
Abstract
Background
Infant adiposity is linked to both high maternal fat mass (FM) and excessive gestational FM gain, whereas the association with maternal adipokines is less clear. The aim was to determine how levels of maternal leptin, the soluble leptin receptor (sOB-R), adiponectin, and FM during pregnancy were linked to infant FM in normal-weight (NW) women and women with obesity (OB).
Methods
Body composition and serum levels of leptin, adiponectin, and sOB-R were determined three times during pregnancy in 80 NW and 46 OB women. For infants, body composition was measured at 1 and 12 weeks of age.
Results
Maternal leptin and sOB-R levels increased during pregnancy. For NW women, infant FM at 1 week was inversely associated with changes in maternal leptin and at 12 weeks inversely associated with absolute maternal sOB-R levels throughout pregnancy, as well as changes in sOB-R levels in early pregnancy. For OB women, infant FM at both 1 and 12 weeks were best explained by maternal FM.
Conclusions
Leptin and sOB-R, thought to regulate leptin bioavailability, are associated with fat accumulation in infants born to NW women. In OB women, maternal FM in early pregnancy is more important than leptin in determining infant fat accumulation.
Impact
-
In normal-weight women, the regulation of maternal leptin bioavailability during pregnancy has a role in infant fat mass accumulation.
-
In women with obesity, however, pre-pregnancy maternal fat mass seems more important for infant fat mass.
-
This is the first study of maternal adipokines and fat mass including longitudinal measurements in both mothers and their children.
-
Understanding the relationship between maternal factors and infant fat mass is of great importance as obesity is programmed over the generations, and it is important to learn what regulates this programming.
Similar content being viewed by others


Introduction
Obesity is thought to be programmed in utero. Evidence from human and animal studies suggests that the programming of adiposity in the fetus is at least partly environmental.1,2,3 Maternal obesity and excessive gestational weight gain have each been linked to offspring adiposity, both during infancy and later in life.1,4 Dysregulation of adipokines in the mother during pregnancy is also thought to predispose the offspring to obesity; however, the precise associations between adipokines and infant fat mass remain unclear.5,6,7
Pregnancy involves major maternal metabolic changes, including changes in fat mass and the secretion of adipokines such as leptin and adiponectin, and also in the soluble leptin receptor (sOB-R) thought to regulate leptin bioavailability and leptin resistance through delayed leptin clearance and decreased leptin transport across the blood–brain barrier.7,8,9,10 Both leptin and adiponectin have been suggested to be involved in the programming of fetal metabolic pathways.6,7 Potential mechanistic explanations are that maternal leptin and adiponectin have regulatory effects on placental nutrient transport, and that alterations in maternal leptin signaling may predispose the fetus for leptin resistance and program neurogenic appetite pathways during organogenesis.11 Findings of previous human studies looking at the relationship between maternal serum leptin or adiponectin and neonate fat mass at birth as measured by sum of skinfold thickness9,12,13,14 or by air-displacement plethysmography (ADP)15,16 have, however, been inconsistent. The relationship between maternal serum leptin and measures of infant fat mass has been shown to be either positive,9,12 negative,13 or non-significant.9,16,17 One reason for these discrepancies is that many studies have not adequately addressed the impact of variations in maternal body mass index (BMI). It is already known that there are large differences in leptin, s-OB-R, and adiponectin levels during pregnancy in women of normal-weight and women with obesity, and that pregnancy induced changes of these adipokines also vary between these two groups.8,9 Furthermore, obesity is typically characterized by a state of leptin resistance. It therefore follows that associations between adipokines and infant fat mass may differ according to maternal body composition. Indeed, studies have pointed to differential effects of leptin and adiponectin on infant/child adiposity according to the pre-gestational BMI of the mother.9,12 Only one previous study investigating infant fat mass has included measurements of maternal sOB-R levels and free leptin index (FLI) during pregnancy to provide information on leptin bioavailability and leptin resistance.9 Results showed that associations of maternal adipokines with newborn weight, length, and sum of skinfold measurements differed depending on the BMI of the mother. These findings have yet to be confirmed in a study using a more accurate method for assessing infant fat mass (such as ADP), and at later time points. Furthermore, the release of adipokines may not be the only effect of maternal adipose tissue on the fetus; there are likely other influences on the placenta, fetal growth, and fetal programming from excess adiposity such as higher nutrient availability and an elevated inflammatory state.11 It is therefore of importance to include maternal fat mass measurements in models studying the effect of adipokines. No study to date has looked at the relationships between both longitudinal adipokine and fat mass measurements during pregnancy and longitudinal measurements of infant fat mass after birth.
