
Abstract
Background/objectives
Findings from epidemiological studies showed controversial findings between dietary sugar intake and the development of diabetes. Most of these studies assessed dietary sugar intake by self-reports which might be prone to bias. Urinary sucrose, an objective biomarker of sucrose intake, might provide better insights into this association. Thus, the aim of this study was to investigate the associations between sucrose intake, measured via self-reports and urinary sucrose, with incident diabetes and to detect the impact of obesity on this association.
Subjects/methods
Data of a sub-group (n = 2996) from the prospective EPIC-Norfolk cohort were investigated. Sucrose intake was assessed by self-reports (validated food frequency questionnaire (FFQ) and 7-day diet diaries (7DD)) and as an objective urinary sucrose biomarker. Cox proportional hazard models were conducted to calculate hazard ratios (HRs) and 95% confidence intervals (CI) for the associations between urinary and dietary sucrose intake and incident diabetes. Mediation analysis was performed to investigate the mediated percentage of body mass index (BMI) and waist circumference (WC) on this association.
Results
The mean age of the participants was 60.6 ± 9.5 years and 53% were women. After a mean follow-up of 11.2 ± 2.9 years, 97 participants developed diabetes. Findings suggested inverse associations regarding incident diabetes for self-reported sucrose intake per 50 g/d via 7DD [HR: 0.63 (95% CI: 0.43, 0.91)], and a tendency via FFQ [HR: 0.81 (95% CI: 0.46, 1.42)]. Urinary sucrose indicated a positive association with incident diabetes for each increase of 100 µM [HR: 1.14 (95% CI: 0.95, 1.36)]. The proportion mediated of BMI and WC for this association was 16 and 22%.
Conclusions
These findings indicate that sucrose measured as objective urinary biomarker points to a positive association with incident diabetes. BMI might partly mediate this association. However, to obtain more precise results, more studies are warranted that consider this objective biomarker.
Similar content being viewed by others

Introduction
Type 2 diabetes (T2D) is a metabolic disease, which is caused by genetic components as well as environmental risk factors. Lifestyle factors, including healthy dietary behavior, play an important role in the development and progression of T2D [1]. There is a high certainty of evidence that high consumption of sugar-sweetened beverages is associated with an increased incidence of T2D [2,3,4]. Moreover, several observational studies investigated the association between dietary sugar intake as a nutrient and incident T2D. However, those findings were inconsistent, showing inverse [5] or null associations [6,7,8,9,10,11] for total sugar intake with T2D, as well as inverse [12] or null associations [6,7,8, 11, 13, 14] for sucrose intake. A systematic review and meta-analysis that pooled these studies, indicated an overall inverse association between a high intake of sucrose and incidence of T2D, and an inverse, but imprecisely estimated, association for total sugars [15]. The certainty of the evidence of these observations was rated as low or very low [4]. However, these findings should be interpreted with caution, in particular as in observational studies the assessment of dietary sugar intake is usually relying on self-reports of the participants using different forms of questionnaires. In general, this leads to a higher risk of bias, since individuals, especially overweight and obese individuals, tend to underreport their true intake of unhealthy—“high sugar”—foods [16, 17].
In consequence, biomarkers of sugar intake were previously used instead of questionnaire data in several studies to objectively assess dietary sugar intake, e.g. urinary sucrose and fructose. In a subsample of the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) sucrose and fructose were measured from spot urine samples, and a positive association between urinary sucrose and the development of overweight or obesity were observed, but interestingly, inverse or null associations were observed using self-reported dietary sugar intake [18, 19]. Moreover, there is an ongoing discussion, if a high dietary sugar intake contributes to an overload of calories that may lead to overweight and obesity, which is the causal risk factor for T2D [20]. However, it remains unclear, if this relationship is only influenced via the indirect pathway via overweight and obesity, or if other direct pathophysiological mechanisms also play a role. In this context, we previously conducted a global, ecological mediation analysis, which suggested that the association between per capita sugar intake and the prevalence of diabetes is mediated by the body mass index (BMI) to a large proportion, but also other mechanisms might have an influence [21]. However, the impact of BMI or waist circumference (WC) on the relation between dietary sugar intake and diabetes incidence had never been investigated in a mediation analysis by using individual data.
Thus, the aim of the present study was to investigate the mediation effect of BMI or WC on the association between dietary sugar intake assessed via urinary sucrose biomarker, food frequency questionnaire (FFQ), or 7-day diet diary (7DD) and the incidence of diabetes using prospective data from a sub-cohort of the EPIC-Norfolk study.
