
Abstract
Study design
Post hoc analysis of prospective multi-national, multi-centre cohort study.
Objective
Determine whether cerebral dominance influences upper extremity recovery following cervical spinal cord injury (SCI).
Setting
A multi-national subset of the longitudinal GRASSP dataset (n = 127).
Methods
Secondary analysis of prospective, longitudinal multicenter study of individuals with cervical SCI (n = 73). Study participants were followed for up to 12 months after a cervical SCI, and the following outcome measures were serially assessed - the Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) and the International Standards for the Neurological Classification of SCI (ISNCSCI), including upper extremity motor and sensory scores. Observed recovery and relative (percent) recovery were then determined for both the GRASSP and ISNCSCI, based on change from initial to last available assessment.
Results
With the exception of prehension performance (quantitative grasping) following complete cervical SCI, there were no significant differences (p < 0.05) for observed and relative (percent) recovery, between the dominant and non-dominant upper extremities, as measured using GRASSP subtests, ISNCSCI motor scores and ISNCSCI sensory scores.
Conclusion
Despite well documented differences between the cerebral hemispheres, cerebral dominance appears to play a limited role in upper extremity recovery following acute cervical SCI.
Similar content being viewed by others

Introduction
Tetraplegia caused by injury to the cervical spinal cord has a significant and disabling effect on the function and independence of impacted individuals. Not surprisingly, improving arm and hand function is a high priority for individuals living with tetraplegia [1]. Following an injury to the central nervous system (CNS), such as a spinal cord injury (SCI), uninjured structures and pathways can compensate for the functions of lost and injured tissue. Termed neuroplasticity, the process has been defined as “an adaptive reorganization of the neural pathways occurring after injury that acts to restore some of the lost function” [2] or alternatively as “the CNS capacity to modify its morphological and functional properties as a response to environmental stimuli” [3].
Following a SCI, neural reorganization occurs not only in the spinal cord but also in supratentorial structures such as the motor cortex [4, 5]. This includes changes in the cortical representation of body parts and formation of new pathways in the spinal cord [6,7,8,9,10,11]. Regions of the brain that control body areas which retain some communication, enlarge and shift in location [12, 13]. In animal models, axons from the motor cortex sprout and synapse on neurons that have maintained viable descending axons, thereby forming new circuits that can bypass partial lesions and mediate recovery [14]. Due to neuroplasticity, marked functional recovery occurs following experimental SCI, with as little as ten percent of the axons spared [15,16,17].
It is also known that in the absence of SCI, there are well-established differences between the dominant and non-dominant cerebral hemispheres of the human brain [18]. The dominant hemisphere plays a larger role in motor planning and sequencing, and there is activation of the dominant but not the non-dominant hemisphere with movement of either arm [19]. Magnetoencephalography and transcranial magnetic stimulation (TMS) have revealed that hand representation is greater in the dominant cortex, compared to the non-dominant cortex [20, 21]. Using TMS, Priori and colleagues also found that the threshold required to produce movement was higher in the non-dominant hand [22]. Functional and physiological differences are also accompanied by morphological asymmetries. The central sulcus is deeper, on the dominant side, with increased neuropil volume, suggesting increased connectivity [23]. Anatomical asymmetry has also been observed in the basal ganglia and cerebellum [24, 25].
Studies in able-bodied individuals suggest that plasticity might also differ between the dominant and non-dominant motor cortices. Motor training in the hands induced greater use-dependent plasticity [26] and motor performance [27] in the non-dominant hand compared to the dominant hand.
Given the well described pre-injury differences between the dominant and non-dominant cerebral hemispheres and the reorganization of the cerebral cortices following a SCI, it is quite conceivable that the nature and extent of motor recovery after SCI could differ between the accompanying dominant and non-dominant extremities. If present, this could have important clinical implications. The primary objective of this study therefore was to compare the differences of the observed and relative (percent) recovery between the dominant and non-dominant upper extremities following cervical SCI. We are unaware of any prior study which has directly addressed this question.
