
Abstract
Introduction:
Preterm birth affects 8–12% of live births and is associated with the development of elevated arterial blood pressure and aortic narrowing in later life; this suggests that preterm birth may alter the development of arteries. Our objective was to determine the effects of preterm birth, accompanied by antenatal corticosteroid administration, on the structure of the aorta and pulmonary artery, which experience different alterations in pressure flow at birth.
Results:
At 11 wk, preterm lambs had significantly thicker aortic walls and a smaller lumen, whereas the morphometry of the pulmonary artery was unaffected. Elastin deposition was markedly increased in the aorta and pulmonary artery and smooth muscle content was reduced in the aorta only. In preterm lambs we found injury in the aorta only; controls were unaffected.
Discussion:
We conclude that moderate preterm birth after antenatal betamethasone can cause injury and persistent alterations in the structure and composition of the aorta, with lesser effects in the pulmonary artery. Our findings suggest that preterm birth may increase the risk of atherosclerosis and aortic aneurysms in later life.
Methods:
Using an established ovine model of preterm birth, lambs were born at 0.9 of gestation and underwent necropsy at 11 wk after birth; controls were born at term.
Similar content being viewed by others

Main
Preterm birth, defined as birth prior to 37 completed weeks of gestation, affects 8–12% of live births. As a result of advances in neonatal care, most preterm infants survive infancy, even those born as early as 23 wk (1). Epidemiological studies have linked preterm birth to hypertension and vascular abnormalities in children and young adults (2,3,4,5,6,7,8,9); the risk is increased with decreasing gestational age at birth, suggestive of causality (2,3,6). For example, one study found a 0.31 mm Hg increase in adult blood pressure for every week of prematurity (2). Such increases are important because a 2 mm Hg increase in adult blood pressure is associated with a 6% increase in the risk of coronary artery disease and a 15% increase in the risk of stroke or transient ischemic attack (10).
Preterm birth has also been associated with increased vascular resistance and arterial wall thickness, which are both associated with hypertension and adverse cardiovascular outcomes (11). For instance, a study of adolescent girls born preterm found higher brachial artery and aortic pressures, a narrower abdominal aorta, and lower peripheral skin blood flow than in girls born at term (9). The cause of these vascular changes might relate to vascular adaptations that were set in place soon after preterm birth as a result of vascular immaturity.
In this regard, we have recently shown adverse structural remodeling of the myocardium in immature lambs as a result of being born preterm (12). The major components of the arterial wall are elastin, collagen, and smooth muscle, each of which is laid down during gestation and early postnatal life (13). Importantly, local hemodynamic conditions in the perinatal period play a major role in determining the structural composition of major arteries (14), which, in turn, directly influences their wall compliance. The human fetal aorta is exposed to a steadily increasing luminal pressure, rising from a mean of 28 mm Hg at 20 wk to 45 mm Hg at 40 wk (15); this increase in pressure provides the normal environment for aortic development. At birth, systemic arterial pressure and aortic flow increase substantially, largely as a result of the loss of the placental vascular bed, closure of vascular shunts, and a decrease in pulmonary vascular resistance (16). Preterm birth, including moderate preterm birth, occurs during this period of compositional change within the aorta (17), at a time when the aorta is immature, thus exposing it to increased shear stress and pressure before it is structurally mature.
In utero, the developing pulmonary artery is exposed to pressures identical to those of the fetal systemic circulation (18) and receives only a small fraction of cardiac output (16,19). At birth, pressure within the pulmonary artery falls (mean pressure ~15 mm Hg), and it receives all of the right ventricular output after closure of the ductus arteriosus (20). This change from high pressure/low flow to low pressure/high flow, when it occurs prematurely, may result in abnormal changes to the walls of the pulmonary artery.
A major recent advance in improving the survival of preterm infants is the administration of antenatal corticosteroids to women who show evidence of preterm labor. Our lamb model of preterm birth includes antenatal betamethasone administration to the ewe because the majority of preterm infants in developed countries will be exposed to antenatal corticosteroids (21).
Hence, we propose that, as a result of preterm birth, the immature aorta undergoes structural remodeling that differs from that occurring at term; we propose that these structural changes may lead to aortic narrowing, impaired aortic compliance, and subsequent development of hypertension. Second, in the pulmonary artery, as a result of the substantial rise in blood flow and the reduction in luminal pressure following preterm birth, we propose that there will be persistent changes in the morphometry and composition of the arterial wall, but these will differ from the changes in the aorta. We examined the proximal ascending aorta and pulmonary artery because these areas experience the highest blood flow velocity, shear stress, and dynamic pressures (22,23). Our objective was to determine and compare the effects of preterm birth, accompanied by antenatal corticosteroid exposure, on the structure and composition of the walls of the aorta and pulmonary artery.
Results
Preterm lambs were born at 133 ± 1 d of gestational age and controls were born at term (147 ± 0 d). At birth, preterm lambs were significantly lighter than controls (preterm, 3.37 ± 0.26 kg vs. term, 4.10 ± 0.18 kg, P < 0.05); however, by 9 wk after term-equivalent age (TEA), there was no significant difference in body weight (preterm, 17.11 ± 0.62 kg, vs. term, 16.83 ± 0.67 kg). At 8 wk after TEA, there were no differences between groups, either in mean arterial pressure (preterm, 76.6 ± 2.0 mm Hg, vs. term, 76.1 ± 1.5 mm Hg) or in systolic and diastolic pressures and heart rate. At necropsy, no lamb had a patent foramen ovale or ductus arteriosus (dye or probe patent). No cardiac structural abnormalities (e.g., septal defects) were observed in term or preterm lambs.
Aortic Injury
Injury was observed histologically in the aortas of four of the seven preterm lambs. The injury was apparent in three of the four affected lambs in the second segment and in all four affected lambs in the third segment. The lesions occurred in one male and three female preterm lambs. Lesions were round at the intimal surface and were on average 2.5 mm in diameter and 800 µm deep. Lesions were located within the tunica intima. The lesions were observed to be composed primarily of collagen and smooth muscle, with low levels of elastin in an abnormal configuration ( Figure 1 ).

