
Abstract
Objective
To investigate the association between change in body mass index (BMI) from birth to 36 weeks gestation (ΔBMI) and bronchopulmonary dysplasia (BPD) among infants born <30 weeks gestation.
Methods
This was a multicenter retrospective cohort study (2015–2018) of infants born <30 weeks gestation and alive at ≥34 weeks corrected. Main exposure was a change in BMI z score from birth to 36 weeks corrected age grouped into quartiles of change. Association between ΔBMI z scores and BPD was assessed using generalized linear mixed models.
Results
Among 772 included infants, 51% developed BPD. From birth to 36 weeks CGA, the weight z score of infants with BPD decreased less than for BPD-free infants, despite a greater decrease in length z score and similar caloric intake resulting in increases in BMI z score (median [IQR], 0.16 [–0.64; 1.03] vs –0.29 [–1.03; 0.49]; P < 0.01). In the adjusted analysis, higher ΔBMI z score quartiles were associated with higher odds of BPD (Q3 vs Q2, AOR [95% CI], 2.02 [1.23; 3.31] and Q4 vs Q2, AOR [95% CI], 2.00 [1.20; 3.34]).
Conclusion
Among preterm infants, an increase in BMI z score from birth to 36 weeks corrected is associated with higher odds of BPD.
Impact
-
Preterm infants with evolving lung disease often experience disproportionate growth in the neonatal period. In this multicenter cohort study, increases in BMI z score from birth to 36 weeks CGA were associated with higher odds of BPD.
-
Despite similar caloric intake, infants with BPD had a higher weight- but lower length-for-age, resulting in higher BMI z score compared to BPD-free infants.
-
This suggests that infants with evolving BPD may require different growth and nutritional targets compared to BPD-free infants.
Similar content being viewed by others

Introduction
Bronchopulmonary dysplasia (BPD) is the most common morbidity among infants born <30 weeks gestational age (GA) affecting over 45% of survivors.1,2 It is associated with higher hospital costs and long-term complications, including neurodevelopmental impairment.3,4,5 The causes of BPD are multifactorial; a low GA, surfactant deficiency, persistent inflammation, prolonged invasive ventilation, and oxidative damage are important contributing factors.2,4,6 Optimal nutritional management of preterm infants with evolving BPD is complex due to their hypermetabolic needs associated with postnatal growth and increased work of breathing.7,8,9 Nutritional interventions commonly focus on achieving optimal body weight gain with less attention to linear growth and body composition.10 Indeed, previous studies in infants with evolving BPD have focused on the association of body weight and head circumference with neurodevelopmental outcomes but seldom on growth trajectories and body composition changes.11,12,13
A lower birth body mass index (BMI) z score, used as an indirect measure of body fat14,15 likely reflects asymmetric fetal growth restrictions and has been associated with higher odds of BPD.16 However, changes in BMI during hospitalization, reflecting disproportionate growth, may further contribute to BPD. A higher BMI in adults is associated with increased ventilatory needs in intensive care units.17,18 Therefore, this study aimed to compare growth patterns of infants with and without BPD, and evaluate the association of changes in BMI z score from birth to 36 weeks corrected gestational age (CGA) with BPD among infants born at <30 weeks of GA. We hypothesized that infants with the most extreme changes in BMI z score would have increased odds of BPD.
Methods
Study population and eligibility criteria
This was a multicenter retrospective cohort study using a convenience sample of infants admitted to three tertiary neonatal intensive care units (NICU) between January 1, 2015, and December 31, 2018. We included infants born at 220–296 weeks GA, admitted within 1 day after birth. Infants who had major congenital anomalies, died before 34 weeks GA, or had missing length measurements before 14 days or at 36 weeks CGA were excluded. Ethics approval was obtained from the Research Ethics Board of each participating site.