Participants and methods
Study participants
EPIC-Norfolk is a prospective cohort study, in which 77,630 healthy individuals at age 39–79 years were invited to participate between 1993 and 1997, of whom 25,639 attended the first health examination [18]. All participants gave signed informed consent and the study received ethical approval by the Norwich District Authority Ethics Committee.
Baseline spot urine samples were available for 6 000 participants (Fig. 1). Due to prevalent diabetes at baseline, we had to exclude 159 participants. Further, participants with missing variables on specific gravity (n = 167) or covariates (n = 65), and implausible calorie intake (n = 321) were also excluded from our analyses. Implausible values for calorie intake were defined as <500 or >3500 kcal/day for women and <800 or >4000 kcal/day for men [22]. To adjust for the urine concentration, a quotient was generated for urinary sucrose relative to specific gravity. Participants with urinary sucrose concentrations outside the acceptable range for sucrose 5–500 µM (n = 2292) were excluded from our main analysis [18]. The final study population included 2996 participants without prevalent diabetes. For sensitivity analyses, multiple imputation was performed for individuals with urinary sucrose levels outside the range of 5–500 µM. The present study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-nut) checklist [23].

Flowchart of data preparation for final study population with urinary sucrose (n = 2996).
Assessment of sucrose
Dietary sucrose intake was assessed at baseline by a 7DD and a 130-item semi-quantitative FFQ. Spot urine samples were collected at baseline health examination and analyzed for urea, creatinine, glucose, sucrose, and fructose concentration using methods previously described [18, 24]. The specific gravity of spot urine samples was measured by Multistix reagent strips (Bayer) at collection [19].
Outcome assessment
Incident diabetes was detected by self-reports of participants from follow-up health and lifestyle questionnaires, e.g. in terms of diagnosis of diabetes by a doctor or taking any antidiabetic medication. Moreover, external sources such as the general practice register, local hospital diabetes registers, hospital admissions data with screening for any diabetes-related admissions, and Office of National Statistics mortality data with coding for diabetes were consulted to receive information on the participants’ diabetes status. To consider the diagnoses as a verified case, self-reported diabetes had to be confirmed by any of the listed external sources [25].
Covariates
The covariates at baseline included in our analyses were selected a priori based on the literature and are illustrated with directed acyclic graphs in Supplementary Fig. 1. BMI or WC were used as mediators. Anthropometric data were measured according to a standardized protocol conducted by trained research nurses at baseline and a second health check (2HC) after three years [26]. Total energy intake was obtained at baseline by 7DD and FFQ, respectively. General factors and demographics, including education level, social class, smoking status, and family history of diabetes were assessed by questionnaires at baseline. The physical activity level at baseline, including occupational and leisure activity, was assessed by a validated questionnaire [27].
Statistical analysis
The associations between urinary and dietary sucrose (FFQ and 7DD) with diabetes incidence were investigated by calculating hazard ratios (HR) with 95% confidence intervals (95% CI) in Cox proportional hazard models. We tested the assumption of proportional hazards (1) by the Schoenfeld residuals method for urinary and dietary sucrose (Supplementary Fig. 2), and (2) by calculating a Kaplan–Meier Plot (Supplementary Fig. 3). In the Cox model, the time of follow-up began with recruitment (assessment of sucrose) and ended with diagnosis of incident diabetes, date of death or date of last contact (31.12.2006). We investigated log-transformed urinary sucrose (per log 100 µM) and dietary sucrose (per log 50 g/d) [15] as continuous measures and calculated quartiles for intake of sucrose from FFQ, 7DD, and urine sample, respectively, by using the first quartile as reference group.
Analyses were adjusted for age and sex (model 1), and model 2 was additionally adjusted for total energy intake from FFQ or 7DD in kcal/d, education level (none, O-level, A-level, degree), smoking status (current, former, never), physical activity level (inactive, moderately inactive, moderately active and active) and family history of diabetes (yes, no). Further adjustment for social class (professional, managerial and technical, non-manual skilled, manual skilled, partly skilled, and unskilled) did not change the results remarkably (HRs changed < 5%), and thus, it was not included in the final model. In order to investigate whether obesity influences the association between sucrose and incident diabetes, additional models were adjusted for BMI or WC plus height. To test for linear trend (pTrend) the medians of the quartiles were used as continuous variables in the corresponding models. Non-linear relations between urinary sucrose and HRs of incident diabetes were explored by generating smoothing splines. After investigating several spline functions with different degrees of freedom, we chose the splines with three degrees of freedom as the best fit.
