
Abstract
Background
Antibiotics are the most prescribed medication in the neonatal intensive care unit (NICU) and there is marked variation in their use. While they are vital for treatment of infections, they put infants at risk for infections with drug resistant organisms, alteration in their microbiome and several other morbidities. Specific guidelines for neonates are often lacking and our NICU is not compliant with late onset sepsis (LOS) guidelines.
Objective
By January 2019, there will be >75% compliance with our LOS bundle for any infant admitted to Tampa General Hospital’s (TGH) NICU undergoing a LOS evaluation at >72 h of life. The bundle includes documented reason for LOS evaluation, appropriate initial antibiotic selection, appropriate initial evaluation considered, and appropriate de-escalation of antibiotics.
Study design
The project was implemented in the NICU at TGH, the academic medical center affiliated with the University of South Florida in Tampa, FL. The multidisciplinary antimicrobial stewardship (ASP) team responsible for the project consists of a neonatology attending, three neonatology fellows, a pediatric infectious disease attending, and two NICU pharmacists. The project was started in January 2017 and all data were collected prospectively. We implemented multiple Plan-Do-Study-Act cycles in a stepwise manner; outcome measures included compliance with the LOS bundle and ASP team recommendations. Our process measures were the documented reason for sepsis evaluation, appropriate initial evaluation considered, appropriate antibiotic selection and appropriate antibiotic de-escalation. Patient length of stay was the balancing measure studied.
Results
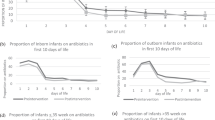
During this 20-month initiative, there were 232 infants who underwent LOS evaluation and there were 98 true positive cultures from blood (28%), urine (35%), and cerebrospinal fluid (3%). Commonly documented rationales for treatment of culture negative sepsis were clinical pneumonia (38%) and necrotizing enterocolitis (38%). Common indications for LOS evaluations were increased respiratory support (51%) and abdominal distension (17%). There was improvement in appropriate initial antibiotic selection (70% vs. 94%); appropriate consideration of initial evaluation (63% vs. 94%, respectively); appropriate de-escalation of antibiotics (86% vs. 100%, respectively) and increase in LOS bundle compliance (44% vs. 87%, respectively). The overall antibiotic utilization rate and length of treatment did not change significantly.
Conclusions
Developing and engaging a NICU ASP team improves compliance with late onset sepsis guidelines through the implementation of a LOS bundle of care.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110:285–91.
Puopolo KM, Benitz WE, Zaoutis TE. Management of neonates born at ≥35 0/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics 2018;142:e20182894.
Puopolo KM, Benitz WE, Zaoutis TE. Management of neonates born at ≤34 6/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics. 2018;142:e20182896.
Wirtschafter DD, Padilla G, Suh O, Wan K, Trupp D, Fayard EE. Antibiotic use for presumed neonatally acquired infections far exceeds that for central line-associated blood stream infections: an exploratory critique. J Perinatol. 2011;31:514–8.
Hsieh EM, Hornik CP, Clark RH, Laughon MM, Benjamin DK Jr, Smith PB. Medication use in the neonatal intensive care unit. Am J Perinatol. 2014;31:811–21.
Cotten CM, McDonald S, Stoll B, Goldberg RN, Poole K, Benjamin DK Jr. The association of third-generation cephalosporin use and invasive candidiasis in extremely low birth-weight infants. Pediatrics. 2006;118:717–22.
Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sanchez PJ, et al. Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics. 2009;123:58–66.
Kuppala VS, Meinzen-Derr J, Morrow AL, Schibler KR. Prolonged initial empirical antibiotic treatment is associated with adverse outcomes in premature infants. J Pediatr. 2011;159:720–5.
Coker MO, Hoen AG, Dade E, Lundgren S, Li Z, Wong AD, et al. Specific class of intrapartum antibiotics relates to maturation of the infant gut microbiota: a prospective cohort study. Bjog. 2019;217–27.
Abdel-Hady H, Hawas S, El-Daker M, El-Kady R. Extended-spectrum beta-lactamase producing Klebsiella pneumoniae in neonatal intensive care unit. J Perinatol. 2008;28:685–90.
Khassawneh M, Khader Y, Abuqtaish N. Clinical features of neonatal sepsis caused by resistant Gram-negative bacteria. Pediatr Int. 2009;51:332–6.
Jenkins TC, Knepper BC, Shihadeh K, Haas MK, Sabel AL, Steele AW, et al. Long-term outcomes of an antimicrobial stewardship program implemented in a hospital with low baseline antibiotic use. Infect Control Hosp Epidemiol. 2015;36:664–72.
Karanika S, Paudel S, Grigoras C, Kalbasi A, Mylonakis E. Systematic review and meta-analysis of clinical and economic outcomes from the implementation of hospital-based antimicrobial stewardship programs. Antimicrobial Agents Chemother. 2016;60:4840–52.
Patel SJ, Saiman L. Principles and strategies of antimicrobial stewardship in the neonatal intensive care unit. Semin Perinatol. 2012;36:431–6.
Warren S, Garcia M, Hankins C. Impact of neonatal early-onset sepsis calculator on antibiotic use within two tertiary healthcare centers. J Perinatol. 2017;37:394–7.
Makri V, Davies G, Cannell S, Willson K, Winterson L, Webb J, et al. Managing antibiotics wisely: a quality improvement programme in a tertiary neonatal unit in the UK. BMJ open Qual. 2018;7:e000285.
Dong Y, Speer CP. Late-onset neonatal sepsis: recent developments. Arch Dis Child Fetal Neonatal Ed. 2015;100: F257–63.
CDC. Get Smart for Health Care.
Davidoff F, Batalden P, Stevens D, Ogrinc G, Mooney SE, SQUIRE development group. Publication guidelines for quality improvement studies in health care: evolution of the SQUIRE project. BMJ. 2009;338:a3152.
Kanegaye JT, Soliemanzadeh P, Bradley JS. Lumbar puncture in pediatric bacterial meningitis: defining the time interval for recovery of cerebrospinal fluid pathogens after parenteral antibiotic pretreatment. Pediatrics. 2001;108:1169–74.
Piantino JH, Schreiber MD, Alexander K, Hageman J. Culture negative sepsis and systemic inflammatory response syndrome in neonates. NeoReviews. 2013;14:e294–305.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81.
Perla RJ, Provost LP, Murray SK. The run chart: a simple analytical tool for learning from variation in healthcare processes. BMJ Qual Saf. 2011;20:46–51.
Schulman J, Dimand RJ, Lee HC, Duenas GV, Bennett MV, Gould JB. Neonatal intensive care unit antibiotic use. Pediatrics. 2015;135:826–33.
Hysong SJ, Best RG, Pugh JA. Audit and feedback and clinical practice guideline adherence: Making feedback actionable. Implement Sci. 2006;1:9.
Acknowledgements
The authors greatly appreciate Dr Jane Carver’s editorial review of the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lamba, V., D’souza, S., Carafa, C. et al. Standardizing the approach to late onset sepsis in neonates through antimicrobial stewardship: a quality improvement initiative. J Perinatol 40, 1433–1440 (2020). https://doi.org/10.1038/s41372-019-0577-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-019-0577-5
This article is cited by
-
Dopamine or norepinephrine for sepsis-related hypotension in preterm infants: a retrospective cohort study
European Journal of Pediatrics (2022)
