
Abstract
Background/objectives
To determine the role of vitreoretinal surgery (VRS) for two different forms of posterior persistent fetal vasculature syndrome (PFVS); with tent-shaped tractional retinal detachment (TRD) and closed funnel-shaped TRD.
Subjects/methods
Retrospective, single surgeon, consecutive case series of 52 eyes of 44 patients with posterior PFVS who underwent VRS. Cases were divided into “tent-shaped TRD” and “funnel-shaped TRD” groups based on the preoperative TRD configuration. Associated anomalies, functional and anatomical outcomes were evaluated. The cosmetic appearance was defined as poor if there was phthisis bulbi, gross buphthalmos, or corneal opacification; acceptable if there was apparent leukocoria; and excellent if none were noted at the last follow-up.
Results
Thirty eyes of 29 patients presented with tent-shaped TRD; 70% of which obtained counting fingers or better vision and 90% showed significant reversal of tenting achieving retinal reattachment. The cosmetic appearance was excellent in 87%. Two eyes (7%) became phthisic. Twenty-two eyes of 15 patients presented with funnel-shaped TRD and leukocoria; 45% achieved LP vision and 70% of patients with bilateral pathology had LP in at least one eye. The cosmetic appearance was acceptable to excellent in 73%. Three eyes (14%) became phthisic, one (5%) of which required enucleation. The median follow-up time was 16 (6–71) months.
Conclusions
VRS often provides functional vision and anatomy in posterior PFVS with tent-shaped TRD morphology. In the funnel-shaped TRD morphology, where no treatment has historically been recommended, surgery may be considered with an aim of restoring light perception and globe preservation, particularly in bilateral cases.
Similar content being viewed by others


Introduction
Persistent fetal vasculature (PFV), previously known as persistent hyperplastic primary vitreous, is a rare congenital developmental abnormality caused by failure of involution of the primary vitreous and hyaloid vasculature [1]. PFV represents a wide spectrum of disease, ranging from minimal abnormalities at the optic nerve or crystalline lens to a completely disorganized globe. Traditionally, the disease is divided into anterior, posterior and combined forms, based on the affected intraocular structures. Anterior form may include the presence of microphthalmia, retrolental fibrovascular membrane, cataract, and elongated ciliary processes with or without a hyaloidal stalk, whereas, posterior form may consist of vitreous membrane and stalk, retinal folds, tractional retinal detachment (TRD), closed-funnel RD and hypoplastic optic nerve and macula. Nevertheless, most cases exhibit features of both and variety of presentations makes PFV management challenging. Except for mild forms, the natural disease course of PFV is characterized by progression of fibrovascular dysplasia leading to anterior chamber shallowing, angle-closure glaucoma leading to buphthalmia, iridocorneal apposition leading to corneal opacification, intraocular hemorrhage, painful red eye and phthisis bulbi [1, 2]. This dismal natural history has largely been changed with surgery after the advances in surgical techniques and instrumentation, as well as earlier diagnosis and aggressive amblyopia therapy. Reattachment rates of up to 77–91% have been reported in recent studies with the use of modern surgical techniques for PFV-related TRD [3,4,5,6]. However, these studies mostly included selected cases of posterior PFV that is in the milder to moderate end of the spectrum. Eyes with more severe form of posterior disease and severe retinal dysplasia, on the other hand, are still considered as poor surgical candidates with little or no visual potential and have not been studied to date. We hypothesize that surgical intervention might provide at least cosmetically acceptable globe and/or light perception (LP) vision in severe cases, which may be particularly important in bilateral cases. Accordingly, we reviewed the surgical results of PFV cases with different degrees of posterior involvement and sought an answer to the question of whether we should expand the surgical indications for patients at the most severe end of the disease spectrum or not.
Methods
We undertook a retrospective record review of all consecutive PFV patients with posterior involvement who underwent surgery by a single surgeon (SO) between January 2010 and December 2020 after obtaining an informed consent. The study followed the principles of the Declaration of Helsinki and was approved by the local institutional ethics committee.