The primary aim of this prospective study was to determine the relationship between levels and changes in both maternal adipokines and fat mass during pregnancy, and fat mass in infants at 1 and 12 weeks after birth, and to determine how maternal obesity was associated with this relationship.
Materials and methods
Ethical approval
The study was approved by the ethics committee at the University of Gothenburg (Dnr 402-08). Informed written consent was obtained from all women participating in the study. Both parents received oral and written information about the study and gave informed written consent before enrollment of their children.
Study design
Subjects
Normal weight (NW: BMI 18.5–24.9 kg/m2) and obese (OB: BMI ≥ 30 kg/m2) pregnant women aged 20–45 years were recruited from six antenatal health units within the Gothenburg area as part of the PONCH study, as previously described.8,18 BMI based on self-reported weight and height at the start of pregnancy was used for inclusion purposes, but these data were not used in any analyses. Exclusion criteria were diabetes, use of neuroleptic drugs, non-European descent, and vegetarianism or veganism. The women attended study visits at the Sahlgrenska University Hospital each trimester (weeks 8–12 (trimester one, T1), 24–26 (two, T2), and 35–37 (three, T3)) during pregnancy. At the third trimester visit, the parents were asked whether they wanted their child to be included in the study after birth; those who agreed were entered into the current mother–child study. NW women were all recruited at or before the T1 visit, whereas later inclusion was allowed for OB women. An overview of maternal and child visits is presented in Fig. 1.

Study visits and participating numbers for normal-weight women (n = 80) or women with obesity (n = 46) and their infants. ADP air displacement plethysmography, NW women of normal weight, OB women with obesity.
Children were divided into groups corresponding to the category assigned to their mother (NW or OB; Fig. 1). A flow-chart of the entire PONCH study is included in Supplementary Fig. S1. The study is ongoing and the current manuscript is based on data from children included between April 2009 and June 2019.
Maternal measurements
Maternal pregnancy visits have been described previously.8,18 All visits occurred in the morning after an overnight fast; anthropometric measurements and blood samples were taken, and lifestyle questionnaires completed at each visit. As part of the wider study, NW and OB women were randomized into dietary intervention or control subgroups in order to explore the impact of dietary counseling;19 the intervention subgroup received dietary counseling to increase adherence to the dietary recommendations for pregnant women stated by the Swedish National Food Agency and in the Nordic Nutrition Recommendations.19 In the current study, there were no significant differences between women in the dietary intervention and control subgroups for any of the maternal outcome measures (including outcomes that are predicted to differ with a change in diet, i.e., gestational weight or fat mass gain), and members of these two subgroups were evenly distributed across the NW and OB groups. Therefore, data for the intervention/control subgroups were combined in all analyses.
Body composition was measured by ADP using the BOD POD system (software version 5.4.0; COSMED, Italy). Adjustments were made for increased hydration of fat-free mass during pregnancy in measurements made in T2 and T3, as previously described.8 The coefficient of variation from duplicate measurements on our equipment in 22 individuals was 2.4%. Weight was measured by the BOD POD system using a Tanita BWB-627-A electronic scale. BMI was calculated from weight at T1 visit. For women recruited in T2 or T3, weight in T1 was taken from medical records for maternity care visits at gestational weeks 8–12 (n = 11). For a short period of time during the study, the BOD POD was not functional and some ADP measurements were missed (Fig. 1).
Leptin and adiponectin were analyzed at the Clinical Chemistry Laboratory, Sahlgrenska University Hospital (accredited in accordance with the International Standard ISO 15189:2007). Leptin (Human Leptin Quantikine, R&D Systems, Minneapolis, MN; interassay coefficient of variation, 8.0% at 9 μg/l), the soluble leptin receptor (sOB-R) (Human Leptin R Quantikine, R&D Systems) and adiponectin (Human Adiponectin ELISA kit, Millipore, Billerica, MA; interassay coefficient of variation, 7.0% at 10.5 mg/l) were analyzed using enzyme-linked immunosorbent assay. FLI was calculated as the ratio of leptin (ng/ml) to sOB-R (ng/ml).20,21 Serum samples were missing from some visits (Fig. 1) owing to technical difficulties during blood sampling or insufficient sample volume.
