
Abstract
Aim
To describe the changes in corneal graft thickness following ultrathin Descemet’s Stripping Automated Endothelial Keratoplasty (UT-DSAEK) comparing pre- and postoperative values over a 24-month period.
Methods
In this retrospective single-center case series, patients who received eye bank-prepared tissues for UT-DSAEK surgery were included. Preoperative and postoperative graft thickness measurements were determined in the eye bank and in clinic using anterior segment optical coherence tomography (AS-OCT) images. Graft thickness measurements and their percentage change between preoperative values and values at 1 day, 1 week and 1, 6, 12, 24 months were calculated.
Results
In total, 47 eyes of 47 patients with a mean age of 69 ± 11 years (29 males) were included. Twnty-three patients had Fuchs’ endothelial dystrophy (49%) and the remaining 24 had pseudophakic bullous keratopathy (51%). In total, 29/47 eyes underwent UT-DSAEK alone (62%) and 18/47 received combined cataract surgery as a triple procedure (38%). Preoperative donor graft thickness was 92 ± 28 μm. Compared to preoperative values, where graft thickness increased to 194 ± 101.3 μm at 1 day, 151.1 ± 71.4 μm at 1 week, and 108.4 ± 52.5 μm at 1 month. Graft thickness continued to gradually decrease over time until 6 months (91.7 ± 33.6 μm), and then plateaued at 12 months (83.9 ± 25.0 μm), showing minimal changes at 2 years (101.4 ± 37.5 μm).
Conclusion
Preoperative DSAEK graft thickness measurements as reported by the eye bank are a valid approximation of DSAEK graft thickness at 6 months after surgery and these measurements tend to stabilize over time up to 2 years after surgery.
Similar content being viewed by others


Introduction
Endothelial keratoplasty techniques started with the introduction by Melles of posterior lamellar keratoplasty in followed by Terry and Ousley’s deep lamellar endothelial keratoplasty (DLEK) in 2001 [1,2,3,4,5,6]. Improvement in interface architecture from DLEK to Descemet stripping automated endothelial keratoplasty (DSAEK) resulted in substantial improvement in visual acuity (VA) [6,7,8,9,10,11]. Notwithstanding the growing interest in Descemet membrane endothelial keratoplasty as a result of its better visual outcomes [12,13,14], DSAEK still remains the most popular treatment of choice for endothelial pathology [15].
It is known that DSAEK provides faster visual rehabilitation, reduced surgically induced regular or irregular astigmatism and preserves biochemical corneal strength compared to penetrating keratoplasty [4,5,6,7, 9, 10, 16,17,18]. Yet, visual outcome is often sub-optimal regardless of the clarity of the graft and fewer patients than expected achieve full visual recovery [19,20,21,22]. There are several possible reasons for this outcome, which include graft irregularities and differences in graft thickness, high order aberrations, donor-recipient interface and anterior stromal fibrosis [20, 21, 23]. Growing interest has developed in investigating graft thickness, with consensus suggesting better visual outcomes with thinner grafts after DSAEK [4, 16, 24,25,26,27].
There is conflicting evidence that the thickness of the donor button measured pre-operatively corresponds with that measured postoperatively [11, 28, 29]. There is a growing interest in nanothin (<50 μm) and ultrathin (~ <100 μm) DSAEK techniques [3, 11, 18, 27, 30,31,32]. Only a few studies have evaluated changes in DSAEK graft thickness over time, with the majority only measuring up to the 6th postoperative month [11, 33, 34].
In this case series, we aimed to describe the relationship between preoperative DSAEK graft thickness and postoperative thickness at various time-points, with a follow-up of up to 24 months.
Methods
Retrospective single-center case series where patients who underwent UT-DSAEK with eye bank-prepared tissues between April 2017 and July 2019 were included. Both types of EKs graft were pre-cut or pre-loaded at the eye bank and shipped to The Royal Liverpool University Hospital (Liverpool, UK). The retrospective data collection followed the tenets of the Declaration of Helsinki and was approved by the local Institutional Review Board (A0002786). Patients included had undergone UT-DSAEK surgery for corneal decompensation due to pseudophakic bullous keratopathy (PBK) or Fuchs’ endothelial dystrophy (FED). Both patients who received UT-DSAEK alone or combined phacoemulsification plus intraocular lens insertion and UT-DSAEK (triple surgery) were included in the study. Patients were excluded if no postoperative graft thickness measurements were present or if the graft had failed.