Methods
Study cohort
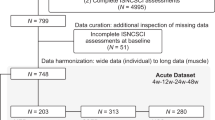
A post-hoc analysis was conducted utilizing a subset of the longitudinal Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP) dataset. The total dataset (n = 127) consists of a multi-national sample collected to establish the responsiveness and minimal clinically important difference of the GRASSP version 1 [28, 29]. Research Ethics approval was obtained at participating sites. The above dataset was used to determine the redundant elements of GRASSP versions 1, develop the GRASSP version 2, and establish the psychometric properties of the GRASSP version 2 [30, 31]. A subset of the data (n = 77) was selected for this analysis, based on whether pre-injury cerebral dominance was available.
Study participants underwent neurological assessment on at least two separate occasions following an acute cervical SCI. Follow-up extended up to 12-months post-injury; however, the 12-month time point was not available for 38 participants. While the follow-up period differed between individuals; the variable of interest (dominant vs. non-dominant extremity recovery) was assessed at the same time point in each individual. Three individuals were classified as ambidextrous and were excluded from analysis. An additional individual was assessed once and was also excluded. The final study cohort consisted of seventy-three individuals with cervical SCI. The extent of recovery between initial assessment and final assessment was then determined and compared for the dominant and non-dominant upper extremities.
International standards for the neurological classification of SCI
The International Standards for the Neurological Classification of SCI (ISNCSCI) [32] was used to determine observed motor recovery for each extremity. Observed motor recovery was defined as the magnitude of observed change in motor scores during the follow-up period. Observed motor recovery was calculated by subtracting the baseline (initial) motor score for an extremity from the final follow-up motor score. An additional measure of recovery, relative (percent) motor recovery, was also calculated. Relative (percent) motor recovery per extremity was defined as the observed motor point recovery per extremity divided by the maximum possible motor point recovery per extremity × 100. For this calculation, maximum possible recovery was defined as 25 points (maximum possible extremity score) minus the initial motor score for an extremity. For example, if the initial motor score for an upper extremity was 13 points, the maximum possible motor point recovery would be 12 points (25 points minus 13 points).
The parameter, relative (percent) recovery, compensates for potential ceiling effects associated with the ISNCSCI. The ISNCSCI has a maximal possible motor score of 25 points for an extremity. The ceiling effect is attributable to the fact that there is a ceiling on the maximum possible motor score (25 points) for an extremity. An individual that presents with a high initial motor score has fewer points that can be recovered, compared to an individual with a low initial motor score. Relative (percent) motor recovery has therefore been utilized in prior studies as an alternative measure of recovery following SCI [33, 34]. In addition, relative (percent) recovery can facilitate the comparison of upper extremity recovery in asymmetric injuries.
As an example, for an individual with an initial extremity score of 5 points that improved to 15 points (maximum possible 25 points) at follow-up; the observed motor recovery would be 10 points (15 points minus 5 points) and the relative (percent) recovery would be 50% (10 points/(25 points – 5 points) × 100). In comparison, for an individual that presented with an initial extremity score of 20 points and improved to 24 points at follow-up; observed motor recovery would be 4 points (24 points minus 20) and relative (percent) recovery would be 80% (4 points/(25 points – 20 points) × 100). The individual with the low initial motor score regained more motor points but remained more impaired, reflected in lower relative (percent) recovery, compared to the individual with the high initial motor score.
Graded redefined assessment of strength, sensibility and prehension
The GRASSP is a clinical impairment measure to assess sensorimotor hand function in persons with cervical spinal cord injuries (C1-T1). It is a multimodal test comprised of 5 subtests for each upper limb.
-
1.
Dorsal sensation is tested with Semmes-Weinstein monofilaments in 3 locations, each scored 0−4, thus the range for dorsal sensation subtest score is 0−12.
-
2.
Palmar sensation is tested with Semmes-Weinstein monofilaments in 3 locations, each scored 0−4, thus the range for palmar sensation subtest score is 0−12.
-
3.
Strength is tested for 10 muscles of the arm & hand, motor grade 0−5 for each, thus the range for the strength subtest is 0−50.
-
4.
Prehension ability (qualitative grasping) consists of 3 grasps: cylindrical, lateral key, tip to tip (each scored 0−4), thus the range for the prehension ability subtest score is 0−12.
-
5.