Diagnosis was based on a combination of clinical examination, examination under general anesthesia, and ultrasonography findings. As Goldberg [1] described, cases with TRD and folds associated with persistent foetal hyaloid remnants were named as posterior PFV. Of these, patients with a positive family history or genetic testing consistent with Norrie disease, familial exudative vitreoretinopathy, trisomy 13, trisomy 18, or Walker-Warburg syndrome were excluded from the study. Considering the possible different implications for prognosis and management, cases were divided into two groups based on the preoperative TRD configuration and severity: “tent-shaped” and “closed-funnel-shaped”. The main differentiating feature between the tent-shaped and closed-funnel-shaped configurations was the presence of attached retina to some extent in the periphery in the tent-shaped type. Then the following information was recorded for each case: Age at time of diagnosis and surgery, sex, presenting complaint, associated systemic and ocular abnormalities, surgical procedure(s) performed, complications, anatomical and functional outcomes, and the length of follow-up.
Surgical technique
All patients underwent 3–port vitrectomy, with or without lensectomy, through a limbal or pars plana/plicata approach. Two different surgical approaches were adopted depending on the posterior PFV subtype.
For tent-shaped TRD, pars plana/plicata entry was preferred to perform lens-sparing vitrectomy (LSV) if anterior segment involvement was limited and peripheral retina could be visualized for possible anomalies. Surgical technique mainly involved transection of the fibrovascular stalk behind the lens and meticulous dissection of retrolental and preretinal membranes to relieve tractions on the retina. In cases of LSV, an attempt to completely clear the hyaloid tissue from the posterior capsule was avoided so as not to induce opacification of the lens, since the attachment site of the tissue on the posterior capsule is inherently weak, or sometimes fused with fetal tissue. Instead, after transecting the stalk, the anterior portion of the tissue was shortened as much as possible and only peeled off the surface if it could be easily released. Otherwise, it was left in place to contract over time. Lensectomy was performed if the lens opacity was clinically significant. If the lens opacity prevented visualization of the peripheral retina, a limbal entry was planned as done for funnel-shaped TRD cases.
For closed funnel-shaped TRD, which is usually associated with cataract or retrolental opacities blocking adequate visualization of the anterior retina, entries were made through the iris root or limbus. Synechiolysis of iridocorneolenticular adhesions (if present), use of iris hooks or partial iridectomy were often required to create an adequately wide pupil for surgery. Total lensectomy including capsules was followed by bimanual dissection of retrolental and preretinal membranes using microforceps and microscissors. Multiple sheets of membranes had to be dissected layer by layer, from the center to the periphery and from the anterior to the posterior, until the funnel was opened-up to reach the posterior pole when possible. Membrane dissection was done very cautiously to avoid breaks in the dysplastic retina and continued as long as the surgeon felt safe. Anterior peripheral dissection behind iris was often impossible and left incomplete. Ocular viscoelastics were used in some cases to open the funnel more following dissection. Eye was left in air at the end of most cases.
Postoperative care and evaluations
Postoperatively, patients received optical correction (soft contact lens of appropriate power/glasses) as soon as possible. Amblyopia therapy was recommended based on a subjective prediction of future visual potential and involved patching the better eye for several waking hours every day. All patients underwent periodic examinations including evaluation of visual acuity (VA), intraocular pressure, and anterior and posterior segment findings.
VA was assessed with age-appropriate tests such as the Teller and Snellen-equivalent methods. In younger patients for whom acuity testing was not possible, fixation patterns were recorded and extrapolated to VA measurements using a previously described method modified from that of Zipf [7]: >20/30 if CSM, 20/30–20/100 if CSUM, <20/300 if CUSUM, and <5/200 if UCUSUM present where C indicates central; S, steady; M, maintained; US, unsteady; UM, unmaintained; UC, uncentral. Globe preservation was assessed from the point of anatomical and cosmetic preservation. Anatomical preservation was defined as preservation of the globe in place without any painful, red, tearing eye development necessitating removal. Cosmetic result was poor if phthisis bulbi, gross buphthalmos or corneal opacification were noted, acceptable if apparent leukocoria was present, and excellent if none of these were noted at the last follow-up.
Statistical analysis
Statistical analyses were performed with IBM SPSS Statistics v22.0 and statistical significance was set as 2-tailed p value < 0.05. Continuous data was tested for normality using the Shapiro–Wilk test. The Mann–Whitney U test, Chi-square and Fisher’s exact tests were used to compare clinical characteristics and outcomes, where appropriate.