Donor corneas were prepared at the Venice or Monza eye bank and shipped to the Royal Liverpool University Hospital as either pre-cut only or pre-loaded tissues. Time from tissue preparation to tissue usage was recorded. Donor characteristics and graft details such as donor age, gender, endothelial cell density (ECD), graft diameter, graft thickness as reported by the eye bank and type of tissue received (pre-cut only or pre-loaded) were recorded.
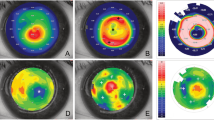
Clinical data collected were age, gender, indication for surgery, preoperative best corrected visual acuity (BCVA), procedure type (UT-DSAEK only or triple procedure), postoperative complications and occurrence of re-bubbling procedures. Postoperative BCVA and postoperative graft thickness were also obtained. Preoperative and postoperative graft thickness was measured using anterior segment optical coherence tomography (Casia AS-OCT, Tomey). High-resolution corneal scans centered on the corneal apex were selected. Axial optical resolution was 10 μm. The horizontal cross-sectional image, from 180 to 0 degrees was selected. The interface was manually identified and central corneal graft thickness was determined on the central point of the selected images. Peripheral measurements were not recorded. All measurements were taken by trained operators.
Measurements were taken postoperatively, where available, at 1 day, 1 week, 1 month, 2 months, 6 months, 12 months and 24 months. Percentage of graft thickness change between preoperative values and values at each time point were calculated.
Data are presented as mean ± standard deviation and percentages for graft thickness change. BCVA was converted into LogMAR. Preoperative and postoperative values were compared using a paired t-test.
Results
Forty-seven eyes from 47 patients who underwent DSAEK surgery were included in the study. The mean patient age at the time of surgery was 69 ± 11 years and 29 were males (62%). Indication for surgery was FED in 23 cases (49%) and PBK in 24 (51%). In total, 29/47 eyes underwent DSAEK alone (62%) and 18/47 received combined cataract surgery as a triple procedure (38%). Surgery was performed in the right eye in 51% of cases (24/47).
Average time from tissue preparation to tissue usage was 2.8 ± 0.8 days. Mean preoperative ECD was 2572 ± 134 cells/mm2.
Preoperative donor graft thickness measured 92.3 ± 28.2 μm [min 42; max 166]. Compared to preoperative values, graft thickness increased by 99.1 ± 69.1% at day 1 (194.0 ± 101.3 μm, min 82, max 347, n = 11, p = 0.003), by 50.7 ± 49.2% at 1 week (151.1 ± 71.4 μm, min 52, max 316, n = 13, p = 0.004), and by 19.5 ± 29.9% at 1 month (108.4 ± 52.5 μm, min 57, max 242, n = 12, p = 0.06). Graft thickness continued to gradually decrease over time, slowly re-assuming preoperative thickness measurements. From 2 months onwards, percentage of change in graft thickness compared to preoperative values was always within ~10%; specifically, graft thickness was increased by 3.9 ± 26.7% at 2 months (99.38 ± 24.0 μm, min 68, max 144, n = 8, p = 0.88), decreased by 11.4 ± 28.6% at 6 months (91.7 ± 33.6 μm, min 53, max 151], n = 14, p = 0.27), decreased by 2.7 ± 26.9% at 12 months (83.9 ± 25.0 μm, min 46, max 124, n = 15, p = 0.88) and increased by 7.2 ± 24.1% at 24 months (101.4 ± 37.5 μm, min 57, max 170, n = 11), p = 0.33). In general, a significant increase in graft thickness was observed on day 1, which progressively reduced until the second month, when the graft thickness was back to preoperative values, then it reached its minimum at 6 months, while it showed a minimal upwards trend at 12 and 24 months. Figure 1 shows graft thickness at different follow-up times, while Fig. 2 shows the percentage change of graft thickness compared to baseline.

Graft thickness at day 1 is doubled from the preoperative and progressively reverts back to preoperative values within the first 2 months. It remains stable at 6 and 12 months, while at 24 months it shows a minimal increase in thickness.

At day 1, the thickness is almost double the preoperative, and in the first 2 months there is the most significant reduction bringing it to a similar value as the baseline. At 6 months there is the minimum graft thickness reached and then there is a slow but progressive upward trend.
We analyzed the ratio between the graft thickness and the recipient cornea (Fig. 3). This ratio started at 0.28 ± 0.14 at day 1 and progressively reduced at 1 week (0.24 ± 0.12, p = 0.12) and at 1 month (0.19 ± 0.08, p = 0.08). Then it stabilized reaching a plateau at 12 months (0.17 ± 0.04) and started to show a minimal upwards trend at 24 months (0.2 ± 0.07).