Mediation analysis was conducted according to the method suggested by VanderWeele using the mediator package in R [28, 29], investigating the indirect effect of BMI and WC on the association between urinary sucrose and the incidence of diabetes. In general, mediation analysis aims to identify the underlying mechanism of an exposure-outcome association by dividing the total effect into a direct and an indirect effect via a third, the “mediating” variable [30]. Given a counterfactual approach, the pure direct effect (PDE) is defined as the contrast in the counterfactual outcome if a person was exposed versus the same person was not exposed, assuming that the mediator remains constant at the value it would have taken if the person had not been exposed [31]. In this study, the PDE describes the effect size of the association between exposure (urinary sucrose) and outcome (diabetes incidence), assuming that the exposure does not affect the mediator (BMI or WC). In addition, the total indirect effect (TIE) is defined as the contrast in the counterfactual outcome of the value that the mediator would have taken if the person had been exposed versus the value that the mediator would have taken if the person had not been exposed, assuming that the person was fixed to being exposed [31]. Thus, the TIE represents the effect size described by the pathway of the exposure to the outcome via the mediator (Fig. 2, Supplementary Fig. 1). In addition, the proportion mediated (PM) can be calculated as the quotient of the TIE and total effect, to determine to what extent (in %) the exposure-outcome association can be explained by the influence of the mediator.

The figure shows the potential mediation effect of body mass index (BMI) or waist circumference on the association between urinary sucrose and incident diabetes by considering potential confounders.
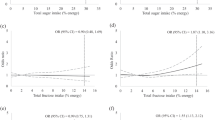
For mediation analysis, the following criteria should be fulfilled: I) the exposure (urinary sucrose intake) is associated with the outcome (diabetes incidence), II) the exposure is associated with the mediator (BMI or WC), and III) the mediator is associated with the outcome. Thus, to assess the first criterion, we conducted adjusted Cox proportional hazard models, as previously described. Further, we performed linear and logistic regression analyses to investigate the association between urinary and dietary sucrose intake and BMI or WC, respectively (criterion II). In the logistic regression models, BMI and WC were categorized as binary variables, to calculate odds ratios (OR) along with 95% CI in relation to quartiles of urinary and dietary sucrose via FFQ and 7DD, as well as log-transformed continuous urinary sucrose values. For this, individuals were divided into obese (BMI ≥ 30 kg/m2; WC ≥ 88 cm (f) and ≥ 102 cm (m)) and non-obese (BMI < 30 kg/m2; WC < 88 cm (f) and < 102 cm (m)). The third criterion was assessed by conducting Cox proportional hazard models to investigate the association between BMI or WC (continuously) and diabetes incidence.
In order to incorporate participants with urinary sucrose levels outside the detection limit in sensitivity analyses, we predicted sucrose values outside the detection range using all covariates included in the adjusted model (model 2). Participants were ordered by their predicted value and allocated to equidistant values from 0.0 to 5.0 µM for measured urinary sucrose below the detection limit and from 500 to 1000 µM for measured urinary sucrose above the detection limit, respectively. Urinary sucrose was then categorized into five groups. For the first category of urinary sucrose, the imputed values of all participants below the detection limit of 5 µM were summarized in one group (n = 2246). The remaining participants (n = 3042) with values in and above the detection limit were divided into quartiles. Moreover, in further sensitivity analyses, data on BMI and WC from 2HC after three years was included in regression and mediation analyses (n = 1728), in order to consider the time sequence of the causal pathway between sucrose intake and overweight and obesity for mediation analysis. In addition, the causal effects of the mediation analysis were estimated as a function of time to examine whether temporal variations in the hazard ratios (Q4 vs. Q1) occurred over the follow-up period [32]. All statistical analyses were performed in R 4.1.0.
Results
In this analysis, 2996 participants (mean (SD) age: 60.6 ± 9.5 years, 52.5% women) with measured urinary sucrose levels within the detection limit were included. During a mean follow-up time of 11.2 ± 2.9 years, 97 cases of incident diabetes occurred. Men tended to have higher urinary sucrose values compared to women (Table 1). In the highest quartile, participants were more likely to be older, obese, and inactive, and to have a lower education and higher energy intake compared to participants in the lower quartiles. For sensitivity analyses, 5288 participants (mean age: 60.1 ± 9.3 years, 57.4% women) were included after imputation of sucrose values outside the detection ranges, of whom 165 developed incident diabetes (Supplementary Table 1).