Data collection
Data on infant characteristics and outcomes were obtained from the Canadian Neonatal Network database. At each site, patient information is entered electronically by trained abstractors into a data-entry program with built-in error checking that has shown high reliability and internal consistency.19 GA was calculated hierarchically from the best estimate based on the date of in vitro fertilization, prenatal ultrasound, last menstrual period, obstetric and pediatric estimates. The following characteristics were extracted: use of antenatal steroids (partial or complete), multiple delivery, mode of delivery, outborn, birth GA, birth weight, small for GA status (SGA; defined as <10th percentile for GA and sex),20 sex, 5-min Apgar <7, Score of Neonatal Acute Physiology version 2 (SNAP-II) >20,21 surfactant, mechanical ventilation, postnatal systemic steroid, necrotizing enterocolitis (NEC; defined as stage 2 or 3 NEC according to Bell’s classification22), and patent ductus arteriosus (PDA; diagnosed based on clinical suspicion and/or echocardiography findings).
Biweekly anthropometric data (weight, length, and head circumference) and caloric intake from birth to 36 weeks CGA were collected from a medical chart review. Weight and length were used to calculate BMI (g/cm2). Biweekly caloric intake (kcal/kg/d) was calculated from each infant’s actual total caloric intake (parenteral and enteral) received on the days the anthropometric measurements were taken.
Standards of care
Nutritional approaches and feeding protocols were comparable across the sites (Supplementary Table 1). Parenteral nutrition was initiated after birth at 65–80 ml/kg/day and enteral feeding was initiated within 12–48 h of birth. Parenteral and enteral nutrition were adjusted by neonatologist in collaboration with trained neonatal dietitians and/or pharmacists. Typical objectives were to achieve 90–120 kcal/kg/d and 3.5–4.5 g/kg/d of protein by days 3–5, and full enteral feeding within 2–3 weeks of life. Weight was measured daily using a neonatal scale. Length and head circumference were measured at least biweekly by a trained registered nurse and nursing assistant using either an infantometer or measuring tape.
Exposure variables and outcome definitions
Weight-, length- and head circumference-for-age z scores were calculated using the 2013 Fenton reference standards20 and BMI-for-age z scores were calculated using the 2015 Olsen reference standards.14,23 Length z scores before 23.5 weeks CGA and BMI z scores before 24.5 weeks CGA were based on extrapolated data as measurements fell beyond the published growth charts.23 The main exposure variables were changes in BMI (ΔBMI), weight (Δwt), length (Δlt), and head circumference (Δhc) z scores from birth to 36 weeks CGA, using the closest value recorded between 340 and 386 weeks CGA. To maximize the number of available datapoints, birth length values were imputed for 48 infants for whom the first length measurement was between 7 and 13 days of life; values were imputed by subtracting the mean difference in length from birth to 13 days for the remaining cohort (0.89 cm). The primary outcome of BPD was defined as the need for oxygen or respiratory support at 36 weeks CGA, or at the time of death or NICU discharge before 36 weeks CGA. BPD severity was graded as mild, moderate, and severe using standardized definitions (Supplementary Table 2).1
Statistical analyses
Descriptive comparisons between infants with and without BPD were conducted using the Pearson χ2 test for categorical variables and Wilcoxon rank-sum test for continuous variables. Growth trajectories were compared between the two groups by plotting the median biweekly measurements (BMI, weight, length, head circumference z scores, and caloric intake), from birth up to 14 weeks postnatally.
Since the association between ΔBMI and BPD was nonlinear, ΔBMI was categorized into quartiles. Quartile 2 (Q2) was used as the reference category since the ΔBMI range in this group (showing a ΔBMI that slightly decreased) was similar to previously described postnatal BMI trajectory in preterm infants and we hypothesized that the most extreme changes would have the highest odds of BPD.24 Generalized linear mixed models including site as random effect were used to assess the association between ΔBMI quartiles and BPD; crude and adjusted odds ratios (OR) with corresponding 95% CI were reported. Two adjustment models were evaluated: the birth model included antenatal steroid exposure, GA, sex, multiple delivery, mode of delivery, SGA status, and SNAP-II score >20, while the postnatal model included all birth model variables, mechanical ventilation exposure, NEC (due to possible effect of NEC on growth), and PDA (due to possible changes in fluid management due to PDA). Collinearity was assessed with a variance inflation factor >5.25 Birth weight and use of surfactant and postnatal steroids were excluded from regression models due to collinearity with GA and mechanical ventilation, respectively. Primary analyses aimed to evaluate the association of BPD with ΔBMI, and secondary analyses evaluated associations with quartiles of Δwt, Δlt, and Δhc in attempts to better understand what components of growth better correlate with BPD. Secondary analyses were not adjusted for multiple comparisons as these were conducted to generate hypotheses and should be interpreted with caution.26 Biweekly median caloric intake was plotted based on ΔBMI quartiles and comparisons were made using the Kruskal–Wallis test.