Prehension performance (quantitative grasping) consists of 6 prehension tasks: pour water from a bottle, open jars, pick up and turn key, transfer 9 pegs from board to board, pick up four coins and place in slots, screw four nuts onto bolts (each scored 0−5), thus the range of the prehension performance subtest score is 0−30.
In a fashion similar to the ISNCSCI motor scores, observed recovery and relative (percent) recovery per extremity were determined for each GRASSP subtest.
Statistical analysis
Observed recovery and relative (percent) recovery for selected outcome measures were assessed for significant differences between the dominant and non-dominant upper extremities using the Wilcoxon signed-rank test (alpha level ≤ 0.05). Given the known differences in natural recovery for complete vs. incomplete SCI, separate analysis was performed for individuals with incomplete vs. complete SCI. All statistical analyses were completed using SAS Enterprise Guide v7.12 (Cary, NC).
Results
Sample demographics
Sample demographics are summarized in Table 1. The sample was comprised of 73 individuals (5 left-handed and 68 right-handed) who had an acute cervical SCI between Jan 2009 and June 2011. The gender distribution was 68.5% male, 90.4% had a traumatic SCI, and mean age at injury was 49.9 ± 19.9 years of age (range 17–85). The leading injury etiologies were falls (38.9%) and sports injuries (28.8%) followed by transportation accidents (13%) and non-traumatic etiologies (9.6%). Fifty-eight study participants sustained an incomplete SCI while 13 were found to have a complete SCI. Two participants could not be categorized as incomplete or complete due to incomplete data, and were excluded from further analysis. Mean duration from injury to baseline neurological assessment was 20 ± 14 days (range 1–78 days) for the ISNCSCI and 21 ± 13 days (range 3–68 days) for the GRASSP. Mean duration between baseline neurological assessment and final neurological assessment was 294 ± 103.1 days (range 39–499) for ISNCSCI and 275 ± 114.3 days (range 21–407) for GRASSP.
Incomplete cervical SCI
The magnitude of motor and functional recovery following acute incomplete cervical SCI was similar for the dominant and non-dominant sides (Table 2).
Upper extremity motor recovery was assessed using upper motor scores derived from the ISNCSCI and the GRASSP strength subtest. Mean observed recovery for upper extremity motor scores was 6.32 ± 4.77 and 7.44 ± 5.63 points for the dominant and non-dominant upper extremities, respectively (p = 0.053). Mean relative (percent) recovery for upper extremity motor scores was 57.09 ± 32.67% and 60.92 ± 36.18% for the dominant and non-dominant upper extremities, respectively (p = 0.212). Mean observed recovery for the GRASSP strength subtest was 14.02 ± 11.04 points for the dominant upper extremity, compared to 15.34 ± 10.51 points for the non-dominant side (p = 0.952). The corresponding mean relative (percent) recovery for the GRASSP strength subtest was 47.64 ± 62.2% for the dominant upper extremity, compared to 53.49 ± 43.19% for the non-dominant upper extremity (p = 0.565).
Functional recovery of the upper extremities (prehension ability and prehension performance) was also comparable for the dominant and non-dominant upper extremities. Mean observed recovery for prehension ability (qualitative grasping) was comparable for the dominant and non-dominant upper extremities (3.79 ± 3.73 points vs. 4.09 ± 3.72 points, p = 0.394). Similar to observed recovery, mean relative (percent) recovery for prehension ability (qualitative grasping) failed to reveal significant differences between the dominant and non-dominant upper extremities (62.84 ± 40.93% vs. 66.84 ± 35.72%, p = 0.271). Mean observed recovery for prehension performance (quantitative grasping) was 9.25 ± 9.91 points for the dominant hand compared to 8.32 ± 9.48 points for the non-dominant hand (p = 0.417). Mean relative (percent) recovery for prehension performance (quantitative grasping) was 57.04 ± 40.91% for the dominant hand compared to 52.66 ± 40.13% for the non-dominant hand (p = 0.368).