Infant anthropometric measurements
Birth weight and length were collected from medical records, and expressed in kg and cm, respectively, as well as in standard deviation scores (SDS) relative to data from healthy infants born in Sweden from 1990 to 1999.22 Study visits were made at 1 week (4–10 days) and 12 weeks (80–90 days) after birth. There were no differences between NW and OB groups in mean age at postnatal visits. Due to the short time intervals for each visit accepted within the protocol, some visits were missed. At 1 week, the most common reason for a missed visit was that the mother had not fully recovered after delivery. Measurements were not made if infants were unwell: contributing to some missing data at 12 weeks. The reason for study drop-out at the 12-week visit was otherwise generally lack of time.
Infant weight, fat mass (in kg, FMkg, and as a % of body weight, FM%), and fat-free mass (in kg, FFMkg) were measured by ADP using the PEA POD (software version 3.3.0; COSMED, Italy). The infants wore a tight swim cap, but were otherwise naked during measurements. Length was measured to the nearest 0.5 cm using a length board. At each visit, mothers were asked whether they were fully, partly, or not breastfeeding.
Study outcome and explanatory variables
The main outcome measure was infant FMkg. The secondary outcome measures were infant FM%, FFMkg, weight, and height. The explanatory variables were maternal FMkg, FM%, leptin, adiponectin, sOB-R, and FLI.
Statistical methods
The statistical methods and analyses were planned a priori and described in a statistical analysis plan. Categorical variables were expressed as number and percentage, and continuous variables were expressed as mean (standard deviation, SD). Differences between NW and OB groups with respect to ordered categorical variables were assessed using the Mantel–Haenszel chi-square test; between-group differences for continuous variables were assessed using a t-test. Within-group comparisons for continuous variables were made using Student’s t-test. Associations between maternal measurements during pregnancy and infant measurements at weeks 1 and 12, as well as changes from week 1 to 12, were analyzed using linear regression models. The diagnostic plots for residuals were reviewed and found satisfactory regarding assumptions of normality and homoscedasticity. Analyses were performed separately for NW and OB groups due to suspected interaction effects based on results from previous studies,9,12 and the magnitude of between-group differences in the levels of certain explanatory variables. Adjustments were made for maternal BMI at T1, gestational age, sex and breastfeeding at the time of infant measurements. Maternal measurements at T1, T2, T3, the change from T1 to T2 (early change), and the change from T2 to T3 (late change) were analyzed as explanatory variables. Least-square (LS) means with 95% confidence intervals (CI) have been presented from these analyses, with associated P values and R2. Stepwise multivariable linear regression was used to identify the strongest associations between maternal characteristics and infant outcomes. Beside unstandardized parameter estimates, the ones standardized for 1SD both for explanatory variables and outcome measurements were obtained to enable comparison of the magnitudes of different associations. As a post hoc analysis interaction between the strongest association variable and the infant’s sex was investigated for FMkg and FM% at 12 weeks.
Imputation was not used to handle missing data. Failure analyses were conducted to explore maternal characteristics associated with missing infant outcome data at postnatal weeks 1 and 12 among NW and OB mothers (Supplementary Table 1).
All tests were two-tailed and conducted at a 0.05 significance level. Due to the exploratory and descriptive nature of the study, no adjustments were made for multiplicity. No tests were interpreted as confirmatory. The upper limit of false significances was calculated based on Eklund–Seeger’s algorithm α/(1 − α)*(N−n(α)), where α = 0.05, N = number of tests performed, and n(α) = number of significant results. For the main study outcome presented in the conclusions for the NW group, FMkg fat accumulation over 12 weeks of age was explained by sOB-R, the number of tests was 30, the number of significant results was 4, and the upper limit for number of false significances of those 4 was 1.4. For the OB group the corresponding significant results for FMkg accumulation over 12 weeks explained by mother’s early fat mass and adiponectin levels might be due chance. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, US).
Results
Infant body composition at 1 and 12 weeks of age
Infants born to OB women were significantly longer and heavier at birth than infants born to NW women (Table 1). At 1 week of age, infants born to OB women remained longer and heavier, and had a higher fat mass, both in absolute terms (FMkg) and as a percentage of body mass (FM%), than their NW counterparts. At 12 weeks of age, infants born to OB women were still longer than infants born to NW women, but there was no significant difference in weight (SDS) or fat mass between the groups. Infants born to OB women were breastfed to a lesser degree than infants born to NW women.