Additional analyses were performed for exploratory purposes and should be interpreted as such. Ordinal regression models, adjusted for the same confounders as above, were used to assess the association of BPD severity with ΔBMI, Δwt, Δlt, and Δhc quartiles. Sensitivity analyses were conducted by stratifying GA groups (22–256 and 26–296), SGA status, and postnatal systemic steroid exposure, to address the potential differences in growth trajectories of lower GA and SGA infants and the possible effects of postnatal systemic steroids on body composition. Statistical significance was set at a two-tailed P value <0.05. Analyses were performed in R version 3.6.1 using Tidyverse version 1.3.0.27,28
Results
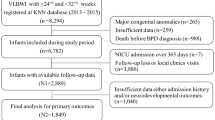
During the study period, 1023 infants were born <30 weeks GA at participating sites and 251 infants were excluded (29 had a major congenital anomaly, 139 died before 34 weeks GA and 83 had a missing length at birth or 36 weeks [Supplementary Fig. 1]). Excluded infants due to a missing length at birth or 36 weeks had a higher birth weight, higher GA and were discharged/transfer prior to 36 weeks (Supplementary Table 3). Of the 772 infants included in the final study sample, 391 (51%) developed BPD. Among infants with BPD, 44 (12%) had mild BPD, 244 (66%) had moderate BPD and 83 (22%) had severe BPD. A total of 11 (1%) infants died, all of whom were >35 weeks CGA at the time of death and met the criteria for BPD.
Comparison of growth trajectories between BPD and BPD-free infants
Compared to BPD-free infants, infants with BPD had similar rates of antenatal steroid exposure, were more frequently delivered by cesarean, born at lower GA and birth weight, and more frequently had a SNAP-II score >20, exposed to surfactant, mechanical ventilation, postnatal steroids, and were more often diagnosed with NEC and PDA (Table 1). At birth, median weight, length, and head circumference z scores were significantly lower for BPD infants compared to BPD-free infants but there was no significant difference in median BMI z score at birth. At 36 weeks CGA, there was no difference in median weight z scores, but length and head circumference z scores remained significantly lower resulting in a significantly higher BMI z score in BPD infants compared to BPD-free infants.
Figure 1 shows the anthropometric trajectories and caloric intake between BPD and BDP-free infants from birth to 14 weeks postnatal. Infants with BPD were born with similar BMI z scores, but lower weight and length z scores compared to BPD-free infants. After week 2, infants with BPD had higher biweekly BMI z scores, similar weight z scores and lower length z scores, despite similar biweekly caloric intakes.

BMI body mass index, HC head circumference. Points and error bars represent median [IQR]. Unadjusted P values derived from the Wilcoxon rank-sum test. Adjusted P values derived from generalized linear mixed models including site as random effect and patient confounders (antenatal steroids, multiple delivery, caesarian delivery, GA at birth, SGA status, sex, SNAP-II score >20, mechanical ventilation during admission, NEC, and PDA).
Association of ΔBMI with BPD
When comparing the characteristics of infants across ΔBMI quartiles, infants in Q3 and Q4 had higher rates of BPD than those in Q1 and Q2 (Supplementary Table 4). Compared to all other quartiles, infants in Q4 had a greater increase in ΔBMI, a smaller decrease in Δwt, and a greater decrease in Δlt from birth to 36 weeks CGA. After adjusting for birth and postnatal variables, infants in Q3 and Q4 of ΔBMI had higher odds of BPD compared to Q2 (Table 2). Similarly, Q3 and Q4 of Δwt were associated with higher odds of BPD after adjustment for postnatal variables, whereas associations were non-significant between Δlt quartiles and BPD.