Results
Chart review revealed 44 patients with posterior PFV who underwent surgery. Thirty-one (70.4%) had unilateral and thirteen (29.5%) had bilateral disease. Of the bilateral cases, 8 had bilateral and 5 had unilateral surgery. As a result, a total of 52 operated eyes were included in the study. The median age at surgery was 5 (2–48) months. The median length of follow-up was 16 (6–71) months.
The first group included 30 eyes of 29 patients with tent-shaped TRD and the second group included 22 eyes of 15 patients with funnel-shaped TRD.
PFV with tent-shaped TRD
Thirty eyes of 29 patients presented with persistent hyaloidal stalk causing tent-shaped or dome-like TRD involving the peripapillary and macular region. Twenty-six patients (90%) had unilateral; three (10%) had bilateral disease. Two patients with bilateral pathology had disorganized globes with severe microcornea and microphthalmia in their fellow eyes, judged to be inoperable (these eyes were not included in the study).
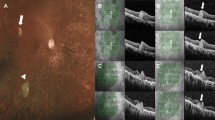
LSV was performed in 13 eyes (43%) where the anterior attachment of the stalk formed a small eccentric opacity behind the lens, allowing visualization of the posterior segment (Fig. 1). Combined lensectomy—vitrectomy (LV) was performed in 17 eyes (57%) with significant anterior segment involvement (i.e., combined PFV) such as larger and/or axial lens opacification, or dense retrolental fibrovascular plaque extending to the peripheral lens capsule. Limbal entries were used in 12 eyes (40%). These included cases with severe anterior segment involvement such as a central and clinically significant lens opacity, broad posterior synechiae and extensive pupillary membrane. Limbal route was preferred in the aforementioned group since the peripheral retina could not be checked for possible anomalies/elongations for the secure pars plana/plicata entry. Pars plana route was used in the remaining 18 eyes (60%). One patient (15-month-old) had a three-piece intraocular lens placed in the sulcus at the time of surgery.

After 5 years of follow-up, visual axis remained clear with a very small paracentral opacity at the back of the lens and the visual acuity was 20/100. Color fundus and optical coherence tomography images show complete flattening of the retina with residual fibrosis at the optic nerve head (bottom row).
Microphthalmia was present in 18 (60%) of the eyes. Median corneal diameter was 9.75 (7.5–11.5) mm. Other findings included colobomatous disc and/or macula (n = 5, 17%) and anterior segment dysgenesis (n = 1). There were peripheral retina-ciliary body abnormalities in 27% of the eyes. We often observed finger-like projections of the peripheral retina, extending beyond an anteriorly-displaced ora serrata. In some cases, peripheral retina more extensively replaced pars plana and directly inserted onto the retrolental fibrovascular tissue. In one of such cases, a retinal tear occurred during an attempt to separate peripheral remnants of retrolental tissue from the anteriorly elongated retina. This eye progressed to phthisis bulbi despite two vitreoretinal surgeries. No other intraoperative complication was noted.
Functional results
Twenty-one eyes (70%) had counting fingers or better vision at the last follow-up. Ten (33%) had 20/200 or better VA measured with Snellen-equivalent methods or fixation patterns. Eleven eyes (37%) had a VA of <20/300 to counting finger vision inclusively. Four eyes (13%) had LP, two of which had colobomatous optic nerve head/macula defects. No light perception (NLP) was noted in 5 eyes (17%) that were either complicated or had severe retinal dysplasia. The median age at surgery was 9 (2–48) months in patients achieving 20/200 or better vision; and it was 5 (2–11) months for those having VA worse than 20/200 (p = 0.27).