At day 1, the ratio 0.28 and it reduces significantly within the first month, reaching 0.19. Then it plateaus until 12 months (0.17) and starts to show a minimal upwards trend at 24 months, which may represent an early graft failure in some patients. (Bottom) Graphical representation of the mathematical equation that expresses the ratio of graft thickness divided by the recipient cornea thickness. Ratio graft thickness/corneal thickness = 0.533102 + 0.000114(day) − 0.29308(day)0.1 + 0.0399368(day)0.2.
We also analyzed the ratio between the graft and the recipient cornea thickness at different follow-up times. This is expressed by the following mathematical equation:
Preoperative BCVA was 1.1 ± 0.7 LogMAR and it improved significantly at 12 months follow-up after surgery to 0.34 ± 0.3 LogMAR (p < 0.0001).
Nine patients required re-bubbling within 1 week after surgery (19%). Although graft thickness was increased at day 1 (+114 ± 68.5% vs. +93.5 ± 74%; thickness of detached vs. non-detached grafts compared with preoperative graft thickness, respectively) and in the first week after surgery (+70 ± 50% vs. +37.2 ± 50%, respectively), this difference was not significant (p = 0.41 and p = 0.23, respectively). All grafts were successfully attached at subsequent follow-up visits.
Discussion
In this study we evaluated central UT-DSAEK graft thickness change over time in comparison with preoperative graft thickness measurements. Our results show an initial marked increase in central corneal graft thickness within the first weeks after surgery, which gradually reduced over the first 6 postoperative months. At 6 months, graft thickness values were similar to those measured pre-operatively by the eye bank and beyond this time point they tended to plateau, showing a minimal increase at 2 years.
Previous studies on DSAEK have shown varying degrees of thinning over time, with thicker grafts undergoing greater reduction of thickness [11, 29]. Woodward et al. reported a mean thinning rate of 17% at 6 months, similar to results from Mater et al., showing a reduction of 12% [11, 12]. Similarly, Romano et al. reported a 15% thinning at 3 months postoperatively in patients with thinner grafts [28]. In agreement, our data showed a significant reduction in the graft thickness within the first 6 months and a graft thickness within 5% of the original preoperative baseline graft thickness measurements thereafter.
It is known that corneal deturgescence begins almost immediately [11], with central deturgescence rate peaking after 1 week [33]. Pogorelov et al. found that the thickness of the donor corneal lenticule decreases rapidly after DSAEK in almost a linear fashion. They suggested that stabilization of the total central corneal thickness and graft thickness was achieved by 8 weeks [26] and similarly, Ahmed et al. suggested that graft thickness stabilized at 3 months after surgery [35]. In contrast, longer DSAEK graft thinning times were shown by Di Pasquale et al. [33], who found that total corneal thickness and central graft thickness reached a steady state between 6-9 months, even showing a mild increase in corneal thickness between 6 and 9 months postoperatively.
Similarly, in our cohort of patients, after the initial 6 months there is a slight increase in average graft thickness and we can speculate that this may represent a very early sign of graft decompensation. However, within our follow up time of 2 years we did not witness to any graft with obvious decompensation, therefore no clear conclusion can be drawn on this.
Most patients undergoing UT-DSAEK surgery fail to achieve 6/6 vision postoperatively [4, 7, 33], with 6/12 vision often used as a benchmark. Studies vary drastically, with results varying in a range of 26 and 70% of patients achieving more than 6/12[4, 7]. Whilst VA in this study was significantly improved postoperatively (p < 0.01), the average postoperative VA was worse than 6/12. We feel this in part was perhaps due to the fact that patients were not excluded if they had underlying amblyopia, macular pathology, dense vision-limiting posterior capsule opacification or any other corneal pathology. Furthermore, there have only been a handful of studies capable of demonstrating a correlation between better VA and lower total corneal thickness [4, 16, 24, 26, 27, 36]. Most others have however failed to show any significant correlation [7, 8, 36,37,38,39,40,41,42, 12, 13, 15, 16, 26, 31, 33, 35]. There has been no randomized control study to date to assess the impact of DSAEK graft thickness on VA. Unfortunately, we are unable to comment on this because the retrospective nature of the study did not allow for a correlation to be made since VA and graft thickness were not available at each nodal time point.