Biweekly caloric intake using postnatal age and CGA was compared between ΔBMI quartiles in Fig. 2. Infants in Q4 had higher caloric intakes from 27 to 33 weeks CGA than those in other quartiles (unadjusted comparisons). In the ordinal regression analysis for the association of ΔBMI with BPD severity, Q3 (AOR [95% CI], 1.85 [1.20–2.86]) and Q4 (AOR [95% CI], 1.93 [1.24–3.01]) were associated with BPD severity compared to Q2 in the postnatal model (Supplementary Table 5). Sensitivity analysis based on GA group (<26 and 26–29 weeks), SGA status, and postnatal systemic steroid exposure showed similar results or effect directions: Q3 and Q4 of ΔBMI were associated with higher odds of BPD compared to Q2 (Supplementary Table 6). Sensitivity analysis among neonates with no imputed data (N = 724) also showed similar results (results not shown).

a Caloric intake accoridng to postnatal age. b Caloric intake according to corrected gestational age. An asterisk symbol (*) indicates P value < 0.05 from the Kruskal–Wallis test.
Discussion
In this multicenter cohort of preterm infants born <30 weeks GA, an increase in BMI z score from birth to 36 weeks was associated with higher odds of BPD. At birth, infants who developed BPD were proportionately smaller, with lower weight and length z scores, compared to BPD-free infants, with no significant difference in BMI z score. By 36 weeks CGA, BPD infants had higher BMI z scores due to a combination of higher weight gain velocity but slower linear growth despite receiving similar caloric intakes as BPD-free infants.
Our findings are consistent with several studies that have shown lower birth weight, length, and head circumference z scores are associated with the development of BPD.11,29,30 However, our study expands on prior work by including a description of changes in length and BMI z scores from birth to 36 weeks based on BPD status. Contrary to a recent study by Lee et al., we observed no significant difference in birth BMI z score between BPD and BPD-free infants, which may be explained by differences in study populations and inclusion criteria:16 Our study excluded infants who died <34 weeks GA who may have had a lower BMI z score at birth which differs from Lee et al. who assessed the association of birth BMI with all neonatal outcomes. Also, Lee et al. included infants based on birth weight <1500 g (regardless of GA), which may have led to including more infants with growth restriction. At 36 weeks CGA, weight z score was similar in BPD and BPD-free groups despite a lower birth weight z score. Our results are consistent with a large UK study showing that infants with BPD had a smaller decrease in Δwt compared to BPD-free infants.11 Length and head circumference z scores remained significantly lower in infants with BPD at 36 weeks CGA. This relative weight “catch up” in infants with BPD combined with poor linear growth may explain why these infants had a higher ΔBMI despite similar caloric intake.
Based on growth trajectories, we hypothesize that the higher ΔBMI in BPD infants was due to a combination of factors including lower weight loss in the first 2 weeks of life, a higher Δwt, and lower Δlt compared to BPD-free infants. The lower initial weight loss in the BPD group is possibly a reflection of differences in fluid balance (either due to intake and/or diuresis post birth), insensible water loss, differences in use of parenteral nutrition and disease severity which are also associated with BPD.31,32,33 While fluid balance likely contributes to ΔBMI in the first 14 days, the contribution of nutritional intake to changes in BMI likely increases in weeks after birth as nutrition becomes better established. Several investigators have shown that preterm infants often experience disproportionate growth with increased adiposity compared to term infants by discharge.34,35,36 Currently, adjustment of nutrition for infants growing disproportionately remains unclear as growth assessment is primarily focused on weight for age. While BMI cannot distinguish between fat mass, fat-free mass, and fluid, studies have shown that a higher BMI correlates with higher fat mass in preterm infants, making BMI a reasonable proxy for body fat percentage.34,37,38 This has been validated against dual-energy X-ray absorptiometry and bioimpedance analysis which are more accurate but less accessible in clinical practice.36,39,40,41 Different anthropometric ratios of body proportionality have also been compared and BMI was consistently the best measure of disproportionate growth in preterm infants.14,42 Although BMI has been suggested as a validated and non-invasive method to assess body proportionality in the NICU for preterm infants, how to integrate it into clinical practice still needs to be investigated.14,15,42,43