Anatomical results
Twenty-seven eyes (90%) showed significant reversal of retinal dragging postoperatively; complete macular reattachment was obtained in all except two cases with persistent macular folds. In one of the bilateral cases whose fellow eye was inoperable, the retina failed to reattach in the operated eye. This eye was in the more severe end of the tent-shaped TRD spectrum; the dense retrolental fibrovascular membrane dragged the entire retina anteriorly and accompanied by significant cataract and corneal leukoma. Although the convexity of detachment relatively decreased and the retina moved slightly posteriorly after surgery, near-total RD persisted. Progressive corneal opacification made examinations difficult, and NLP was noted at 6-month follow-up. Another case who underwent bilateral LSV developed total RD in one eye 2 months after surgery. This eye had a thicker fibrovascular stalk that caused more severe tenting of the retina compared to the fellow eye and resulted in phthisis bulbi. Glaucoma developed in 3 eyes (10%); one was controlled with topical antiglaucoma medication, and two required surgeries. Of the 13 eyes who underwent LSV, only one (8%) developed significant cataract requiring surgery 2.5 years after the primary surgery.
Cosmetic results
Cosmetic appearance was excellent in 26 eyes (87%) based on the criteria employed. The remaining 4 eyes (13%) had poor cosmesis at the last follow-up; one (3%) had opaque cornea, one (3%) had buphthalmia, and the other two (7%) were phthisic. The phthisic eyes were stable and fitted with overlying prostheses.
PFV with closed funnel-shaped TRD
Twenty-two eyes of 15 patients presented with leukocoric pupils associated with total TRD with closed-funnel configuration. Five patients (33%) had unilateral and 10 (67%) had bilateral disease. Three of the patients with bilateral pathology underwent unilateral surgery. One was due to parents’ decision not to have the other eye operated, and the other two were severely microphthalmic eyes, one of which also had sclerocornea, and deemed inoperable (these eyes were not included in the study).
All patients in this group were born full-term and had a negative family history of retinal disease. Ocular examination of parents and siblings, performed when possible, was unremarkable. Male patients with bilateral disease were subjected to genetic testing to rule out Norrie disease, all of which tested negative for NDP mutations.
Microphthalmia was the most prominent finding, affecting 86% (n = 19) of the eyes. Median corneal diameter was 8.75 (8–12.5) mm. One eye had buphthalmos. Presence of a fixed irregular pupil with broad synechiae and a shallow chamber was common and found in 64% (n = 14) of the eyes. Nine (41%) of them presented with corneal opacity associated with irido-corneo-lenticular adhesions.
Functional results
Overall, 10 eyes (45%) achieved LP vision. This corresponded to 70% of the patients with bilateral pathology who obtained LP in at least one eye.
Anatomical results
All eyes in this group had limbal LV surgery. Synechiolysis often provided sufficient corneal clearance for vitrectomy in eyes with preexisting corneal opacity except for 3 eyes (14%) in which the surgery had to be terminated prematurely. These eyes had total RD at the pupillary plane causing leukocoria and NLP at the last follow-up; but none of them developed phthisis or further corneal opacification.
In 13 of the remaining eyes (59% of all), the funnel could be opened with efficient membrane dissection and release of tractions (Fig. 2). Postoperatively, 3 eyes (14%) achieved partial posterior polar reattachment with localized areas of retinal folds outside the macula, which was the best outcome in this group (Fig. 2b). Another eye continued to have total RD, which gradually settled and became very shallow over time (Fig. 2a). Five eyes (23%) had more elevated detachment with anterior open posterior closed-funnel configuration at final follow-up, but apparent leukocoria resolved in all with the receded retina and LP vision was noted in all except one. Despite efficient release of tractions on the retina, four eyes (18%) had poorer prognosis due to complications. Two of these had iatrogenic retinal breaks during peripheral dissection of the retrolental membranes and became phthisic during follow-up. One developed a late posterior retinal break 2 months after surgery and resulted in inoperable PVR-RD and NLP. The other one had severely dysplastic retina that showed membrane proliferation and worsening of detachment in the postoperative period. A possible missed retinal break formation was considered in the aetiology as in the former case, although not documented.

Case 1 (a) Surgical images of a patient with severe closed-funnel posterior PFV. Leukocoric pupil with synechiae, elongated ciliary processes, and layer by layer removal of membranes are demonstrated. Wide opening of the funnel was possible with painstaking dissection of membranes in both eyes. Dysplastic retina remained detached but receded and became shallow over time. Patient achieved light perception vision. Case 2 (b) Surgical images of another patient with severe closed-funnel posterior PFV. Step by step removal of the membranes, transection of the fibrovascular stalk and opening of the funnel are demonstrated. Retina was partially attached at the final follow-up and light perception vision was maintained.