Maternal body composition and adipokine levels
Body weight increased significantly in each trimester in both NW and OB women (Table 2). Despite a lower gestational weight gain in OB compared with NW women, more OB women gained weight excessively according to Institute of Medicine recommendations (Table 1). Absolute fat mass (FMkg) increased significantly during pregnancy in NW women, but not in OB women; this resulted in an increased FM% in NW women compared with T1 and a decreased FM% in OB women (Table 2). Changes in adipokine levels also differed between groups. Leptin and sOB-R levels increased between T1 and T2 in both groups; however, after this time point, sOB-R levels decreased in NW women but continued to increase in OB women. The FLI (i.e. the ratio between leptin and sOB-R) was low during T1 in NW women and remained stable during early and mid-pregnancy with a small increase between T2 and T3. In contrast, in OB women with higher FLI than in NW women in all trimesters, FLI decreased from T1 to T2, and remained lower at T3 than in T1. Adiponectin levels were higher in NW women than in OB women during T1 and decreased in both groups at different time points, from T1 to T2 in OB women and from T2 to T3 in NW women; a numerically smaller decrease was seen for OB women than for NW women.
Infant fat mass in relation to maternal adipokine levels and fat mass during pregnancy
Maternal fat mass and adipokine variables explaining a significant amount of the variation in infant FMkg are shown in Table 3 (for other infant outcomes see Supplementary Tables S2–S6). For NW women, higher values of infant FMkg at 1 week were explained best by the greater decrease in leptin concentration between T2 and T3; for OB women, this variable was explained by maternal fat mass (FMkg and FM%) at T3 showing a positive correlation. At 12 weeks, higher infant fat mass in NW women was explained by lower sOB-R concentration in T2 and T3, as well as by a smaller change in sOB-R levels between T1 and T2. In OB women, infant fat mass at 12 weeks was best explained by high maternal fat mass at T2.
In NW women, greater increases in infant fat mass between 1 and 12 weeks were explained by lower sOB-R levels at all trimesters, and the smaller change in sOB-R levels between T1 and T2. In OB women, the change in fat mass between 1 and 12 weeks was explained by lower adiponectin levels in T3.
Although the analyses presented were adjusted for breastfeeding, our data showed no significant association between breastfeeding up to 12 weeks of age and infant outcome measures (FMkg and FM% at 12 weeks) in either of the NW or OB groups, R2 ≤ 0.01.
Multivariable regression models for the association between maternal adipokine levels and fat mass, and infant fat mass
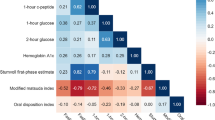
The strongest independent maternal explanatory variables (with SD-adjusted estimates) for infant outcomes using adjusted stepwise linear regression are summarized in Fig. 2. In NW women, the strongest explanatory variable for infant FMkg, FFMkg, and weight at 1 week was the change in maternal leptin concentration between T2 and T3, and for infant length it was independently the change in leptin between T2 and T3 and change in leptin between T1 and T2. At 12 weeks, however, the strongest explanatory variable for infant FM%, FMkg and weight was the change in maternal sOB-R between T1 and T2. The highest R2, ranging between 0.20 and 0.23, and most pronounced estimates expressed per 1SD increase, were obtained for FM% at 12 weeks and change in FM% from 1 to 12 weeks.

The strongest explanatory variables of infant outcomes at 1 and 12 weeks using adjusted stepwise linear regression for the a normal weight (NW) group and b obese (OB) group. Estimates per 1 SD increase and 95% CI are shown to allow comparison between different variables and outcomes. FM fat mass, FFM fat-free mass, sOB-R soluble leptin receptor, T1 trimester 1, T2 trimester 2, T3 trimester 3.
In OB women, the strongest models for infant outcomes generally included maternal fat mass or adiponectin levels. Infant fat mass (FMkg and FM%) at 1 week was best explained by maternal FMkg and FM%, respectively, at T3, and infant FFMkg and weight at 1 week were best explained by maternal FMkg at T1. The model for infant length at 1 week included two independent variables: maternal sOB-R at T3 and FMkg at T1. At 12 weeks, infant FMkg, weight, and length were best explained by maternal FMkg at T2, T3, and T1, respectively. Infant FM% at 12 weeks and change in FMkg from 1 to 12 weeks were both best explained by maternal adiponectin concentration at T3. The analysis of length SDS at week 1 had the highest R2 of 0.47. Moreover, the highest standardized estimates observed were for FMkg at T1 explaining infant length at weeks 1 and 12.
At 12 weeks, no significant model was found for infant fat-free mass in either NW or OB women. No significant interaction between the maternal variable with the strongest independent association with infant sex was observed for FMkg and FM% at 12 weeks (post hoc analysis, data not shown).