After the 11.2-year follow-up, results of the Cox proportional hazard models (model 2) pointed to inverse associations between dietary sucrose intake via FFQ and 7DD with diabetes incidence, and to a positive association for urinary sucrose (Table 2). Modeling sucrose as a continuous variable showed a 37% lower incidence of diabetes per 50 g/d for sucrose assessed with 7DD [HR (95% CI): 0.63 (0.43, 0.91)] and a 19%, but imprecisely estimated, lower incidence of diabetes for sucrose assessed with FFQ [HR (95% CI): 0.81 (0.46, 1.42)]. There was an indication that higher urinary sucrose levels were associated with increased incidence of diabetes in the continuous analysis [HR (95% CI) per 100 µM: 1.14 (0.95, 1.36)] and comparing fourth vs. first quartile [HR (95% CI): 1.36 (0.77, 2.41)]. After including BMI or WC as covariates into the multivariable models the associations were attenuated (Table 2). The smoothing spline indicated that the hazard ratio of incident diabetes was increasing with higher urinary sucrose levels (Fig. 3).

Smoothing splines of the association between urinary sucrose and incident diabetes before imputation (A—n = 2996) and after imputation of values of urinary sucrose levels outside the detection limit (B—n = 5228).
In the sensitivity analysis with imputed values outside the detection limits, sucrose assessed with FFQ and 7DD (per 50 g/d) was associated with a 34% [HR (95% CI): 0.66 (0.44, 0.98)] and 29% [HR (95% CI): 0.71 (0.52, 0.96)] lower hazard of developing diabetes in the adjusted model (model 2), respectively (Supplementary Table 2). Urinary sucrose per 100 µM was not associated with diabetes incidence [HR (95% CI): 1.00 (0.92, 1.08)]. However, comparing the fourth vs. first quartile of urinary sucrose pointed to an increase in T2D incidence [HR (95% CI): 1.38 (0.79, 2.42)].
Regarding the criteria for mediation analysis, urinary sucrose showed a positive association with both, BMI and WC (Supplementary Table 3). BMI and WC were also associated with diabetes incidence (Supplementary Table 4). Findings from the mediation analysis, using BMI as the mediator, pointed to an increase in the hazard of incident diabetes for the TIE [HR (95% CI): 1.02 (1.00, 1.04)] and the PDE [HR (95% CI): 1.11 (0.92, 1.35)] for urinary sucrose per 100 µM. The PM of BMI in this relation was 16%. The findings were similar, when WC was used as a mediator (WC: PM: 22%). In sensitivity analysis using BMI and WC from 2HC as mediators, findings on PDE, TIE, and total effect were comparable [BMI: TIE (95% CI): 1.02 (0.99, 1.06), PM: 10%; WC: TIE (95% CI): 1.03 (1.00, 1.07), PM: 12%] (Table 3). Plotting the causal effects estimated as a function of time showed that the HRs for diabetes incidence did not vary over the follow-up period for the PDE, TIE, and total effect (Supplementary Fig. 4).
Discussion
The findings of our study indicated inverse associations for dietary sucrose assessed via FFQ and 7DD with diabetes incidence, but a tendency to a positive association for urinary sucrose regarding incident diabetes. Results from the mediation analysis suggested that the total association between urinary sucrose and diabetes incidence might be explained by ~16% or 22% by the indirect pathway via BMI or WC. However, the effect size of the TIE is small and the PDE is imprecisely estimated. Nevertheless, it is possible that direct or other mechanisms play a role and influence this association.
Our results reflect the present body of research, indicating that the evidence for associations between dietary sugar intake and incident diabetes is inconsistent [4]. Whereas there is a high certainty of the evidence for a positive association between sugar-sweetened beverages and diabetes incidence [2,3,4], the evidence regarding dietary sugar intake as a nutrient remains inconclusive and findings are controversial [4, 15]. Similar to the findings of a systematic review and meta-analysis, in which sucrose intake was inversely associated with the incidence of T2D [15], we also found an inverse association for dietary sucrose assessed with 7DD, and an imprecisely estimated inverse association for dietary sucrose assessed with FFQ regarding the incidence of diabetes. Moreover, some studies showed that the inverse association between dietary sugar intake and diabetes incidence disappeared after adjusting for BMI [6, 8, 9]. In this study, the estimated associations were also attenuated after including BMI and WC in the adjusted Cox proportional hazard models.