In the remaining 6 eyes (27% of all), opening of the funnel was very limited or not possible at all. One of them had a rigid fibrovascular membrane that could only be partially removed. In others, the membranes were so firm that they allowed only limited dissection along the plateau of the retina, not into the funnel. Among these eyes, only one developed phthisis bulbi.
Cosmetic results
Cosmetic appearance was excellent in 9 eyes (41%); and acceptable in the additional 7 (32%) eyes based on the criteria employed (Fig. 3). Six eyes (27%) had poor cosmesis at the last follow-up; three (9%) had opaque corneas, one of which was buphthalmic; and the other 3 (13.6%) were phthisic. One of the phthisic eyes was enucleated after becoming painful. The other two were stable and fitted with overlying prostheses.

B-scan ultrasonography revealed a closed-funnel retinal detachment. Note the large central corneal opacification (a) secondary to irido-lenticulo-corneal adhesions, which was significantly reversed after lensectomy and synechiolysis done for cosmesis. b Picture taken 6 months after the operation shows a central leukocoria with very mild corneal oedema in the left eye. The parents were very satisfied with the cosmetic result.
Membrane dissection and opening the funnel was more difficult in cases with severe corneal pathology at presentation. Compared to the eyes with clear cornea, these eyes more often resulted in NLP (67% vs. 46%) and poor cosmesis (44% vs. 15%); however, the differences were not statistically significant (p = 0.34, p = 0.13, respectively). Surgical age and corneal diameter did not have any effect on cosmetic results (p = 0.40, p = 0.21, respectively) or LP recovery (p = 0.97, p = 0.53, respectively).
Comparisons between two groups
Tent-shaped TRD group most often presented with strabismus (63%), while the most common presenting complaint was leukocoria (59%), followed by microphthalmia (32%) in the funnel-shaped TRD group. When compared to the tent-shaped TRD cases, funnel-shaped TRD cases were diagnosed significantly earlier (2.5 vs. 5.5 months), and they were more likely to have bilateral pathology, microphthalmia, anterior segment involvement, shallow anterior chamber, and corneal opacity (Table 1). Postoperatively, cosmetic appearance was excellent in 87% of the tent-shaped group; acceptable to excellent in a total of 73% of the funnel-shaped group. LP vision was the best functional outcome in funnel-shaped TRD group and was achieved in 45% of the cases. In contrast, 70% of cases with tent-shaped TRD achieved counting fingers or better vision (Table 2).
Discussion
There have been many articles on surgical management of the PFV [3, 4, 6, 8,9,10,11]. Early literature suggested that posterior PFV forms were associated inevitably with poor outcomes and many cases were considered as exclusion criteria for surgical treatment. However, recent studies herald improved outcomes as surgical techniques and disease knowledge have advanced over years. Today, we have come to a point where we can offer treatment to many mild to moderate forms of posterior PFV and expect satisfactory results. In this report, we aimed to discuss whether it is possible to take this point one step further in the light of evidence.
We examined two different retinal detachment patterns that we believe should be considered separately in posterior PFV. Tent-shaped morphology, which is the typical and most common presentation of the posterior disease, was well-defined and frequently reported in the literature. Anatomical and functional results in this group were comparable to the results of previous studies [3,4,5,6], with 90% of the eyes achieving complete or near-complete retinal reattachment and 70% obtaining counting fingers or better vision. In contrast to the previous data by several authors [5, 6, 8], younger surgical age did not correlate with better visual results in our series, which is probably attributable to the heterogeneity of disease severity across studies. We observed the best visual outcome in an eye with mild form operated at the age of 4 years, and the worst outcomes in the presence of optic nerve/macula pathologies and dysplasia. Therefore, although earlier intervention is the only changeable factor to maximize these eyes’ potential, the potential itself appears to be determined mainly by the severity of the posterior disease. Our observations indicate that a specific group of tent-shaped cases with eccentric stalks (as in Fig. 1) have by far the best prognosis among the posterior PFV spectrum where the lens is not significantly affected and a LSV could end up with very good visual results.