To better understand the association of ΔBMI, we used several adjustment models and sensitivity analyses. Across all models, quartiles with an increasing ΔBMI (Q3 and Q4) were consistently associated with increased odds of BPD. This novel finding suggests infants with BPD appeared to have a different growth potential even when provided with similar calories. We hypothesized that the combination of episodes of hypometabolic hypoxia, chronic inflammation and nutritional epigenetic may alter the growth and metabolism of infants with evolving BPD.44,45,46,47,48,49,50 Alternatively, the extent of change in BMI z score as early as at 2 weeks of life can perhaps be a marker of a more severe phenotype of BPD requiring a different nutritional approach. Despite similar caloric intakes, our results suggest that disproportionate weight gain in relation to linear growth might correlate with increased fat mass and contribute to delayed weaning from mechanical ventilation and development of BPD. Studies in ventilated adults have shown that physiological alterations from obesity can increase upper airway resistance, alveolar de-recruitment, and decreased respiratory compliance.17,18,51,52 Although this has not been studied in preterm infants, similar changes may occur; a higher fat mass and lower lean body mass may impact ventilatory requirements. BPD-free infants had lower BMI z scores after postnatal week 2 but also a better linear growth which could reflect a higher percentage of lean body mass. Linear growth is generally recognized as a better indicator of lean body mass accretion, organ growth, and nutritional adequacy, which together can improve muscle function involved in lung mechanics.3,53,54 It is also possible that prolonged intermittent hypoxia, inflammation, and steroid exposure in infants with BPD alter their metabolic profile in a way that may predispose them to disproportionate growth; thus, potentially making the relationship between BMI and BPD bidirectional.
Current preterm guidelines focus on achieving standard growth velocities regardless of the infant’s disease status. Weight gain and head circumference are overwhelmingly used as a benchmark of adequate postnatal growth. This study highlights the need to identify and validate other indicators for postnatal growth in preterm infants. For example, the consensus guidelines for term-corrected children with severe BPD emphasize monitoring somatic growth by aiming for an ideal weight-for-length ratio at ~50%, preventing excessive weight gain, and reassessing calories when weight gain crosses the growth chart percentile.3 In addition, Williamson et al. recently developed longitudinal BMI curves based on the postnatal growth of preterm infants.24 However, there is no definition for excessive weight gain in preterm neonates prior to term-corrected age and more research is required to better understand if a positive change in BMI z score correlates with fat mass deposition and/or fluid accumulation. It is also unclear how and if nutritional interventions can change body proportionality and health outcomes in the neonatal period. Optimal growth in preterm infants appears to be about striking a balance between two extremes. Further research is required to evaluate if and how monitoring of ΔBMI combined with other anthropometric measurements can help achieve a more balanced postnatal growth among infants born less than 30 weeks GA.
Strengths and limitations
Strengths of this study include the analyses of each individual growth parameters (BMI, weight, length, and head circumference) at multiple time points and their association with BPD using a large multicenter cohort with a validated dataset. Caloric intake was assessed based on actual intake received at the same time points to mitigate the confounding effect of nutrition in association with BPD. Our results were consistent across adjusted models, analysis of exposures for each 2-week period, and in sensitivity analyses.
This study has limitations. Having used retrospective data, we cannot infer causality and account for errors in reporting measurements and caloric intakes that may have happened. Other nutritional components that may impact BPD such as macronutrient (protein, fat, macronutrient distribution), modality of feeding (enteral to parenteral ratio) and fluid intake were not included. Although we adjusted for postnatal factors that can affect growth and fluid balance such as NEC and PDA, we did not have data on fluid intake and fluid balance. There may be residual confounding due to different clinical practices for nutrition, ventilation, or steroid exposure among centers despite statistical adjustment and sensitivity analysis. Although sensitivity analysis among non-SGA showed similar results (association of higher ΔBMI z score with BPD), we cannot fully account for differences in intra-uterine growth restrictions and need for postnatal catch-up growth. Caloric intake was assessed biweekly and may not reflect the cumulative effect of energy intake on growth. The use of BPD as a primary binary outcome has limitations since it does not fully correlate with lung growth, lung function, and long-term respiratory outcomes. The grouping of the exposure into quartiles of change due to the nonlinear association between ΔBMI and BPD also has limitations such as assuming a similar effect for all values within each quartile and using cut-off based on the data distribution.55 Further research is required to better define and validate the expected postnatal BMI trajectory in preterm infants.24 The exclusion of infants that died before 34 weeks (because these infants would not have a known BPD status) may contribute to survival bias.