The results on urinary sucrose point to a positive association regarding diabetes incidence. This observation is in line with existing studies using urinary biomarkers in adults. In feeding studies, conducted in the UK [24, 33] and USA [34], 24-hour urinary sucrose and fructose (24uSF) were used to develop a predictive objective biomarker for dietary sugar intake. A validation of the biomarker, considering different levels of specific biases, was performed to assess “unbiased” sugar intake [35]. In the Women’s Health Initiative, dietary sugar assessed by self-reports was associated with a decreased risk of T2D, but after using the calibrated intake using equations from the biomarker study, findings were attenuated towards the null [36]. Beyond that, studies investigating sugar intake and risk of obesity also found a positive association using 24uSF [37], and urinary sucrose from spot urine [18, 19], whereas self-reported dietary sugar intake was not associated with obesity. Furthermore, findings of a Swedish study showed positive associations for overnight urinary sucrose and fructose with BMI, WC, blood pressure, and plasma fasting glucose in women. However, interestingly, the urinary biomarker was inversely associated with BMI and WC in men. For self-reported dietary sugar intake, no associations were observed in this study for most of the outcomes [38]. Using BMI and WC as mediators, the findings of our study indicate that overweight and obesity may partly explain the association between sucrose intake and diabetes incidence. Here, the mediating effect of BMI was weaker compared to the findings in our ecological mediation analysis based on aggregated data [BMI: PM (95% CI): 66% (34%, 100%)] [21]. Consequently, there is an indication that direct mechanisms next to overweight and obesity might have an impact on the association between sugar intake and the development of diabetes.
The different findings regarding urinary sugar biomarkers and self-reported dietary sugar intake may be explained due to reporting bias. Dietary data is usually based on self-reports of participants using questionnaires, which is prone to bias, and especially overweight individuals tend to underreport their true intake [16, 17]. In studies that investigated differences between 24uSF as an objective urinary biomarker and self-reported dietary sugar intake, biomarker predicted sugar intake was higher than self-reported dietary sugar intake, indicating measurement errors and underreporting due to self-reports [39, 40]. Feeding studies were conducted to investigate 24uSF as a potential predictive and objective biomarker [24, 33, 34], and one of those studies reported a high correlation between 30-days mean 24uSF and 30-days mean dietary sugar intake [Spearman correlation coefficient (95% CI): 0.84 (0.54, 0.95)] [24]. Consequently, a calibration study was carried out in the Observing Protein and Energy Nutrition (OPEN) study, in order to find a reliable biomarker for objective dietary sugar assessment [35]. Yet, 24uSF was used in several cohorts [35,36,37, 39, 40], whereas, other studies were restricted to urinary sucrose or fructose from spot urine samples [18, 19, 38]. However, urinary biomarkers from spot urine sample, which was also used in our study, were not proven as objective biomarkers in calibration studies yet.
The present body of research implies that a high dietary sugar intake may lead to overweight and obesity due to an overload of calories [41], and consequently, the indirect pathway via overweight and obesity is the causal risk factor for incident T2D [42]. However, other direct sugar-related pathophysiologic mechanisms might have an impact on the association between dietary sugar intake and T2D. For instance, a high dietary sugar intake, and especially fructose intake, has been associated with increased liver fat content and non-alcoholic fatty liver disease [43, 44], which are causal risk factors for insulin resistance [45]. Beyond that, a diet high in added sugars can lead to a higher glycaemic and insulinemic response due to a higher glycaemic load [46], which is associated with an increased risk of T2D [47, 48].