GRASSP scores provided insight into sensory changes in the dominant and non-dominant upper extremities. Mean observed recovery for dorsal sensation was 1.75 ± 2.74 points for the dominant hand, compared to 1.82 ± 2.72 points for the non-dominant hand (p = 0.721). The corresponding mean relative (percent) recovery for dorsal sensation was 30.23 ± 86.82% for the dominant hand compared with 39.40 ± 63.47% for the non-dominant hand (p = 0.209). Mean observed recovery for palmar sensation was 2.28 ± 2.60 points for the dominant hand compared to 2.23 ± 2.67 points for the non-dominant hand (p = 0.948). The corresponding mean relative (percent) recovery for palmar sensation was 51.35 ± 41.03% for the dominant hand compared with 53.00 ± 55.62% for the non-dominant hand (p = 0.533).
Complete cervical SCI
Upper extremity motor and functional recovery were also assessed for study participants with complete cervical SCI. Similar to incomplete cervical SCI, there were no significant differences (p-value <0.05) observed between the dominant and non-dominant upper extremities for study participants with complete SCI; with the one exception being prehension performance (Table 3).
Mean observed recovery for upper extremity motor scores, as derived from the ISNCSCI, was found to be 5.08 ± 4.99 points for the dominant upper extremity, compared to 5.15 ± 2.91 for the non-dominant upper extremity (p = 0.212). Mean relative (percent) recovery for upper extremity motor scores was 27.95 ± 27.95% for the dominant upper extremity, compared to 27.95 ± 19.58% for the non-dominant side (p = 0.204). Mean observed recovery for the GRASSP strength subtest was found to be 7.00 ± 6.12 points for the dominant upper extremity, compared to 7.38 ± 3.43 points for the non-dominant side (p = 0.297). Mean relative (percent) recovery for the GRASSP strength subtest was 19.40 ± 19.50% for the dominant upper extremity, compared to 18.58 ± 10.69% for the non-dominant upper extremity (p = 0.542).
Mean observed recovery for prehension ability (qualitative grasping) was 1.31 ± 2.25 for the dominant hand compared to 2.08 ± 2.56 for the non-dominant hand (p = 0.516). The corresponding mean relative (percent) recovery for prehension ability (qualitative grasping) was 13.73 ± 24.82% for the dominant hand compared to 19.69 ± 25.99% for the non-dominant hand (p = 0.4688). Differences in mean observed recovery for prehension performance (quantitative grasping) also failed to reach significance, 5.50 ± 5.99 points for the dominant hand compared to 2.40 ± 3.13 points for the non-dominant hand (p = 0.188). The corresponding mean relative (percent) recovery for prehension performance (quantitative grasping) was 24.33 ± 24.55% for the dominant hand compared to 9.74 ± 14.97% for the non-dominant hand (p = 0.031); which did reach significance.
Sensory changes for the dominant and non-dominant upper extremities were similar for both dorsal and palmer sensation. Mean observed recovery for dorsal sensation as tested with Semmes-Weinstein monofilaments was 1.15 ± 2.82 points for the dominant hand compared to 1.46 ± 2.15 points for the non-dominant hand (p = 0.867), while mean relative (percent) recovery was 10.75 ± 27.42% for the dominant hand compared to 13.61 ± 20.58% for the non-dominant hand (p = 0.549). Mean observed recovery for palmar sensation was 1.31 ± 2.14 points vs. 0.77 ± 2.31 points for the dominant compared to the non-dominant hand, respectively (p = 0.421). Corresponding mean relative (percent) recovery for palmar sensation was higher for the dominant hand (15.47 ± 30.18%) compared to the non-dominant hand (6.9 ± 28.86%), but failed to reach significance (p = 0.465).
Discussion
To our knowledge, this is the first study to examine whether cerebral dominance impacts observed recovery following cervical SCI. In comparison to many pre-existing studies, the primary objective of this study was not to characterize the magnitude and nature of natural recovery following cervical SCI. Rather, the primary objective was to determine whether, irrespective of magnitude, there was differential recovery between the dominant and non-dominant extremities during the available observation (follow-up) periods. To accomplish this, we performed a retrospective analysis of a dataset derived from rigorous prospective cohort studies which validated the GRASSP, a measure of upper extremity following SCI. While there were temporal differences in the baseline assessments and accompanying follow-up intervals between study participants, each participant in essence served as their own control. For each participant, the assessments for the dominant and non-dominant upper extremities were performed at the same time points. We were therefore able to address the primary study objective.