Conclusions
An increasing BMI z score from birth to 36 weeks was independently associated with higher odds of BPD. This positive ΔBMI from birth to 36 weeks was due to a lower weight loss in the first 2 weeks of life, a higher weight gain overtime, and a slower linear growth velocity, despite no differences in caloric intake when compared to BPD-free infants. These findings suggest that infants who develop BPD may have altered metabolism and may require individualized growth targets. Future studies on macronutrient intake and body composition are required to better identify nutritional goals in very preterm infants with evolving lung disease.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from the corresponding author on reasonable request.
References
Isayama, T. et al. Revisiting the definition of bronchopulmonary dysplasia: effect of changing panoply of respiratory support for preterm neonates. JAMA Pediatr. 171, 271–279 (2017).
Wu, S.-Y., Gupta, S., Chen, C.-M. & Yeh, T. F. in Lung Diseases – Selected State of the Art Reviews (ed Irusen, D. E. M.) 493–484 (In Tech, 2012).
Abman, S. H. et al. Interdisciplinary care of children with severe bronchopulmonary dysplasia. J. Pediatr. 181, 12–28.e11 (2017).
Kinsella, J. P., Greenough, A. & Abman, S. H. Bronchopulmonary dysplasia. Lancet 367, 1421–1431 (2006).
Lapcharoensap, W., Lee, H. C., Nyberg, A. & Dukhovny, D. Health care and societal costs of bronchopulmonary dysplasia. NeoReviews 19, e211–e223 (2018).
Jensen, E. A. Prevention of bronchopulmonary dysplasia: a summary of evidence-based strategies. NeoReviews 20, e189–e201 (2019).
Rocha, G., Guimarães, H. & Pereira-da-Silva, L. The role of nutrition in the prevention and management of bronchopulmonary dysplasia: a literature review and clinical approach. Int J. Environ. Res. Public Health 18, 6245 (2021).
Theile, A. R., Radmacher, P. G., Anschutz, T. W., Davis, D. W. & Adamkin, D. H. Nutritional strategies and growth in extremely low birth weight infants with bronchopulmonary dysplasia over the past 10 years. J. Perinatol. 32, 117–122 (2012).
Uberos, J., Jimenez-Montilla, S., Molina-Oya, M. & García-Serrano, J. L. Early energy restriction in premature infants and bronchopulmonary dysplasia: a cohort study. Br. J. Nutr. 123, 1024–1031 (2020).
Lee, S. M. et al. Prediction of postnatal growth failure among very low birth weight infants. Sci. Rep. 8, 3729–3729 (2018).
Dassios, T., Williams, E. E., Hickey, A., Bunce, C. & Greenough, A. Bronchopulmonary dysplasia and postnatal growth following extremely preterm birth. Arch. Dis. Child Fetal Neonatal Ed. 106, 386–391 (2021).
Raghuram, K. et al. Head growth trajectory and neurodevelopmental outcomes in preterm neonates. Pediatrics 140, e20170216 (2017).
Belfort, M. B., Gillman, M. W., Buka, S. L., Casey, P. H. & McCormick, M. C. Preterm infant linear growth and adiposity gain: trade-offs for later weight status and intelligence quotient. J. Pediatr. 163, 1564–1569.e1562 (2013).
Olsen, I. E. et al. BMI curves for preterm infants. Pediatrics 135, e572–e581 (2015).
Villar, J. et al. Body composition at birth and its relationship with neonatal anthropometric ratios: the newborn body composition study of the Intergrowth-21(St) Project. Pediatr. Res. 82, 305–316 (2017).
Lee, B. K., Lee, J. H., Shin, J., Jung, Y. H. & Choi, C. W. The association of low body mass index with neonatal morbidities in preterm infants. Sci. Rep. 11, 18841 (2021).
Dennis, D. M., Bharat, C. & Paterson, T. Prevalence of obesity and the effect on length of mechanical ventilation and length of stay in intensive care patients: a single site observational study. Aust. Crit. Care 30, 145–150 (2017).
Shashaty, M. G. & Stapleton, R. Physiologic and management implications of obesity in critical illness. Ann. Am. Thorac. Soc. 11, 1286–1297 (2014).