Another point worth attention is the unexpectedly high prevalence of peripheral retinal anomalies; more than one-quarter had abnormal retinal insertion directly onto the pars plicata or retrolental membrane. In a previous study, we reported that peripheral retinal elongations were even more common in anterior PFV cases, up to 82% [12]. The elongated retinal tissue may be damaged during sclerotomy or excision of the retrolental membrane, resulting in rhegmatogenous RD. Hence, careful inspection of the ora-ciliary body region or use of limbal entries if the view is obstructed by an extensive fibrovascular membrane is necessary.
The second group included severe posterior PFV cases presenting with leukocoria and closed funnel-shaped TRD. To our knowledge, this rare phenotype has not been described in detail before. Literature research suggests that these cases were often enucleated with the concern of retinoblastoma or considered inoperable [2, 13,14,15]. Although natural course of untreated posterior disease has been associated with high rates of NLP vision, they likely underestimate the morbidity associated with closed-funnel variant, as this type was not explicitly addressed in the previous studies [2, 8, 10, 11, 13]. In our experience, we estimate that almost all eyes with closed funnel-shaped TRD at presentation deteriorate over time if left untreated, resulting in corneal opacification, glaucoma or phthisis bulbi. In recent years, we have expanded surgical indications for these cases to prevent these complications, and preserve the globe in an acceptable cosmesis, which was achieved in 73% of the closed-funnel TRD eyes.
Surgical success is directly related to removing as much tractional membranes as possible, without creating a rhegmatogenous component, and enabling the funnel opening. When a satisfactory dissection could be performed to open the funnel, the detached retina goes backwards from the pupillary plane to some extent during the postoperative 2–3 months period, allowing the resolution of apparent leukocoria. It is not expected to flatten the whole retina with one surgery; however, a staged surgical approach may be adopted to remove more membranes when retina settles back over time. In eyes with shallow anterior chamber, a lensectomy with synechiolysis may prevent further corneal opacification and even partially reverse preexisting opacities (Fig. 3). In this study, 64% of the cases had shallow anterior chamber and 41% had corneal opacity (irido-lenticulo-corneal adhesions) at presentation. None of these developed further corneal opacification after surgery. Moreover, leukocoria was resolved in 41% and nearly half of the eyes (45%) gained LP vision. Light perception is very important for diurnal rhythm of the body which regulates sleep-wake cycles as well as for better orientation of child to time and space. The functional result of surgery is even more pronounced in bilateral cases, with 70% of them having light perception in at least one eye.
In this study, the membranes causing the funnel configuration were relatively easier to dissect in 59% of the eyes, while they were more rigid and fibrotic, making dissections more difficult or even impossible in the remaining. Preoperative prediction of the nature of the membranes and the funnel opening potential may improve success and prevent unnecessary surgery. Presence of an opaque cornea might be important in this regard. Although not statistically significant, eyes with severe corneal opacity were more likely to result in limited or failed opening of the funnel, NLP and poor cosmesis, compared to the eyes with clear cornea. We did not find any correlation between the corneal diameter and the outcomes; however, all operated eyes had corneas of 8 mm or larger and outcomes may differ in eyes with smaller corneas.
This study has some limitations. Despite the relatively large sample size, severe posterior PFV is rare and the number of patients in the subgroups remained small. However, due to the rarity and heterogeneity of the disease, it is impractical to conduct a prospective controlled study with a larger cohort. Additionally, differential diagnosis from Norrie disease might be very challenging in severe funnel-shaped TRD cases. Given the overlap between diseases, one may argue that some patients may have Norrie disease since genetic testing was not available in all cases. However, this is unlikely in the absence of family history of blindness, deafness or mental retardation. Moreover, postoperative iris neovascularization and neovascular glaucoma, which are very common in Norrie disease, was not seen in any case.
In conclusion, this study corroborates the information published in earlier series on posterior PFV and, for the first time, demonstrates the characteristics and surgical outcomes of two distinct posterior PFV types, namely tent-shaped and closed funnel-shaped TRD. Vitreoretinal surgery (VRS) usually provides functional vision in the tent-shaped variant. Conversely, the closed-funnel variant may benefit from surgery in terms of having LP and a cosmetically acceptable globe and thereby become amenable to potential visual restorative technologies in the future.
