
Abstract
Objective
Our specific, measurable, attainable, relevant, and time-limited (SMART) aim was to reduce the incidence of severe intracranial hemorrhage (ICH) among preterm infants born <30 weeks’ gestation from a baseline of 24% (January 2012–December 2013) to a long-term average of 11% by December 2015.
Study design
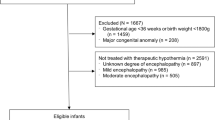
We instituted an ICH bundle consisting of elements of the “golden hour” (delayed cord clamping, optimized cardiopulmonary resuscitation, improved thermoregulation) and provision of cluster care in the neonatal intensive care unit (NICU). We identified key drivers to achieve our SMART aims, and implemented quality improvement (QI) cycles: initiation of the ICH bundle, education of NICU staff, and emphasis on sustained adherence. We excluded infants born outside our facility and those with congenital anomalies.
Results
Using statistical process control analysis (p-chart), the ICH bundle was associated with successful reduction in severe ICH (grade 3–4) in our NICU from a prebundle rate of 24% (January 2012–December 2013) to a sustained reduction over the next 4 years to an average rate of 9.7% by December 2017. Results during 2016–2017 showed a sustained improvement beyond the goal for 2014–2015. Over the same interval, there was improvement in admission temperatures [median 36.1 °C (interquartile range: 35.3–36.7 °C) vs. 37.1 °C (36.8–37.5 °C), p < 0.01] and a decrease in mortality rate [pre: 16/117 (14%) vs. post: 16/281 (6%), P < 0.01].
Conclusion
Our multidisciplinary QI initiative decreased severe ICH in our institution from a baseline rate of 24% to a lower rate of 9.7% over the ensuing 4 years. Intensive focus on sustained implementation of an ICH bundle protocol consisting of improved delivery room management, thermoregulation, and clustered care in the NICU was temporally associated with a clinically significant reduction in severe ICH.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Ment LR, Oh W, Philip AG, Ehrenkranz RA, Duncan CC, Allan W, et al. Risk factors for early intraventricular hemorrhage in low birth weight infants. J Pediatr. 1992;121:776–83.
Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. J Am Med Assoc. 2015;314:1039–51.
Schmidt B, Asztalos EV, Roberts RS, Robertson CM, Suave RS, Whitfield MF, et al. Impact of bronchopulmonary dysplasia, brain injury, and severe retinopathy on the outcome of extremely low-birth-weight infants at 18 months: results from the trial of indomethacin prophylaxis in preterms. J Am Med Assoc. 2003;289:1124–9.
Bolisetty S, Dhawan A, Abdel-Latif M, Bajuk B, Stack J, Lui K, et al. Intraventricular hemorrhage and neurodevelopmental outcomes in extreme preterm infants. Pediatrics. 2014;133:55–62.
Mukerji A, Shah V, Shah PS. Periventricular/Intraventricular hemorrhage and neurodevelopmental outcomes: a meta-analysis. Pediatrics. 2015;136:1132–43.
Moore T, Hennessy EM, Myles J, Sj Johnson, Draper ES, Costeloe KL, et al. Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: the EPICure studies. Br Med J. 2012;345:e7961.
Serenius F, Kallen K, Blennow M, Ewald U, Fellman V, Holmstrom G, et al. Neurodevelopmental outcome in extremely preterm infants at 2.5 years after active perinatal care in Sweden. J Am Med Assoc. 2013;309:1810–20.
Younge N, Goldstein RF, Bann CM, Hintz SR, Patel RM, Smith PB, et al. Survival and neurodevelopmental outcomes among periviable infants. N Engl J Med. 2017;376:617–28.
Kaiser JR, Gauss CH, Pont MM, Williams DK. Hypercapnia during the first 3 days of life is associated with severe intraventricular hemorrhage in very low birth weight infants. J Perinatol. 2006;26:279–85.
Volpe JJ. Brain injury in premature infants: a complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009;8:110–24.