Discussion
Our findings lead us to propose a role in normal-weight pregnancies for the sOB-R in determining infant fat accumulation in the first 3 months after birth owing to its actions as a regulator of leptin bioavailability. The most striking observation in NW women was that large increases in maternal sOB-R concentration early in pregnancy, and high sOB-R concentrations in each trimester were associated with lower infant fat accumulation after 1 week of age resulting in a lower infant fat mass at 12 weeks of age. This was the case irrespective of whether or not the model was adjusted for confounders. We found no relationship between absolute leptin concentration and infant fat mass at 1 or 12 weeks of age for either NW or OB women. Change in leptin concentration, however, seemed important in NW women, with negative associations being seen with infant fat mass, fat-free mass, weight and length at 1 week of age. For OB women, on the other hand, high maternal fat mass and low adiponectin levels were the main explanatory factors for infant fat mass early in life. Findings suggest that the relationship between maternal adipokines and infant fat mass differs according to maternal BMI.
Pregnancy is associated with an increased inflammatory response, increased leptin levels, and decreased adiponectin levels, all of which have been suggested to be of importance for fetal growth and fetal programming.11 Human studies have shown these factors to be important regulators of placental nutrient transport and therefore fetal growth. Obesity, which already before pregnancy infers higher adipose-tissue-derived inflammation and leptin levels and lower adiponectin levels, is associated with increased placental nutrient transport capacity. This results in increased fetal growth and a greater frequency of infants born large for gestational age.11 Furthermore, altered leptin signaling in utero has been suggested to predispose the fetus to leptin resistance, resulting in metabolic consequences after birth.23 Effects on growth and adiposity after birth have also been observed in animal studies which have shown that neonatal leptin surges can increase the hypothalamic nerve terminals in the offspring and alter their appetite regulation.24 We have previously shown not only large differences in absolute values in adipokines between NW and OB women, but also that the timing and magnitude of changes in leptin, the soluble leptin receptor and adiponectin during pregnancy differ in NW and OB women. It is therefore of interest to examine both the relationship of absolute adipokine values and adipokine changes early and late in pregnancy with fetal growth.
The bioavailability and transport/activity of leptin is believed to be at least partly regulated by its soluble receptor, sOB-R, which we have previously shown to be upregulated between T1 and T2 in both NW and OB women.8 This upregulation resulted in a constant FLI (ratio of leptin to sOB-R) in NW women during pregnancy and a decreased FLI in OB women as pregnancy progressed. In the present study we show that sOB-R levels, and early increases in sOB-R levels during pregnancy, are associated with accumulation of infant fat mass between 1 and 12 weeks of age in children born to NW women. The upregulation of sOB-R in pregnancy is believed to regulate leptin availability both centrally and peripherally at the placental level.7 Leptin, as discussed, acts as a regulator of nutrient transport across the placenta and may effect metabolic and appetite programming during fetal organogenesis. Our results suggest that this action by leptin during pregnancy might be determined by the upregulation of circulating sOB-R in healthy normal-weight women. In women with obesity, however, there is an underlying obesity-related leptin resistance which differs from the pregnancy-induced resistance and is probably not driven by sOB-R.5 Furthermore, placentas from mothers with obesity express lower amounts of the membrane-bound form of the leptin receptor (OBRb), affecting placental leptin action.25 These findings could explain why the effect of leptin and its bioavailability seems less important for fetal growth and programming in women with obesity compared to normal-weight women.
Only one previous study investigated the relationship between maternal sOB-R and infant fat mass.9 Hinkle et al. found a positive association between sOB-R levels and neonate sum of skinfold thickness in normal-weight plus overweight women when adjusting for BMI, but the association was reversed in women with obesity. In our study, there was no association between sOB-R levels in NW pregnant women and infant fat mass at the early infant time point, but there were consistently negative associations at 12 weeks. There are several differences between the studies which make them difficult to compare. While Hinkle et al. only assessed infants at birth, our study reported body composition measurements at 1 and 12 weeks after birth. The two studies also used different methods to assess body composition; the present study used ADP which is widely accepted to be a more accurate method for assessing infant fat mass than the neonatal skinfold thickness measurements used by Hinkle et al. Furthermore, the ethnicity and division into BMI categories of the study populations differed between studies. The associations found between maternal sOB-R and infant fat mass gain between 1 and 12 weeks (and infant fat mass in absolute values at 12 weeks) in the current study could either mean that: (1) any influence of sOB-R on fetal fat mass is only important for fat accumulation after birth or (2) associations are only visible at the 12-week time point because of a larger spread in the fat mass outcome at 12 weeks (compared with 1 week), with differences only starting to show at that point. Intriguingly, if the first assumption is true, i.e., that maternal leptin regulation/bioavailability during pregnancy is important for infant mass accretion after birth, it would tie in with previous literature suggesting that maternal leptin action is important for programming of offspring energy metabolism and appetite after birth.5,11
The few studies that have investigated the association between maternal adiponectin levels and infant adiposity have all been performed at birth, with varying results.9,14,16,26 Hinkle et al. showed that there was no correlation between adiponectin levels and infant sum of skinfold in a combined group of normal weight and overweight women, but that there was an inverse correlation between these variables in women with obesity. In the current study, we also found an inverse correlation between maternal adiponectin late in pregnancy and infant body fat percentage for the children of OB women, although this was only observed at 12 weeks after birth. Adiponectin was lower in OB than in NW and is further reduced during pregnancy, i.e., we saw an association with adiponectin when the levels were very low. Maternal adiponectin has been suggested to reduce nutrients available for the fetus (by increasing maternal insulin sensitivity) and to reduce mTORC and insulin/IGF-I signaling in the placenta, resulting in reduced fetal growth.27 Our data might suggest that this signaling is particularly important when adiponectin levels are low (i.e. in our case this means in OB women towards the end of pregnancy). Furthermore, as discussed for sOB-R in NW above, the data for adiponectin in OB women indicate that maternal levels are most important for infant fat mass accretion between 1 and 12 weeks, again leading to speculation that maternal adipokines might influence infant energy metabolism after birth through fetal programming.