Summary
What was known before
-
Severe posterior persistent foetal vasculature syndrome (PFVS) presenting with leukocoria and funnel-shaped retinal detachment has been considered inoperable in the previous literature.
-
Majority of the eyes with closed funnel-shaped TRD at presentation deteriorate over time if left untreated, resulting in corneal opacification, glaucoma, or phthisis bulbi.
What this study adds
-
VRS provided a cosmetically acceptable globe in three-quarters of the severe posterior PFVS eyes with funnel-shaped retinal detachment.
-
In this group, nearly half of the eyes gained light perception vision after vitreoretinal surgery.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Goldberg MF. Persistent fetal vasculature (PFV): An integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV) LIV Edward Jackson Memorial Lecture. Am J Ophthalmol. 1997;124:587–626.
Reese AB. Persistent hyperplastic primary vitreous. Am J Ophthalmol. 1955;40:317–31.
Karacorlu M, Hocaoglu M, Sayman Muslubas I, Arf S, Ersoz MG, Uysal O. Functional and anatomical outcomes following surgical management of persistent fetal vasculature: a single-center experience of 44 cases. Graefes Arch Clin Exp Ophthalmol. 2018;256:495–501.
Sisk RA, Berrocal AM, Feuer WJ, Murray TG. Visual and anatomic outcomes with or without surgery in persistent fetal vasculature. Ophthalmology. 2010;117:2178–83.
Bosjolie A, Ferrone P. Visual outcome in early vitrectomy for posterior persistent fetal vasculature associated with traction retinal detachment. Retina. 2015;35:570–6.
Hunt A, Rowe N, Lam A, Martin F. Outcomes in persistent hyperplastic primary vitreous. Br J Ophthalmol. 2005;89:859–63.
Zipf RF. Binocular fixation pattern. Arch Ophthalmol. 1976;94:401–5.
Walsh MK, Drenser KA, Capone A, Trese MT. Early vitrectomy effective for bilateral combined anterior and posterior persistent fetal vasculature syndrome. Retina. 2010;30:S2–8.
Alexandrakis G, Scott IU, Flynn HW, Murray TG, Feuer WJ. Visual acuity outcomes with and without surgery in patients with persistent fetal vasculature. Ophthalmology. 2000;107:1068–72.
Federman JL, Shields JA, Altman B, Koller H. The surgical and nonsurgical management of persistent hyperplastic prima vitreous. Ophthalmology. 1982;89:20–4.
Pollard ZF. Persistent hyperplastic primary vitreous: diagnosis, treatment and results. Trans Am Ophthalmological Soc. 1997;95:487–549.
Ozdek S, Ozdemir Zeydanli E, Atalay HT, Aktas Z. Anterior elongation of the retina in persistent fetal vasculature: emphasis on retinal complications. Eye. 2019;33:938–47.
Scuderi G, Balestrazzi E, Ranieri G. Destructive and conservative treatment of persistent hyperplastic primary vitreous and retinal dysplasia. Ophthalmologica. 1976;172:346–52.
Dawson DG, Gleiser J, Movaghar M, Patel SM, Albert DM. Persistent fetal vasculature. Arch Ophthalmol. 2003;121:1340–1.
Soheilian M, Vistamehr S, Rahmani B, Ahmadieh H, Azarmina M, Mashayekhi A, et al. Outcomes of surgical (pars plicata and limbal lensectomy, vitrectomy) and non-surgical management of persistent fetal vasculature (PFV): An analysis of 54 eyes. Eur J Ophthalmol. 2002;12:523–33.
Author information
Authors and Affiliations
Contributions
All co-authors of this work met all of the following criteria: Conceived and/or designed the work that led to the submission, acquired data, and/or played an important role in interpreting the results. Drafted or revised the manuscript. Approved the final version. Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ozdemir Zeydanli, E., Ozdek, S., Acar, B. et al. Surgical outcomes of posterior persistent fetal vasculature syndrome: cases with tent-shaped and closed funnel-shaped retinal detachment. Eye 37, 1371–1376 (2023). https://doi.org/10.1038/s41433-022-02140-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-02140-0
This article is cited by
-
Severe anterior persistent fetal vasculature: the role of anterior retinal elongation on prognosis
Graefe's Archive for Clinical and Experimental Ophthalmology (2023)