As partially highlighted above, our study is not without limitations. It is retrospective in nature with caveats in serial postoperative BCVA and AS-OCT measurements at expected nodal points, which in some patients were not available. The literature shows considerable variability in graft thickness amongst conventional DSAEK techniques, ranging between 78 to 259 μm [7, 8, 26, 33, 35, 40], while in our case we opted to only consider bank-prepared DSAEK in order to increase reproducibility. That being said, our study only assessed central donor disc corneal thickness and not the peripheral thickness [43,44,45,46,47,48,49]. However, whilst central thickness may vary significantly from peripheral thickness, this does not have any statistically significant influence on postoperative VA [31]. Lastly, our graft thickness measurements were taken manually on an image acquired using AS-OCT, which might result in a less reliable measurement.
In conclusion, this study aimed to determine whether prior knowledge of the baseline UT-DSAEK graft thickness allows prediction of graft thickness at a given time point postoperatively. We found that preoperative DSAEK graft thickness as reported by the eye bank is a valid approximation of DSAEK graft thickness at 6 months and up to 2 years after surgery. A better understanding of the relationship between graft thickness and VA would be beneficial and further studies with longer follow up could help clarify whether the slight increase in graft thickness seen after the first 6 months could be representative of an early graft decompensation.
Summary
What was known before
-
Postoperative DSAEK graft thickness tends to decrease with time.
What this study adds
-
This study highlights the rate of change in the postoperative corneal graft thickness deturgescence, giving the surgeon a better understanding of expected corneal thickness at nodal postoperative time-points.
Data availability
Raw data were generated at Royal Liverpool University Hospital. Derived data supporting the findings of this study are available in the Supplementary Material (see Supplementary Table 1).
References
Melles GR, Eggink FA, Lander F, Pels E, Rietveld FJ, Beekhuis WH, et al. A surgical technique for posterior lameliar keratoplasty. Cornea. 1998;17:618–26.
Melles GRJ, Lander F, Nieuwendaal C. Sutureless, posterior lamellar keratoplasty: a case report of a modified technique. Cornea. 2002;21:325–7.
Melles GRJ, Lander F, Van Dooren BTH, Pels E, Beekhuis WH. Preliminary clinical results of posterior lamellar keratoplasty through a sclerocorneal pocket incision. Ophthalmology. 2000;107:1850–6.
Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Descemet-stripping automated endothelial keratoplasty: six-month results in a prospective study of 100 eyes. Cornea. 2008;27:514–20.
Terry MA, Ousley PJ. Deep lamellar endothelial keratoplasty in the first United States patients. Cornea. 2001;20:239–43.
Gorovoy MS. Descemet-stripping automated endothelial keratoplasty. Cornea. 2006;25:886–9.
Price MO, Price FW. Descemet’s stripping with endothelial keratoplasty. Comparative outcomes with microkeratome-dissected and manually dissected donor tissue. Ophthalmology. 2006;113:1936–42.
Terry MA, Straiko MD, Goshe JM, Li JY, Davis-Boozer D. Descemet’s stripping automated endothelial keratoplasty: the tenuous relationship between donor thickness and postoperative vision. Ophthalmology. 2012;119:1988–96.
Terry MA, Shamie N, Chen ES, Phillips PM, Shah AK, Hoar KL, et al. Endothelial keratoplasty for Fuchs’ dystrophy with cataract. Complications and clinical results with the new triple procedure. Ophthalmology. 2009;116:631–9.
Terry MA, Hoar KL, Wall J, Ousley P. Histology of dislocations in endothelial keratoplasty (DSEK and DLEK): a laboratory-based, surgical solution to dislocation in 100 consecutive DSEK cases. Cornea. 2006;25:926–32.
Meter A, Kuzman T, Kalauz M, Škegro I, Masnec S, Pavan J. Postoperative thinning of lamellar donor graft after conventional descemet’s stripping automated endothelial keratoplasty. Acta Clin Croat. 2018;57:653–7.
Woodward MA, Raoof-Daneshvar D, Mian S, Shtein RM. Relationship of visual acuity and lamellar thickness in descemet stripping automated endothelial keratoplasty. Cornea. 2013;32:e69–73.
Shinton AJ, Tsatsos M, Konstantopoulos A, Goverdhan S, Elsahn AF, Anderson DF, et al. Impact of graft thickness on visual acuity after Descemet’s stripping endothelial keratoplasty. Br J Ophthalmol. 2012;96:246–9.
Guerra FP, Anshu A, Price MO, Giebel AW, Price FW. Descemet’s membrane endothelial keratoplasty: prospective study of 1-year visual outcomes, graft survival, and endothelial cell loss. Ophthalmology. 2011;118:2368–73.