Our study has several strengths and limitations. This was the first study that investigated the indirect impact and mediation effect of BMI or WC on the association between dietary sugar intake and incidence of diabetes in a prospective approach using individual data. Furthermore, different assessment methods of sucrose were available and thus, results of dietary sucrose assessed with FFQ and 7DD could be compared to urinary sucrose. However, our study had some limitations as well. First, only 97 participants developed T2D during follow-up. Due to this small number, 95% CIs were wide and thus, findings were imprecisely estimated. Consequently, these findings should be interpreted with caution. Second, a large number of participants in our study population died during the follow-up period (n = 1358). As we considered death as a censoring event for the time to incident diagnosis, we assume that time to death and time to diabetes diagnosis are independent. However, this assumption might not be fulfilled, and thus, competing risk cannot be ruled out. Third, the urinary sucrose levels of 42.5% of the participants were below and 0.9% above the detection level of 5–500 µM (n = 2292). Recent studies used other methods with a lower detection limit to assess urinary sucrose, and thus, excluded a lower percentage of their participants (~4–10%) [34, 38]. We, therefore, conducted a sensitivity analysis and imputed sucrose values outside the detection limits. However, after including these imputed values the association between urinary sucrose and incidence of diabetes was u-shaped, and thus, we cannot be sure if the measured values below the detection limit represent the true values. Fourth, urinary sucrose was only measured once and assessed via spot urine samples. Urinary sucrose from spot urine was also considered in other studies [18, 19, 38], however, no validation studies have been conducted so far, that investigated whether spot urine has the potential to predict usual sucrose intake.
Conclusions
Our findings showed that sucrose measured as objective urinary biomarker points to an increased incidence of diabetes. BMI and WC may partly mediate this association; however, it is possible that other mechanisms also play a role. More large-scale epidemiological studies considering objective sucrose biomarkers are warranted to obtain more precise results.
Data availability
The data set that supports the findings of this study cannot be made available by the authors, since they have no permission to share the data. EPIC-Norfolk researchers will make the data set available under a Data Transfer Agreement to any bona fide researcher who wishes to obtain the data set in order to undertake a replication analysis. The contact for data requests is: epic-norfolk@mrc-epid.cam.ac.uk.
References
Schlesinger S, Neuenschwander M, Ballon A, Nothlings U, Barbaresko J. Adherence to healthy lifestyles and incidence of diabetes and mortality among individuals with diabetes: a systematic review and meta-analysis of prospective studies. J Epidemiol Community Health. 2020;74:481–7.
Imamura F, O’Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, et al. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015;351:h3576.
Imamura F, Schulze MB, Sharp SJ, Guevara M, Romaguera D, Bendinelli B, et al. Estimated substitution of tea or coffee for sugar-sweetened beverages was associated with lower type 2 diabetes incidence in case-cohort analysis across 8 european countries in the EPIC-InterAct study. J Nutr. 2019;149:1985–93.
Neuenschwander M, Ballon A, Weber KS, Norat T, Aune D, Schwingshackl L, et al. Role of diet in type 2 diabetes incidence: umbrella review of meta-analyses of prospective observational studies. BMJ 2019;366:l2368.
Hodge AM, English DR, O’Dea K, Giles GG. Glycemic index and dietary fiber and the risk of type 2 diabetes. Diabetes Care. 2004;27:2701–6.
Janket SJ, Manson JE, Sesso H, Buring JE, Liu S. A prospective study of sugar intake and risk of type 2 diabetes in women. Diabetes Care. 2003;26:1008–15.
Montonen J, Jarvinen R, Knekt P, Heliovaara M, Reunanen A. Consumption of sweetened beverages and intakes of fructose and glucose predict type 2 diabetes occurrence. J Nutr. 2007;137:1447–54.
Ahmadi-Abhari S, Luben RN, Powell N, Bhaniani A, Chowdhury R, Wareham NJ, et al. Dietary intake of carbohydrates and risk of type 2 diabetes: the European Prospective Investigation into Cancer-Norfolk study. Br J Nutr. 2014;111:342–52.
Sluijs I, Beulens JW, van der Schouw YT, van der AD, Buckland G, Kuijsten A, et al. Dietary glycemic index, glycemic load, and digestible carbohydrate intake are not associated with risk of type 2 diabetes in eight European countries. J Nutr. 2013;143:93–9.
Barclay AW, Flood VM, Rochtchina E, Mitchell P, Brand-Miller JC. Glycemic index, dietary fiber, and risk of type 2 diabetes in a cohort of older Australians. Diabetes Care. 2007;30:2811–3.
Kanehara R, Goto A, Sawada N, Mizoue T, Noda M, Hida A, et al. Association between sugar and starch intakes and type 2 diabetes risk in middle-aged adults in a prospective cohort study. Eur J Clin Nutr. 2021;76:746–755.
Meyer KA, Kushi LH, Jacobs DR Jr, Slavin J, Sellers TA, Folsom AR. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am J Clin Nutr. 2000;71:921–30. 2000
Colditz GA, Manson JE, Stampfer MJ, Rosner B, Willett WC, Speizer FE. Diet and risk of clinical diabetes in women. Am J Clin Nutr. 1992;55:1018–23.