An interesting difference between BMI groups was that maternal leptin or sOB-R levels were the most important explanatory variables for all infant measurements (fat mass, fat-free mass, weight, and length) in NW women, whereas for OB women, maternal fat mass was the main explanatory variable in most cases. No previous studies have looked at both maternal fat mass and adipokines in relation to infant outcomes, and one can only speculate about the differences in regulation of infant fat mass between NW and OB women. One explanation for the observed differences between BMI groups in this study could be the leptin resistance in obesity, and that leptin exerts its effects mainly when fat depots are low,28 as is the case in NW individuals. This could also explain inconsistencies between studies in terms of the relationship between maternal leptin and infant weight/fat mass. In fact, studies that have separated women into groups based on BMI have typically found different results in overweight or obese compared with normal-weight mothers.9,12,29,30 In contrast, results for adiponectin are largely consistent across studies. Generally, studies report either a negative association or no relationship between adiponectin and infant measures of fat mass. Nutrient transport over the placenta and thereby fetal growth is regulated, not only by adipokines, but also by cytokines and circulating nutrients. High levels of fat mass are linked to high levels of circulating inflammatory cytokines and free fatty acids, which together with adiponectin could have a larger impact than leptin on the regulation of placental transport in OB women who are already leptin resistant before pregnancy.11 It is also interesting that associations with infant anthropometry for OB women in the current study were consistently related to absolute levels of fat mass and not to changes in fat mass, indicating that pre-pregnancy fat mass is more important for infant outcomes than changes in fat mass during pregnancy This is in agreement with prior studies showing that gestational weight gain is not related to infant fat mass and that lifestyle interventions during pregnancy have little effect on fetal outcome.4 The explanation why absolute levels of maternal fat mass is of such high importance for fetal fat mass, as seen in our OB group, has been suggested to be the inflammatory state in combination with over nutrition by excess circulating metabolites (i.e. free fatty acids, amino acids, glucose) associated with high adiposity.4 Placentas from mothers with obesity show several differences compared to those of normal-weight mothers; factors believed to be particularly important to fetal growth are increased expression of system A amino acid transporters 1 and 2 and higher activity of the mTOR and IGF-I signaling pathways.31
The PONCH study is a well-controlled study with visits performed at a single center using consistent procedures for blood sampling, and reference methods to measure body composition in a homogeneous and well-characterized population. The inclusion of longitudinal data from both mothers and children is a clear strength of the study. Body composition is known to go through marked changes during infancy, with body fat percentages doubling between 1 and 12 weeks of age.32,33 Changes during the first 3 months of life are of particular interest because rapid weight gain in this period, which is largely due to changes in fat mass, is associated with being overweight and having a high degree of adiposity in childhood,34 and is linked to metabolic risk in early adulthood.35 In our study we obtained both a measure of intrauterine growth (1 week) and infant growth during the important first few months of life (12 weeks). Interestingly, when we considered changes in infant weight/length ratio or BMI as outcome variables, we did not find associations with maternal adipokines (data not shown), highlighting the importance of using accurate methods to assess infant fat mass.