Shah, P. S. et al. Internal audit of the Canadian Neonatal Network data collection system. Am. J. Perinatol. 34, 1241–1249 (2017).
Fenton, T. R. & Kim, J. H. A systematic review and meta-analysis to revise the fenton growth chart for preterm infants. BMC Pediatr. 13, 59 (2013).
Beltempo, M. et al. SNAP-II for prediction of mortality and morbidity in extremely preterm infants. J. Matern. Fetal Neonatal Med. 32, 2694–2701 (2019).
Bell, M. J. et al. Neonatal necrotizing enterocolitis. therapeutic decisions based upon clinical staging. Ann. Surg. 187, 1–7 (1978).
Chou, J. H., Roumiantsev, S. & Singh, R. Peditools electronic growth chart calculators: applications in clinical care, research, and quality improvement. J. Med. Internet Res. 22, e16204 (2020).
Williamson, A. L. et al. Longitudinal BMI growth curves for surviving preterm NICU infants based on a large US sample. Pediatrics 142, e20174169 (2018).
UCLA ARC. Regression with SPSS Chapter 2- Regression Diagnostics. (2021) https://stats.idre.ucla.edu/spss/webbooks/reg/chapter2/spss-webbooksregressionwith-spsschapter-2-regressiondiagnostics/.
Rothman, K. J. No adjustments are needed for multiple comparisons. Epidemiology 1, 43–46 (1990).
Wickham, H. et al. Welcome to the tidyverse. J. Open Source Softw. 4, 1686 (2019).
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/ (2020).
Huysman, W. A. et al. Growth and body composition in preterm infants with bronchopulmonary dysplasia. Arch. Dis. Child Fetal Neonatal. Ed. 88, 46–51 (2003).
deRegnier, R. O., Guilbert, T. W., Mills, M. M. & Georgieff, M. K. Growth failure and altered body composition are established by one month of age in infants with bronchopulmonary dysplasia. J. Nutr. 126, 168–175 (1996).
Matsushita, F. Y., Krebs, V. L. J., Ferraro, A. A. & de Carvalho, W. B. Early fluid overload is associated with mortality and prolonged mechanical ventilation in extremely low birth weight infants. Eur. J. Pediatr. 179, 1665–1671 (2020).
Soullane, S. et al. Fluid status in the first 10 days of life and death/bronchopulmonary dysplasia among preterm infants. Pediatr. Res. 90, 353–358 (2021).
Guo, M. M.-H. et al. Severe bronchopulmonary dysplasia is associated with higher fluid intake in very low-birth-weight infants: a retrospective study. Am. J. Perinatol. 32, 155–162 (2015).
Pereira-da-Silva, L., Virella, D. & Fusch, C. Nutritional assessment in preterm infants: a practical approach in the NICU. Nutrients 11, 1999 (2019).
Tremblay, G. et al. Body composition in very preterm infants: role of neonatal characteristics and nutrition in achieving growth similar to term infants. Neonatology 111, 214–221 (2017).
Nagel, E. et al. Clinical application of body composition methods in premature infants. JPEN J. Parenter. Enter. Nutr. 44, 785–795 (2020).
Gallagher, D. et al. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am. J. Epidemiol. 143, 228–239 (1996).
Strydom, K., Van Niekerk, E. & Dhansay, M. A. Factors affecting body composition in preterm infants: assessment techniques and nutritional interventions. Pediatr. Neonatol. 60, 121–128 (2019).
Algotar, A. et al. Unique patterns of body composition and anthropometric measurements during maturation in neonatal intensive care unit neonates: opportunities for modifying nutritional therapy and influencing clinical outcomes. JPEN J. Parenter. Enter. Nutr. 42, 231–238 (2018).
Cooke, R. J. & Griffin, I. Altered body composition in preterm infants at hospital discharge. Acta Paediatr. 98, 1269–1273 (2009).
Bott, L. et al. Body composition in children with bronchopulmonary dysplasia predicted from bioelectric impedance and anthropometric variables: comparison with a reference dual X-ray absorptiometry. Clin. Nutr. 25, 810–815 (2006).