Mencucci R, Favuzza E, Tartaro R, Busin M, Virgili G. Descemet stripping automated endothelial keratoplasty in Fuchs’ corneal endothelial dystrophy: anterior segment optical coherence tomography and in vivo confocal microscopy analysis. BMC Ophthalmol. 2015;15:CD008420.
Dickman MM, Cheng YYY, Berendschot TTJM, Van Den Biggelaar FJHM, Nuijts RMMA. Effects of graft thickness and asymmetry on visual gain and aberrations after descemet stripping automated endothelial keratoplasty. JAMA Ophthalmol. 2013;131:737–44.
Koenig SB, Covert DJ. Early results of small-incision descemet’s stripping and automated endothelial keratoplasty. Ophthalmology. 2007;114:221–6.
Ousley PJ, Terry MA. Stability of vision, topography, and endothelial cell density from 1 year to 2 years after deep lamellar endothelial keratoplasty surgery. Ophthalmology. 2005;112:50–7.
Guerra FP, Anshu A, Price MO, Price FW. Endothelial keratoplasty: fellow eyes comparison of descemet stripping automated endothelial keratoplasty and descemet membrane endothelial keratoplasty. Cornea. 2011;30:1382–6.
McLaren JW, Patel SV. Modeling the effect of forward scatter and aberrations on visual acuity after endothelial keratoplasty. Investig Ophthalmol Vis Sci. 2012;53:5545.
Rudolph M, Laaser K, Bachmann BO, Cursiefen C, Epstein D, Kruse FE. Corneal higher-order aberrations after descemet’s membrane endothelial keratoplasty. Ophthalmology. 2012;119:528–35.
Li JY, Terry MA, Goshe J, Davis-Boozer D, Shamie N. Three-year visual acuity outcomes after Descemet’s stripping automated endothelial keratoplasty. Ophthalmology. 2012;119:1126–9.
Hindman HB, McCally RL, Myrowitz E, Terry MA, Stark WJ, Weinberg RS, et al. Evaluation of deep lamellar endothelial keratoplasty surgery using scatterometry and wavefront analyses. Ophthalmology. 2007;114:2006–12.
Acar BT, Akdemir MO, Acar S. Visual acuity and endothelial cell density with respect to the graft thickness in descemet’s stripping automated endothelial keratoplasty: one year results. Int J Ophthalmol. 2014;7:974–9.
Busin M, Albé E. Does thickness matter: ultrathin Descemet stripping automated endothelial keratoplasty. Curr Opin Ophthalmol. 2014;25:312–8.
Pogorelov P, Cursiefen C, Bachmann BO, Kruse FE. Changes in donor corneal lenticule thickness after Descemet’s stripping automated endothelial keratoplasty (DSAEK) with organ-cultured corneas. Br J Ophthalmol. 2009;93:825–9.
Neff KD, Biber JM, Holland EJ. Comparison of central corneal graft thickness to visual acuity outcomes in endothelial keratoplasty. Cornea. 2011;30:388–91.
Romano V, Steger B, Myneni J, Batterbury M, Willoughby CE, Kaye SB. Preparation of ultrathin grafts for Descemet-stripping endothelial keratoplasty with a single microkeratome pass. J Cataract Refract Surg. 2017;43:12–15.
Tang M, Stoeger C, Galloway J, Holiman J, Bald MR, Huang D. Evaluating DSAEK graft deturgescence in preservation medium after microkeratome cut with optical coherence tomography. Cornea. 2013;32:847–50.
Maier AKB, Gundlach E, Klamann MKJ, Gonnermann J, Bertelmann E, Joussen AM, et al. Influence of donor lamella thickness on visual acuity after Descemet’s stripping automated endothelial keratoplasty (DSAEK). Ophthalmologe. 2014;111:128–34.
Nieuwendaal CP, Van Velthoven MEJ, Biallosterski C, Van Der Meulen IJE, Lapid-Gortzak R, Melles GRJ, et al. Thickness measurements of donor posterior disks after descemet stripping endothelial keratoplasty with anterior segment optical coherence tomography. Cornea. 2009;28:298–303.
Suwan-Apichon O, Reyes JMG, Griffin NB, Barker J, Gore P, Chuck RS. Microkeratome versus femtosecond laser predissection of corneal grafts for anterior and posterior lamellar keratoplasty. Cornea. 2006;25:966–8.