Ballabh P. Pathogenesis and prevention of intraventricular hemorrhage. Clin Perinatol. 2014;41:47–67.
Mohamed MA, Aly H. Male gender is associated with intraventricular hemorrhage. Pediatrics. 2010;125:e333–9.
Ment LR, Aden U, Bauer CR, Bada HS, Carlo WA, Kaiser JR, et al. Genes and environment in neonatal intraventricular hemorrhage. Semin Perinatol. 2015;39:592–603.
Bhandari V, Bizzarro MJ, Shetty A, Zhong X, Page GP, Zhang H, et al. Familial and genetic susceptibility to major neonatal morbidities in preterm twins. Pediatrics. 2006;117:1901–6.
Ryckman KK, Dagle JM, Kelsey K, Momany AM, Murray JC. Replication of genetic associations in the inflammation, complement, and coagulation pathways with intraventricular hemorrhage in LBW preterm neonates. Pediatr Res. 2011;70:90–5.
Shankaran S, Lin A, Maller-Kesselman J, Zhang H, O’Shea TM, Bada HS, et al. Maternal race, demography, and health care disparities impact risk for intraventricular hemorrhage in preterm neonates. J Pediatr. 2014;164:1005–11 e3.
Mercer JS, Vohr BR, McGrath MM, Padbury JF, Wallach M, Oh W. Delayed cord clamping in very preterm infants reduces the incidence of intraventricular hemorrhage and late-onset sepsis: a randomized, controlled trial. Pediatrics. 2006;117:1235–42.
Malusky S, Donze A. Neutral head positioning in premature infants for intraventricular hemorrhage prevention: an evidence-based review. Neonatal Netw. 2011;30:381–96.
Wyckoff MH. Initial resuscitation and stabilization of the periviable neonate: the Golden-Hour approach. Semin Perinatol. 2014;38:12–6.
Manley BJ, Owen LS, Hooper SB, Jacobs SE, Cheong JLY, Doyle LW, et al. Towards evidence-based resuscitation of the newborn infant. Lancet. 2017;389:1639–48.
https://public.vtoxford.org/wp-content/uploads/2015/09/Manual_of_Operations_Part2_v20.pdf
Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–34.
Parry G, Tucker J, Tarnow-Mordi W, Group UKNSSC.. CRIB II: an update of the clinical risk index for babies score. Lancet. 2003;361:1789–91.
Perla RJ, Provost LP, Murray SK. The run chart: a simple analytical tool for learning from variation in healthcare processes. BMJ Qual Saf. 2011;20:46–51.
Benneyan JC, Lloyd RC, Plsek PE. Statistical process control as a tool for research and healthcare improvement. Qual Saf Health Care. 2003;12:458–64.
Mohammed MA, Worthington P, Woodall WH. Plotting basic control charts: tutorial notes for healthcare practitioners. Qual Saf Health Care. 2008;17:137–45.
Wei JC, Catalano R, Profit J, Gould JB, Lee HC. Impact of antenatal steroids on intraventricular hemorrhage in very-low-birth-weight infants. J Perinatol. 2016;36:352–6.
Miller SS, Lee HC, Gould JB. Hypothermia in very low birth weight infants: distribution, risk factors and outcomes. J Perinatol. 2011;31(Suppl 1):S49–56.
Lyu Y, Shah PS, Ye XY, et al. Association between admission temperature and mortality and major morbidity in preterm infants born at fewer than 33 weeks’ gestation. JAMA Pediatr. 2015;169:e150277.
Finer NN, Carlo WA, Duara S, et al. Delivery room continuous positive airway pressure/positive end-expiratory pressure in extremely low birth weight infants: a feasibility trial. Pediatrics. 2004;114:651–7.
Sauer CW, Kong JY, Vaucher YE, Finer N, Proudfoot JA, Boutin MA, et al. Intubation attempts increase the risk for severe intraventricular hemorrhage in preterm infants—a retrospective cohort study. J Pediatr. 2016;177:108–13.