Ferguson, A. N. et al. BMI is a better body proportionality measure than the ponderal index and weight-for-length for preterm infants. Neonatology 113, 108–116 (2018).
Paviotti, G. et al. Body mass index curves for Italian preterm infants are comparable with American curves for infants born before 34 weeks of gestational age. Acta Paediatr. 105, 483–489 (2016).
Belfort, M. B. et al. Systemic inflammation in the first 2 weeks after birth as a determinant of physical growth outcomes in hospitalized infants with extremely low gestational age. J. Pediatr. 240, 37–43.e31 (2022).
Gu, C. & Jun, J. C. Does hypoxia decrease the metabolic rate? Front. Endocrinol. 9, 668–668 (2018).
Pozo, M. et al. Effect of postnatal intermittent hypoxia on growth and cardiovascular regulation of rat pups. Neonatology 102, 107–113 (2012).
Cuestas, E., Aguilera, B., Cerutti, M. & Rizzotti, A. Sustained neonatal inflammation is associated with poor growth in infants born very preterm during the first year of life. J. Pediatr. 205, 91–97 (2019).
Baye, K. & Hirvonen, K. Evaluation of linear growth at higher altitudes. JAMA Pediatr. 174, 977–984 (2020).
Mohammed, S. H. et al. The relationship between residential altitude and stunting: evidence from >26 000 children living in highlands and lowlands of Ethiopia. Br. J. Nutr. 123, 934–941 (2020).
Ream, M., Ray, A. M., Chandra, R. & Chikaraishi, D. M. Early fetal hypoxia leads to growth restriction and myocardial thinning. Am. J. Physiol. Regul. Integr. Comp. Physiol. 295, R583–R595 (2008).
Lee, C. K., Tefera, E. & Colice, G. The effect of obesity on outcomes in mechanically ventilated patients in a medical intensive care unit. Respiration 87, 219–226 (2014).
Dixon, A. E. & Peters, U. The effect of obesity on lung function. Expert Rev. Respir. Med. 12, 755–767 (2018).
Lawn, C. J., Chavasse, R. J., Booth, K. A., Angeles, M. & Weir, F. J. The neorule: a new instrument to measure linear growth in preterm infants. Arch. Dis. Child Fetal Neonatal Ed. 89, 360–363 (2004).
Clark, R. H., Olsen, I. E. & Spitzer, A. R. Assessment of neonatal growth in prematurely born infants. Clin. Perinatol. 41, 295–307 (2014).
Bennette, C. & Vickers, A. Against quantiles: categorization of continuous variables in epidemiologic research, and its discontents. BMC Med. Res. Methodol. 12, 21 (2012).
Acknowledgements
The authors gratefully acknowledge the Canadian Neonatal Network for data support.
Funding
This study was supported by the 2022 Research Institute of the McGill University Health Centre Studentship in Child Health Research (L.L.C.N.); Canadian Institute of Health Research Institute of Human Development, Child and Youth Health (M.-E.B.); Fonds de Recherche du Quebec (M.-E.B.); and Montreal Children’s Hospital Foundation (M.-E.B.). None of the funding agencies above had any role in the design or conduct of the study.
Author information
Authors and Affiliations
Contributions
M.B. conceptualized and designed the study, provided administrative and material support, provided support for statistical analysis and interpretation of data, critically reviewed the manuscript for important intellectual content, and supervised the entirety of the study. L.L.C.N. conceptualized and designed the study, collected data, performed statistical analysis and interpretation of data, drafted the initial manuscript, and critically reviewed the manuscript for important intellectual content. S.P. coordinated the data collection, performed statistical analysis and interpretation of data, and critically reviewed the manuscript for important intellectual content. M.-E.B., H.P., and G.S. interpreted the data and critically reviewed the manuscript for important intellectual content. A.L. and V.B. provided administrative and material support and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li Ching Ng, L., Patel, S., Plourde, H. et al. The association between BMI trajectories and bronchopulmonary dysplasia among very preterm infants. Pediatr Res 93, 1609–1615 (2023). https://doi.org/10.1038/s41390-022-02358-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02358-4
This article is cited by
-
Does faster weight trajectory lead to improved neurodevelopmental outcomes in ELBW infants with bronchopulmonary dysplasia?
Journal of Perinatology (2024)