Schulze MB, Schulz M, Heidemann C, Schienkiewitz A, Hoffmann K, Boeing H. Carbohydrate intake and incidence of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Br J Nutr. 2008;99:1107–16.
Tsilas CS, de Souza RJ, Mejia SB, Mirrahimi A, Cozma AI, Jayalath VH, et al. Relation of total sugars, fructose and sucrose with incident type 2 diabetes: a systematic review and meta-analysis of prospective cohort studies. CMAJ 2017;189:E711–E20.
Lutomski JE, van den Broeck J, Harrington J, Shiely F, Perry IJ. Sociodemographic, lifestyle, mental health and dietary factors associated with direction of misreporting of energy intake. Public Health Nutr. 2011;14:532–41.
Gottschald M, Knuppel S, Boeing H, Buijsse B. The influence of adjustment for energy misreporting on relations of cake and cookie intake with cardiometabolic disease risk factors. Eur J Clin Nutr. 2016;70:1318–24.
Kuhnle GG, Tasevska N, Lentjes MA, Griffin JL, Sims MA, Richardson L, et al. Association between sucrose intake and risk of overweight and obesity in a prospective sub-cohort of the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk). Public Health Nutr. 2015;18:2815–24.
Bingham S, Luben R, Welch A, Tasevska N, Wareham N, Khaw KT. Epidemiologic assessment of sugars consumption using biomarkers: comparisons of obese and nonobese individuals in the European prospective investigation of cancer Norfolk. Cancer Epidemiol Biomark Prev. 2007;16:1651–4.
Taubes G. What if sugar is worse than just empty calories? An essay by Gary Taubes. BMJ 2018;360:j5808.
Lang A, Kuss O, Filla T, Schlesinger S. Association between per capita sugar consumption and diabetes prevalence mediated by the body mass index: results of a global mediation analysis. Eur J Nutr. 2021;60:2121–9.
Willett WC. Nutritional Epidemiology. 3rd edn. New York, NY: Oxford University Press. 2013.
Lachat C, Hawwash D, Ocke MC, Berg C, Forsum E, Hornell A, et al. Strengthening the reporting of observational studies in epidemiology-nutritional epidemiology (STROBE-nut): an extension of the STROBE statement. PLoS Med. 2016;13:e1002036.
Tasevska N, Runswick SA, McTaggart A, Bingham SA. Urinary sucrose and fructose as biomarkers for sugar consumption. Cancer Epidemiol Biomark Prev. 2005;14:1287–94.
Cooper AJ, Sharp SJ, Lentjes MA, Luben RN, Khaw KT, Wareham NJ, et al. A prospective study of the association between quantity and variety of fruit and vegetable intake and incident type 2 diabetes. Diabetes Care. 2012;35:1293–300.
Park JY, Mitrou PN, Keogh RH, Luben RN, Wareham NJ, Khaw KT. Self-reported and measured anthropometric data and risk of colorectal cancer in the EPIC-Norfolk study. Int J Obes (Lond). 2012;36:107–18.
Wareham NJ, Jakes RW, Rennie KL, Mitchell J, Susie Hennings S, Day NE. Validity and repeatability of the EPIC-Norfolk Physical Activity Questionnaire. Int J Epidemiol. 2002;31:168–74. 2002
VanderWeele TJ. Causal mediation analysis with survival data. Epidemiology 2011;22:582–5.
Creed J, Gerke T Causal mediation analysis in R. https://github.com/GerkeLab/mediator.
VanderWeele TJ. Mediation analysis: a practitioner’s guide. Annu Rev Public Health. 2016;37:17–32.
VanderWeele TJ. A three-way decomposition of a total effect into direct, indirect, and interactive effects. Epidemiology 2013;24:224–32.
Fasanelli F, Giraudo MT, Ricceri F, Valeri L, Zugna D. Marginal time-dependent causal effects in mediation analysis with survival data. Am J Epidemiol. 2019;188:967–74.
Joosen AM, Kuhnle GG, Runswick SA, Bingham SA. Urinary sucrose and fructose as biomarkers of sugar consumption: comparison of normal weight and obese volunteers. Int J Obes (Lond). 2008;32:1736–40.
Tasevska N, Sagi-Kiss V, Palma-Duran SA, Barrett B, Chaloux M, Commins J, et al. Investigating the performance of 24-h urinary sucrose and fructose as a biomarker of total sugars intake in US participants - a controlled feeding study. Am J Clin Nutr. 2021;114:721–30.