One limitation of using such a homogeneous study group is applicability to other populations. Another possible limitation is that we did not assess adipokine levels in the breast milk of participating mothers; breast milk is known to contain adipokines that can affect adiposity in infants. On the other hand, we did have reliable data on breastfeeding which allowed us to adjust for whether the infant was fully, partly, or not breast fed. Furthermore, serum and body composition measurements were missing for a number women due to either technical issues or later study inclusion (OB women only), which reduced the statistical power for the analysis particularly at T1 in OB women. As with other similar studies, the design was observational, which limited the ability to draw conclusions regarding cause and effect. We chose not to analyze all women together because maternal adipokines levels and fat mass during pregnancy were numerically very different in the NW and OB populations. The results obtained, with changes apparent in different directions when analyses were performed separately on the NW and OB groups, confirmed that statistics should be performed by strata rather than on the total cohort. However, this stratification led to even smaller group sizes, especially for OB mothers, lowering the power for identifying relationships between variables. Lastly, our longitudinal design illustrated how the investigation of maternal factors during all three trimesters of pregnancy shed more light on possible interactions than using only one time point.
In conclusion, our results suggest that in healthy pregnancies in normal-weight women, sOB-R may be involved during intrauterine fetal programming of infant fat accumulation over the first 3 months of life. In women with pre-pregnancy obesity and a pre-existing state of leptin resistance, however, our data indicate that the level of maternal fat mass early in pregnancy together with adiponectin levels may play a more important role in infant fat mass accumulation. In future studies, our longitudinal study design will allow us to follow the children at older ages to assess whether weight and fat mass gain continue to be linked to maternal leptin bioavailability, adiponectin, and fat mass in a similar pattern as for the first 3 months of life.
References
Godfrey, K. M. et al. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. 5, 53–64 (2017).
Patel, N., Pasupathy, D. & Poston, L. Determining the consequences of maternal obesity for offspring health. Exp. Physiol. 100, 1421–1428 (2015).
Smith, J. et al. Effects of maternal surgical weight loss in mothers on intergenerational transmission of obesity. J. Clin. Endocrinol. Metab. 94, 4275–4283 (2009).
Catalano, P. M. & Shankar, K. Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ 356, j1 (2017).
Briffa, J. F., McAinch, A. J., Romano, T., Wlodek, M. E. & Hryciw, D. H. Leptin in pregnancy and development: a contributor to adulthood disease? Am. J. Physiol. Endocrinol. Metab. 308, E335–E350 (2014).
Briana, D. D. & Malamitsi‐Puchner, A. The role of adipocytokines in fetal growth. Ann. NY Acad. Sci. 1205, 82–87 (2010).
Tessier, D., Ferraro, Z. & Gruslin, A. Role of leptin in pregnancy: consequences of maternal obesity. Placenta 34, 205–211 (2013).
Andersson-Hall, U. et al. Longitudinal changes in adipokines and free leptin index during and after pregnancy in women with obesity. Int. J. Obes. 44, 675–683 (2019).
Hinkle, S. N. et al. Maternal adipokines longitudinally measured across pregnancy and their associations with neonatal size, length, and adiposity. Int. J. Obes. 43, 1422–1434 (2018).
Briana, D. D. & Malamitsi-Puchner, A. Reviews: adipocytokines in normal and complicated pregnancies. Reprod. Sci. 16, 921–937 (2009).
Howell, K. R. & Powell, T. L. Effects of maternal obesity on placental function and fetal development. Reproduction 153, R97 (2017).
Patenaude, J. et al. Associations of maternal leptin with neonatal adiposity differ according to pregravid weight. Neonatology 111, 344–352 (2017).
Valsamakis, G. et al. Neonatal birth waist is positively predicted by second trimester maternal active ghrelin, a pro-appetite hormone, and negatively associated with third trimester maternal leptin, a pro-satiety hormone. Early Hum. Dev. 90, 487–492 (2014).
Lowe, L. P. et al. Inflammatory mediators and glucose in pregnancy: results from a subset of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. J. Clin. Endocrinol. Metab. 95, 5427–5434 (2010).
Josefson, J. L., Zeiss, D. M., Rademaker, A. W. & Metzger, B. E. Maternal leptin predicts adiposity of the neonate. Horm. Res. Paediatr. 81, 13–19 (2014).
Castro, N. et al. The relationship between maternal plasma leptin and adiponectin concentrations and newborn adiposity. Nutrients 9, 182 (2017).
Brunner, S. et al. Effect of reducing the n‐6/n‐3 fatty acid ratio on the maternal and fetal leptin axis in relation to infant body composition. Obesity 22, 217–224 (2014).
Svensson, H. et al. Body fat mass and the proportion of very large adipocytes in pregnant women are associated with gestational insulin resistance. Int J. Obes. 40, 646–653 (2016).