The study employed an upper extremity specific outcome measure, the GRASSP, with demonstrated reliability and validity [35]. The responsiveness and sensitivity of the GRASSP is also superior to alternative measures such as the ISNCSCI and Spinal Cord Independence Measure (SCIM) III for detecting changes in strength, sensibility, and prehension in individuals with cervical SCI [28, 29]. Despite well-described differences between the dominant and non-dominant cerebral hemispheres and motor cortices, this analysis generally did not demonstrate significant differences in the magnitude of motor and functional recovery between the dominant and non-dominant extremities following cervical SCI. The one exception was prehension performance (quantitative grasping) following complete cervical SCI, were recovery was greater in the dominant extremity. It can be postulated that clinicians focus disproportionately on the dominant upper extremity in the context of complete cervical SCI; particularly given the critical importance of having one functional upper extremity. The prehension performance (quantitative grasping) subtest of the GRASSP focuses on functional tasks (e.g., pouring from a bottle, opening jars, picking up and manipulating objects), which would reflect the above.
The research question is an important one given the importance of upper extremity function following cervical SCI. It is essential to improve our understanding of the mechanisms and variables that affect neurological plasticity and recovery following cervical SCI; this includes possible differences between the dominant and non-dominant upper extremities. This is particularly true given that neuromodulatory strategies such as TMS have shown potential for increasing upper extremity motor output and hand dexterity [4, 36].
Several factors could account for the limited difference observed between the dominant and non-dominant upper extremities. Following complete cervical SCI, the extent of recovery is general limited to the zone of partial preservation with most individuals with complete tetraplegia spontaneously regaining one to two root levels of function [37, 38]. The limited extent of recovery following complete cervical SCI could predispose the study findings to a ceiling effect, thereby masking differences. Compared to complete cervical SCI, neurological recovery following incomplete cervical SCI is variable and often extensive [38]. In this population there is therefore a greater potential to demonstrate differences in motor and functional recovery between the dominant and non-dominant upper extremities. The results of the study, however, did not support this hypothesis. There were no significant differences in the magnitude of observed recovery between the dominant and non-dominant upper extremities following incomplete cervical SCI.
Limitations
The study was a post hoc analysis of previously collected data and subsequently the cohort size was determined by available data. This limitation could have impacted its power to detect small differences in recovery; particularly given the variability in the magnitude of recovery between study participants, as evidenced by the standard deviations and accompanying confidence intervals for the assessed outcomes. There is also the possibility that the intensity of provided therapy could have differed between extremities. This study was not designed to answer this question; however, the difference in recovery of dominant vs. non-dominant prehension performance following cervical complete SCI hints at this possibility. The expectation would be that differences in therapy intensity would be reflected in differential recovery. Future large-scale prospective studies of recovery following cervical SCI could be designed to address the issues identified above and definitively address the role of cerebral dominance.
While this study could have missed differences of a smaller scale, the question remains whether subtle differences are clinically meaningful. Overall, the results of this study suggest that differences between the dominant and non-dominant motor cortices are not a major determinant of upper extremity recovery following cervical SCI. Both cortical hemispheres might be equally efficient in maximizing recovery through spared pathways following an SCI. As described above, animal models of SCI have demonstrated marked motor recovery with as little as ten percent axon sparing [15,16,17]. While structural and functional plasticity occurs at multiple levels in the adult nervous system (cortical, subcortical, brainstem, spinal cord) in response to spinal cord injury, existing differences between cortical hemispheres might have minimal additional impact on observed recovery, either positive or negative.
Conclusion
There are well-described differences between the dominant and non-dominant cerebral hemispheres. Furthermore, neuroanatomical changes occur in both the brain and spinal cord following SCI. Despite the above, study results generally failed to reveal differences in the magnitude of dominant vs. non-dominant upper extremity motor and functional recovery following incomplete and complete cervical SCI; the exception being prehension performance (quantitative grasping) following complete cervical SCI. Cerebral dominance appears to play a limited role in upper extremity recovery following cervical SCI.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma. 2004;21:1371–83.
Bradbury EJ, McMahon SB, Bradbury EJ, McMahon SB. Spinal cord repair strategies: why do they work? Nat Rev Neurosci. 2006;7:644–53.