Di Pascuale MA, Prasher P, Schlecte C, Arey M, Bowman RW, Cavanagh HD, et al. Corneal deturgescence after Descemet stripping automated endothelial keratoplasty evaluated by visante anterior segment optical coherence tomography. Am J Ophthalmol. 2009;148:32–7.
Kanellopoulos AJ, Asimellis G. Anterior-segment optical coherence tomography investigation of corneal deturgescence and epithelial remodeling after DSAEK. Cornea. 2014;33:340–8.
Ahmed KA, McLaren JW, Baratz KH, Maguire LJ, Kittleson KM, Patel SV. Host and graft thickness after descemet stripping endothelial keratoplasty for fuchs endothelial dystrophy. Am J Ophthalmol. 2010;150:490–7.
Feizi S, Javadi M. Effect of donor graft thickness on clinical outcomes after descemet stripping automated endothelial keratoplasty. J Ophthalmic Vis Res. 2019;14:18.
Daoud YJ, Munro AD, Delmonte DD, Stinnett S, Kim T, Carlson AN, et al. Effect of cornea donor graft thickness on the outcome of descemet stripping automated endothelial keratoplasty surgery. Am J Ophthalmol. 2013;156:860–6.
Hindman HB, Huxlin KR, Pantanelli SM, Callan CL, Sabesan R, Ching SST, et al. Post-DSAEK optical changes: a comprehensive prospective analysis on the role of ocular wavefront aberrations, haze, and corneal thickness. Cornea. 2013;32:1567–77.
Phillips PM, Phillips LJ, Maloney CM. Preoperative graft thickness measurements do not influence final BSCVA or speed of vision recovery after descemet stripping automated endothelial keratoplasty. Cornea. 2013;32:1423–7.
Roberts HW, Mukherjee A, Aichner H, Rajan MS. Visual outcomes and graft thickness in microthin DSAEK—one-year results. Cornea. 2015;34:1345–50.
Seery LS, Nau CB, McLaren JW, Baratz KH, Patel SV. Graft thickness, graft folds, and aberrations after descemet stripping endothelial keratoplasty for fuchs dystrophy. Am J Ophthalmol. 2011;152:910–6.
Van Cleynenbreugel H, Remeijer L, Hillenaar T. Descemet stripping automated endothelial keratoplasty: effect of intraoperative lenticule thickness on visual outcome and endothelial cell density. Cornea. 2011;30:1195–200.
Dupps WJ, Qian Y, Meisler DM. Multivariate model of refractive shift in Descemet-stripping automated endothelial keratoplasty. J Cataract Refract Surg. 2008;34:578–84.
Yoo SH. One-year results and anterior segment optical coherence tomography findings of descemet stripping automated endothelial keratoplasty combined with phacoemulsification. Arch Ophthalmol. 2008;126:1052.
Zhao PS, Wong TY, Wong WL, Saw SM, Aung T. Comparison of central corneal thickness measurements by visante anterior segment optical coherence tomography with ultrasound pachymetry. Am J Ophthalmol. 2007;143:1047–9.
Prospero Ponce CM, Rocha KM, Smith SD, Krueger RR. Central and peripheral corneal thickness measured with optical coherence tomography, Scheimpflug imaging, and ultrasound pachymetry in normal, keratoconus-suspect, and post-laser in situ keratomileusis eyes. J Cataract Refract Surg. 2009;35:1055–62.
Wirbelauer C, Scholz C, Hoerauf H, Pham DT, Laqua H, Birngruber R. Noncontact corneal pachymetry with slit lamp-adapted optical coherence tomography. Am J Ophthalmol. 2002;133:444–50.
Kim HY, Budenz DL, Lee PS, Feuer WJ, Barton K. Comparison of central corneal thickness using anterior segment optical coherence tomography vs ultrasound pachymetry. Am J Ophthalmol. 2008;145:228–32.
Lee WB, Jacobs DS, Musch DC, Kaufman SC, Reinhart WJ, Shtein RM. Descemet’s stripping endothelial keratoplasty: safety and outcomes. A report by the American Academy of Ophthalmology. Ophthalmology. 2009;116:1818–30.
Author information
Authors and Affiliations
Contributions
All authors equally contributed to study design, data collection, statistical analysis, drafting of the manuscript and reviewing it.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Fenech, M.T., Coco, G., Pagano, L. et al. Thinning rate over 24 months in ultrathin DSAEK. Eye 37, 655–659 (2023). https://doi.org/10.1038/s41433-022-02011-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-02011-8