Wallenstein MB, Birnie KL, Arain YH, Yang W, Yamada NK, Huffman LC, et al. Failed endotracheal intubation and adverse outcomes among extremely low birth weight infants. J Perinatol. 2016;36:112–5.
Perlman JM, McMenamin JB, Volpe JJ. Fluctuating cerebral blood-flow velocity in respiratory-distress syndrome. Relation to the development of intraventricular hemorrhage. N Engl J Med. 1983;309:204–9.
Fabres J, Carlo WA, Phillips V, Howard G, Ambalavanan N. Both extremes of arterial carbon dioxide pressure and the magnitude of fluctuations in arterial carbon dioxide pressure are associated with severe intraventricular hemorrhage in preterm infants. Pediatrics. 2007;119:299–305.
Sommers R, Stonestreet BS, Oh W, Laptook A, Yanowitz TD, Raker C, et al. Hemodynamic effects of delayed cord clamping in premature infants. Pediatrics. 2012;129:e667–72.
Bhatt S, Alison BJ, Wallace EM, Crossley KJ, Gill AW, Kluckow M, et al. Delaying cord clamping until ventilation onset improves cardiovascular function at birth in preterm lambs. J Physiol. 2013;591:2113–26.
Oh W, Fanaroff AA, Carlo WA, Donovan EF, McDonald SA, Poole WK, et al. Effects of delayed cord clamping in very-low-birth-weight infants. J Perinatol. 2011;31(Suppl 1):S68–71.
Rabe H, Diaz-Rossello JL, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev 2012; 8:CD003248.
Mercer JS, Vohr BR, Erickson-Owens DA, Padbury JF, Oh W. Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J Perinatol. 2010;30:11–6.
Emery JR, Peabody JL. Head position affects intracranial pressure in newborn infants. J Pediatr. 1983;103:950–3.
Romantsik O, Calevo MG, Bruschettini M. Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular hemorrhage in preterm infants. Cochrane Database Syst Rev. 2017;7:CD012362.
Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst Rev 2006;2:CD001814.
Doyle LW. Antenatal magnesium sulfate and neuroprotection. Curr Opin Pediatr. 2012;24:154–9.
Mittendorf R, Dambrosia J, Dammann O, Pryde PG, Lee KS, Ben-Ami TE, et al. Association between maternal serum ionized magnesium levels at delivery and neonatal intraventricular hemorrhage. J Pediatr. 2002;140:540–6.
Canterino JC, Vermal UL, Visintainer PF, Figueroa R, Klein SA, Tejani NA. Maternal magnesium sulfate and the development of neonatal periventricular leucomalacia and intraventricular hemorrhage. Obstet Gynecol. 1999;93:396–402.
Acknowledgments
We thank all our collaborators and NICU staff; Dr. R. Donald Garrison for his leadership, building the foundation that has become the ICH bundle; Dr. Philipp Aldana for encouraging us to report our findings; and Dr. Matt Garber for his expertize on quality improvement. Lastly, we thank all our infants who continually inspire us; and their families who have trusted us not only to do what is right but also to improve on our best efforts.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Chiriboga, N., Cortez, J., Pena-Ariet, A. et al. Successful implementation of an intracranial hemorrhage (ICH) bundle in reducing severe ICH: a quality improvement project. J Perinatol 39, 143–151 (2019). https://doi.org/10.1038/s41372-018-0257-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-018-0257-x
This article is cited by
-
Quality improvement in the golden hour for premature infants: a scoping review
BMC Pediatrics (2024)
-
Variations in care of neonates during therapeutic hypothermia: call for care practice bundle implementation
Pediatric Research (2023)
-
Impact of quality improvement outreach education on the incidence of acute brain injury in transported neonates born premature
Journal of Perinatology (2022)
-
The development of neonatal neurointensive care
Pediatric Research (2019)