Gutierrez RMS, Ricci NA, Gomes QRS, Oliviera DL, Britto LR, Pires RS. et al. The effects of acrobatic exercise on brain plasticity: a systematic review of animal studies. Brain Struct Funct. 2018;223:2055–71.
Long J, Federico P, Perez MA. A novel cortical target to enhance hand motor output in humans with spinal cord injury. Brain 2017;140:1619–32.
Oudega M, Perez MA. Corticospinal reorganization after spinal cord injury. J Physiol. 2012;590:3647–63.
Turner JA, Lee JS, Schandler SL, Cohen MJ. An fMRI investigation of hand representation in paraplegic humans. Neurorehabil Neural Repair. 2003;17:37–47.
Turner JA, Lee JS, Martinez O, Medlin AL, Schandler SL, Cohen MJ, et al. Somatotopy of the motor cortex after long-term spinal cord injury or amputation. IEEE Trans Neural Syst Rehabil Eng. 2001;9:154–60.
Corbetta M, Burton H, Sinclair RJ, Conturo TE, Akbudak E, McDonald JW, et al. Functional reorganization and stability of somatosensory-motor cortical topography in a tetraplegic subject with late recovery. Proc Natl Acad Sci USA. 2002;99:17066–71.
Mikulis DJ, Jurkiewicz MT, McIlroy WE, Staines WR, Rickards L, Kalsi-Ryan S, et al. Adaptation in the motor cortex following cervical spinal cord injury. Neurology 2002;58:794–801.
Curt A, Bruehlmeier M, Leenders KL, Roelcke U, Dietz V. Differential effect of spinal cord injury and functional impairment on human brain activation. J Neurotrauma. 2002;19:43–51.
Weidner N, Ner A, Salimi N, Tuszynski MH, Weidner N, Ner A, et al. Spontaneous corticospinal axonal plasticity and functional recovery after adult central nervous system injury. Proc Natl Acad Sci USA. 2001;98:3513–8.
Fouad K, Pedersen V, Schwab ME, Brosamle C. Cervical sprouting of corticospinal fibers after thoracic spinal cord injury accompanies shifts in evoked motor responses. Curr Biol. 2001;11:1766–70.
Bruehlmeier M, Dietz V, Leenders KL, Roelcke U, Missimer J, Curt A, et al. How does the human brain deal with a spinal cord injury? Eur J Neurosci. 1998;10:3918–22.
Ghosh A, Haiss F, Sydekum E, Schneider R, Gullo M, Wyss MT, et al. Rewiring of hindlimb corticospinal neurons after spinal cord injury. Nat Neurosci. 2010;13:97–104.
Fehlings MG, Tator CH. The relationships among the severity of spinal cord injury, residual neurological function, axon counts, and counts of retrogradely labeled neurons after experimental spinal cord injury. Exp Neurol. 1995;132:220–8.
Eidelberg E, Straehley D, Erspamer R, Watkins CJ. Relationship between residual hindlimb-assisted locomotion and surviving axons after incomplete spinal cord injuries. Exp Neurol. 1977;56:312–22.
Blight AR. Cellular morphology of chronic spinal cord injury in the cat: analysis of myelinated axons by line-sampling. Neuroscience 1983;10:521–43.
Hammond G. Correlates of human handedness in primary motor cortex: a review and hypothesis. Neurosci Biobehav Rev. 2002;26:285–92.
Haaland KY, Harrington DL. Hemispheric asymmetry of movement. Curr Opin Neurobiol. 1996;6:796–800.
Volkmann J, Schnitzler A, Witte OW, Freund H. Handed-ness and asymmetry of hand representation in human motor cortex. J Neurophysiol. 1998;79:2149–54.
Wassermann EM, McShane LM, Hallett M, Cohen LG. Noninvasive mapping of muscle representations in human motor cortex. Electroencephalogr Clin Neurophysiolol. 1992;85:1–8.
Priori A, Oliviero A, Donati E, Callea L, Bertolasi L, Rothwell JC, et al. Human handedness and asymmetry of the motor cortical silent period. Exp Brain Res. 1999;128:390–6.
Amunts K, Schlaug G, Schleicher A, Steinmetz H, Dabringhaus A, Roland PE, et al. Asymmetry in the human motor cortex and handedness. Neuroimage 1996;4:216–22.