Tasevska N, Midthune D, Potischman N, Subar AF, Cross AJ, Bingham SA, et al. Use of the predictive sugars biomarker to evaluate self-reported total sugars intake in the Observing Protein and Energy Nutrition (OPEN) study. Cancer Epidemiol Biomark Prev. 2011;20:490–500.
Tasevska N, Pettinger M, Kipnis V, Midthune D, Tinker LF, Potischman N, et al. Associations of biomarker-calibrated intake of total sugars with the risk of type 2 diabetes and cardiovascular disease in the Women’s health initiative observational study. Am J Epidemiol. 2018;187:2126–35.
Campbell R, Tasevska N, Jackson KG, Sagi-Kiss V, di Paolo N, Mindell JS, et al. Association between urinary biomarkers of total sugars intake and measures of obesity in a cross-sectional study. PLoS One. 2017;12:e0179508.
Ramne S, Gray N, Hellstrand S, Brunkwall L, Enhorning S, Nilsson PM, et al. Comparing self-reported sugar intake with the sucrose and fructose biomarker from overnight urine samples in relation to cardiometabolic risk factors. Front Nutr. 2020;7:62.
Beasley JM, Jung M, Tasevska N, Wong WW, Siega-Riz AM, Sotres-Alvarez D, et al. Biomarker-predicted sugars intake compared with self-reported measures in US Hispanics/Latinos: results from the HCHS/SOL SOLNAS study. Public Health Nutr. 2016;19:3256–64.
Tasevska N, Midthune D, Tinker LF, Potischman N, Lampe JW, Neuhouser ML, et al. Use of a urinary sugars biomarker to assess measurement error in self-reported sugars intake in the nutrition and physical activity assessment study (NPAAS). Cancer Epidemiol Biomark Prev. 2014;23:2874–83.
Te Morenga L, Mallard S, Mann J. Dietary sugars and body weight: systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012;346:e7492.
Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. 2010;89:309–19.
Assy N, Nasser G, Kamayse I, Nseir W, Beniashvili Z, Djibre A, et al. Soft drink consumption linked with fatty liver in the absence of traditional risk factors. Can J Gastroenterol. 2008;22:811–6.
Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol. 2008;48:993–9.
Younossi ZM. Non-alcoholic fatty liver disease - a global public health perspective. J Hepatol. 2019;70:531–44.
Malik VS, Hu FB. Sweeteners and risk of obesity and type 2 diabetes: the role of sugar-sweetened beverages. Curr. Diab. Rep. 2012;12:195–203.
Buyken AE, Mitchell P, Ceriello A, Brand-Miller J. Optimal dietary approaches for prevention of type 2 diabetes: a life-course perspective. Diabetologia 2010;53:406–18.
Greenwood DC, Threapleton DE, Evans CE, Cleghorn CL, Nykjaer C, Woodhead C, et al. Glycemic index, glycemic load, carbohydrates, and type 2 diabetes: systematic review and dose-response meta-analysis of prospective studies. Diabetes Care. 2013;36:4166–71.
Acknowledgements
The EPIC-Norfolk study (DOI 10.22025/2019.10.105.00004) has received funding from the Medical Research Council (MR/N003284/1, MC-UU_12015/1, and MC_UU_00006/1) and Cancer Research UK (C864/A14136). We are grateful to all the participants who have been part of the project and to the many members of the study teams at the University of Cambridge who have enabled this research.
Funding
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Innovation, Science, Research, and Technology of the State North Rhine-Westphalia. This study was supported in part by a grant from the German Federal Ministry of Education and Research to the German Center for Diabetes Research (DZD). The funding source has no role in the decisions about the data collection, analysis, interpretation of the data, preparation, review, or approval of the manuscript. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
SS and OK designed the research. AL performed the analyses with the support of TF and OK. AL and SS interpreted the data and wrote the first draft of the paper. AL, OK, TF, GK, and SS critically read the manuscript and approved the final version. AL and SS are guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria were omitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lang, A., Kuss, O., Filla, T. et al. The mediating role of obesity on the prospective association between urinary sucrose and diabetes incidence in a sub-cohort of the EPIC-Norfolk. Nutr. Diabetes 13, 14 (2023). https://doi.org/10.1038/s41387-023-00243-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41387-023-00243-5
