduction latencies obtained from the patient groups with different grades of spinal cord dysfunction (P=0.451). However, the MAP amplitude showed a prominent difference among the three groups of CTSM patients (P=0.023). Grade III patients showed a greater MAP amplitude than did grade I patients (P=0.002) and grade II patients (P=0.026). We found a positive relationship between the MAP amplitude and the grading of spinal cord dysfunction (P=0.005, Pearson's correlation test). Patients with increased MAP amplitude of Rossolimo reflexes tend to have more serious spinal cord dysfunction in CTSM.
Discussion
Physiologically, the Rossolimo reflex is a stretch reflex response of the toe flexor,6 which is when a sensory input comes from the tendon stretch. It may elicit a monosynaptic stretch reflex in Rexed lamina IX of the spinal cord7 and coupling of muscles to the other toe flexors. This focal stretch response does not appear in normal adults because the excitabilities of spinal motoneurons are fully suppressed by the descending influence of supra-spinal pathways. However, this response may be activated and mediated through changes in spinal cord or cortico-spinal tract lesions of the spinal reflex circuits. According to the findings of Hiersemenzel et al.8 and Nielsen et al.9 on the pathophysiology of spinal cord injury, adaptational changes in excitability were found in the spinal neuronal circuits caudal to the spinal cord lesion. Great motoneurons are initially activated because of disturbed interaction of inhibitory and excitatory mechanisms on segmental levels. During the transition of spinal shock to spasticity, the reappearance of tendon reflex and muscle tone was associated with the recovery of spinal reflex and motor neuron excitability. This is the possible cause that the H/M (Hoffmann reflex amplitude to MAP amplitude) ratio may reach its maximum at 8 weeks after spinal cord injury and remains stable thereafter.8 At a later stage in 8 weeks after spinal cord injury when clinical signs of spasticity became established, the electrophysiological measures showed little change.8 Therefore, it was always necessary to examine the Rossolimo reflex in CTSM patients who were having spinal cord dysfunction at least 2 months after the onset of the disease.
The compression ratio of spinal cord has been recognized as a strong indicator of spinal cord dysfunction10 and served as a criterion for surgical treatment for cervical spondylotic myelopathy.11 This study shows a positive correlation between MAP amplitude of Rossolimo reflexes and functional grading of spinal cord. A linear relationship is also found between the MAP amplitude of the reflexes and the cord compression ratios of the patients. These findings strongly indicate that MAP amplitudes of Rossolimo reflexes are indicative of the severities of spinal cord dysfunction. Physiologically, increasing neuron excitability may be associated with increasing numbers of disinhibited motoneurons from central controls in the progression of spinal cord dysfunction in CTSM. Thus, an increase in activating neurons and their axonal fibers may lead to an increase in MAP amplitude in the reflex responses. In spite of the findings in MAP amplitude, we found no difference in conduction latencies of Rossolimo reflexes among patient groups. This finding suggests that the fastest nerve conductive fibers in the reflex arcs exist in CTSM. Theoretically, different degrees of spinal cord lesions may affect different proportions of excited motoneurons below the cord lesion and change the MAP amplitude through the reflex responses. However, no peripheral nerve pathology occurred caudal to the spinal cord lesion. The short latency responses for stretch reflexes should be not affected,12 and their nerve conduction in the reflex arcs could still be intact.
In the literature, there is little information on the ability of the Rossolimo reflex to predict spinal cord compression. In this study, we showed that the Rossolimo reflex has a high diagnostic sensitivity for neurological examination of CTSM patients. However, as we did not investigate the specificity of the Rossolimo reflex for differential diagnosis of other diseases of the spinal cord, this area requires further exploration.
In conclusion, Rossolimo reflexes can be measured by electrophysiological assessments, and we demonstrate a new quantification method for an established neurological sign. Not only is the Rossolimo reflex a highly sensitive test in clinical neurological examination but the electrophysiological assessment for this sign can also serve as a sensitive marker for evaluation of the severity of spinal cord dysfunction in CTSM.
References
Campbell WW, DeJong RN, Haerer AF . DeJong's the Neurologic Examination, 6th edn. Lippincott Williams & Wilkins: Philadelphia, 2005, p 493.
Firkin BG, Whitworth JA . Dictionary of Medical Eponyms, 2nd edn. Taylor & Francis: London, 2001, p 347.
Satran R . Chekhov and Rossolimo, careers in medicine and neurology in Russia 100 years ago. Neurology 2005; 64: 121–127.
Madonick MJ . Statistical control studies in neurology, X. relationship between frequencies of reflexes in a group of 2500 non-neurological patients: Babinski, Hoffmann, Rossolimo, Oppenheim, Gordon and absent cutaneous abdominal reflexes. J Nerv Ment Dis 1960; 131: 547–549.
Nurick S . The natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain 1972; 95: 87–100.
Shahani BT, Young RR . Human flexor reflexes. J Neurol Neurosurg Psychiatry 1971; 34: 616–627.
Harrop JS, Hanna A, Silva MT, Sharan A . Neurological manifestations of cervical spondylosis: an overview of signs, symptoms, and pathophysiology. Neurosurgery 2007; 60: S14–S20.
Hiersemenzel LP, Curt A, Dietz V . From spinal shock to spasticity: neuronal adaptations to a spinal cord injury. Neurology 2000; 54: 1574–1582.
Nielsen JB, Crone C, Hultborn H . The spinal pathophysiology of spasticity-from a basic science point of view. Acta Physiol (Oxf) 2007; 189: 171–180.
Harrop JS, Naroji S, Maltenfort M, Anderson DG, Albert T, Ratliff JK et al. Cervical myelopathy: a clinical and radiographic evaluation and correlation to cervical spondylotic myelopathy. Spine 2010 (e-pub ahead of print 10 February 2010).
Law Jr MD, Bernhardt M, White III AA . Cervical spondylotic myelopathy: a review of surgical indication and decision making. Yale J Biol Med 1993; 66: 165–177.
Toft E, Sinkjaer T, Espersen GT . Quantitation of the stretch reflex, technical procedures and clinical applications. Acta Neurol Scand 1989; 79: 384–389.
Acknowledgements
We are grateful to Kai-Fong Chang for his technical assistance on the MR imaging of the spinal cords.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Chang, CW., Chang, KY. & Lin, SM. Quantification of Rossolimo reflexes: A sensitive marker for spondylotic myelopathy. Spinal Cord 49, 211–214 (2011). https://doi.org/10.1038/sc.2010.81
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.81