Kooistra CA, Heilman KM. Motor dominance and lateral asymmetry of the globus pallidus. Neurology 1988;38:388–90.
Snyder PJ, Bilder RM, Wu H, Bogerts B, Lieberman JA, Snyder PJ, et al. Cerebellar volume asymmetries are related to handedness: a quantitative MRI study. Neuropsychologia 1995;33:407–19.
Cirillo J, Rogasch NC, Semmler JG. Hemispheric differences in use-dependent corticomotor plasticity in young and old adults. Exp Brain Res. 2010;205:57–68.
Ridding MC, Flavel SC. Induction of plasticity in the dominant and non-dominant motor cortices of humans. Exp Brain Res. 2006;171:551–7.
Velstra IM, Curt A, Frotzler A, Abel R, Kalsi-Ryan S, Rietman JS, et al. Changes in strength, sensation and prehension in acute cervical spinal cord Injury: European Multicenter Responsiveness Study of the GRASSP. Neurorehabil Neural Repair. 2015;29:755–66.
Kalsi-Ryan S, Beaton D, Ahn H, Askes H, Drew B, Curt A, et al. Responsiveness, sensitivity and minimally detectable difference of the graded and redefined assessment of strength, sensibility, and prehension, version 1.0 (GRASSP V1). J Neurotrauma. 2016;33:307–14.
Kalsi-Ryan S, Chan C, Verrier M, Curt A, Fehlings M, Bolliger M. et al. The graded redefined assessment of strength sensibility and prehension version 2 (GV2): psychometric properties. J Spinal Cord Med. 2019;42:149–57. sup1.
Velstra IM, Fellinghauer C, Abel R, Kalsi-Ryan S, Rupp R, Curt A, et al. The graded and redefined assessment of strength, sensibility, and prehension version 2 provides interval measure properties. J Neurotrauma. 2018;35:854–63.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al. International standards for neurological classification of spinal cord injury (Revised 2011). J Spinal Cord Med. 2011;34:535–46.
Waters RL, Adkins RH, Sie IH, Yakura JS. Motor recovery following spinal cord injury associated with cervical spondylosis: a collaborative study. Spinal Cord. 1996;34:711–5.
Curt A, Van Hedel HJ, Klaus D, Dietz V. Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. J Neurotrauma. 2008;25:677–85.
Kalsi-Ryan S, Beaton D, Curt A, Duff S, Popovic MR, Rudhe C, et al. The graded redefined assessment of strength sensibility and prehension: reliability and validity. J Neurotrauma. 2012;29:905–14.
Christiansen L, Perez MA. Targeted-plasticity in the corticospinal tract after human spinal cord injury. Neurotherapeutics. 2018;15:618–27.
Ditunno JF Jr, Stover SL, Freed MM, Ahn JH. Motor recovery of the upper extremities in traumatic quadriplegia: a multicenter study. Arch Phys Med Rehabil. 1992;73:431–6.
Burns AS, Marino RJ, Flanders AE, Flett H. Clinical diagnosis and prognosis following spinal cord injury. Handb Clin Neurol. 2012;109:47–62.
Acknowledgements
We would like to thank the GRASSP Research and Development Group for providing the resources to conduct this analysis.
Author information
Authors and Affiliations
Contributions
MB contributed to the study design, data analysis, and manuscript preparation. SK contributed to construction of the analyzed data set, and provided feedback during manuscript preparation. JJD contributed to the data analysis. ASB contributed to the study design, data analysis, and manuscript preparation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study utilized a subset of the multinational, longitudinal Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP) dataset. Research ethics approval was obtained at contributing sites.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bondi, M., Kalsi-Ryan, S., Delparte, J.J. et al. Differences in sensorimotor and functional recovery between the dominant and non-dominant upper extremity following cervical spinal cord injury. Spinal Cord 60, 422–427 (2022). https://doi.org/10.1038/s41393-022-00782-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00782-1
This article is cited by
-
Upper extremity asymmetry due to nerve injuries or central neurologic conditions: a scoping review
Journal of NeuroEngineering and Rehabilitation (2023)
-
Characterizing neurological status in individuals with tetraplegia using transcutaneous spinal stimulation
Scientific Reports (2023)