Bosaeus, M. et al. A randomized longitudinal dietary intervention study during pregnancy: effects on fish intake, phospholipids, and body composition. Nutr. J. 14, 1 (2015).
Ingelsson, E. et al. Circulating ghrelin, leptin, and soluble leptin receptor concentrations and cardiometabolic risk factors in a community-based sample. J. Clin. Endocrinol. Metab. 93, 3149–3157 (2008).
Kratzsch, J. et al. Circulating soluble leptin receptor and free leptin index during childhood, puberty, and adolescence. J. Clin. Endocrinol. Metab. 87, 4587–4594 (2002).
Niklasson, A. & Albertsson-Wikland, K. Continuous growth reference from 24th week of gestation to 24 months by gender. BMC Pediatr. 8, 8 (2008).
Bouret, S. Nutritional programming of hypothalamic development: critical periods and windows of opportunity. Int. J. Obes. Suppl. 2, S19–S24 (2012).
Yura, S. et al. Role of premature leptin surge in obesity resulting from intrauterine undernutrition. Cell Metab. 1, 371–378 (2005).
Farley, D. et al. Placental amino acid transport and placental leptin resistance in pregnancies complicated by maternal obesity. Placenta 31, 718–724 (2010).
Mohamad, M., Lim, P., Wang, Y., Soo, K. & Mohamed, H. Maternal serum and breast milk adiponectin: the association with infant adiposity development. Int. J. Environ. Res. Public Health 15, 1250 (2018).
Aye, I. L., Powell, T. L. & Jansson, T. Adiponectin—the missing link between maternal adiposity, placental transport and fetal growth? Placenta 34, S40–S45 (2013).
Harris, R. B. Direct and indirect effects of leptin on adipocyte metabolism. Biochim. Biophys. Acta 1842, 414–423 (2014).
Misra, V. K., Straughen, J. K. & Trudeau, S. Maternal serum leptin during pregnancy and infant birth weight: the influence of maternal overweight and obesity. Obesity 21, 1064–1069 (2013).
Perichart-Perera, O. et al. Metabolic markers during pregnancy and their association with maternal and newborn weight status. PLoS ONE 12, e0180874 (2017).
Jansson, N. et al. Activation of placental mTOR signaling and amino acid transporters in obese women giving birth to large babies. J. Clin. Endocrinol. Metab. 98, 105–113 (2013).
Eriksson, B., Lof, M. & Forsum, E. Body composition in full-term healthy infants measured with air displacement plethysmography at 1 and 12 weeks of age. Acta Paediatr. 99, 563–568 (2010).
Andersson-Hall, U. K. et al. Maternal obesity and gestational diabetes mellitus affect body composition through infancy: the PONCH Study. Pediatr. Res. 85, 369–377 (2018).
Young, B. E., Johnson, S. L. & Krebs, N. F. Biological determinants linking infant weight gain and child obesity: current knowledge and future directions. Adv. Nutr. 3, 675–686 (2012).
Leunissen, R. W., Kerkhof, G. F., Stijnen, T. & Hokken-Koelega, A. Timing and tempo of first-year rapid growth in relation to cardiovascular and metabolic risk profile in early adulthood. JAMA 301, 2234–2242 (2009).
Acknowledgements
We would like to thank all participating women of the PONCH study, and registered dietician Evelina Järvinen for expert care and measurements during study visits. This work was supported by grants from the Emil and Wera Cornell Foundation, the Swedish Research Council (12206), the Swedish Diabetes Association Research Foundation (2015-08), and the Swedish state under the agreement between the Swedish government and the country councils, the ALF-agreement (ALF-GBG-720851, 719041 and 812951).
Author information
Authors and Affiliations
Contributions
Conception, data acquisition, or data analysis and interpretation: U.K.A.-H., A.P., H.K.d.M., J.P.S., and A.B.H. Drafting or revising article for intellectual content: U.K.A.-H., E.C.M., K.G.A.-W., and A.B.H. Final appoval of article: U.K.A.-H., A.P., H.K.d.M., J.P.S., E.C.M., K.G.A.-W., and A.B.H.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was approved by the ethics committee at the University of Gothenburg (Dnr 402-08). Informed written consent was obtained from all women participating in the study. Both parents received oral and written information about the study and gave informed written consent before enrollment of their children.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Andersson-Hall, U.K., Pivodic, A., de Maré, H.K. et al. Infant body composition relationship to maternal adipokines and fat mass: the PONCH study. Pediatr Res 89, 1756–1764 (2021). https://doi.org/10.1038/s41390-020-01115-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-01115-9