Section stained with Verhoeff’s elastin demonstrating the aortic injury seen in preterm lambs. Elastin is stained black. Main image is at 10× magnification. Main image scale bar represents 200 µm. Inset (upper right) is at 3× magnification. Inset image bar represents 1 mm.
Immunohistochemistry revealed minimal apoptosis (caspase 3) and proliferation (Ki-67) in the lesion or the surrounding tissue.
Aortic Morphometry
Aortic walls were significantly thicker in preterm lambs compared with controls, by an average of 22.6% across the three segments ( Figure 2a ). There was a statistically significant narrowing (24.7% reduction in lumen area) in the third segment of the aorta in the preterm lambs compared with controls ( Figure 2b ) and therefore an increased media/lumen ratio in the same segment ( Figure 2f ).

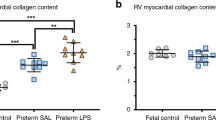
Summary of morphometric data from the aorta of preterm and term lambs. Data from term lambs appear in blank bars and those from preterm lambs appear in solid bars. All plots show means ± SEM. *P < 0.05. (a) A marked increase in wall thickness was found in preterm lambs across all three segments. In the third segment, there was (b) a reduction in lumen area and (f) an increased media to lumen ratio. In all aortic segments, we observed (c) an increase in elastin, (d) reduced smooth muscle, and (e) no change in collagen deposition. seg, segment.
Aortic Wall Composition
Aortic elastin deposition was greater in all three segments in preterm lambs relative to controls ( Figure 2c ). Smooth muscle content was significantly lower in all segments of the aorta in preterm lambs compared with controls ( Figure 2d ); however, total collagen deposition did not differ among groups ( Figure 2e ).
Pulmonary Artery Morphometry
The mean thickness of the pulmonary arterial wall was 10% lower in preterm lambs compared with controls; however, the difference was not significant (P = 0.08, Figure 3a ). After adjusting for lumen circumference, thickness between groups did not differ. No difference between groups was detected in pulmonary arterial lumen area ( Figure 3b ) or in the media/lumen ratio ( Figure 3f ).

Summary of morphometric data from the pulmonary artery of preterm and term lambs. Data from term lambs appear in blank bars and those from preterm lambs appear in solid bars. All plots show means ± SEM. *P < 0.05. (a) Wall thickness was reduced by 10% in all three segments, but this was not statistically significant. There was no alteration in (b) lumen area or (f) media/lumen ratio. In all segments of pulmonary artery, there was (c) an increase in elastin (d) but no change in smooth muscle or (e) collagen deposition. seg, segment.
Pulmonary Artery Composition
Pulmonary arterial elastin deposition was greater in all three segments from preterm lambs relative to term lambs ( Figure 3c ). Smooth muscle deposition did not differ between groups ( Figure 3d ), but there was a significantly lower amount of collagen compared with controls in the second segment of the pulmonary artery, with a nonsignificant trend for reduction in the first segment ( Figure 3e ).
Discussion
Our findings clearly demonstrate evidence of aortic intimal injury and marked remodeling of the aortic wall, leading to a smaller luminal area, following preterm birth. These changes are likely irreversible and could contribute to long-term risk of cardiovascular disease, in particular, hypertension, aortic aneurysm, and atherosclerosis. Less dramatic changes were seen in the wall of the pulmonary artery, which probably reflects the difference in hemodynamic changes in these two arteries at the time of birth. The changes in vascular structure observed in the preterm lambs likely are an adaptive response of the immature arteries to the hemodynamic transition at birth, but we cannot exclude a possible influence of antenatal corticosteroids.
Aortic Injury
Surprisingly, we obtained striking morphological evidence demonstrating that injury can occur in the intima of the aortic wall following preterm birth. In four of the seven preterm aortas studied at 11 wk after birth, we observed focal areas of intimal thickening within the aorta, indicative of previous injury to the aortic wall; such intimal thickening was not observed in any of the term lambs at the same age.
Injury within the aortas of all preterm lambs is likely, but was only detected in four of the seven animals. Indeed, only a small segment of the aorta was analyzed, and aortic injury may have occurred more distally in the other preterm lambs. Importantly, the areas of aortic injury were not associated with the remnants of the ductus arteriosus because this area was avoided during dissection.
In testing our hypothesis, we focused on the ascending aorta because it is the region of highest dynamic pressure. In comparison, there is relatively low pressure at the aortic valve (with some pressure being relieved by the branching of the coronary arteries at this level) (24). These differences in arterial pressure likely account for the most striking structural changes observed in our most distal segment because the first aortic segment analyzed was at the level of the aortic valves.
We propose that the large rise in aortic pressure and/or flow that occurs at birth (16,25,26,27) leads to intimal injury in the ascending aorta because the immature artery at the time of preterm birth is not sufficiently developed to accommodate the high postnatal levels of blood pressure and flow. Importantly, in this regard, we have found in preterm lambs that mean arterial pressure rises by more than 20 mm Hg at the time of birth (unpublished observations). Of particular concern, we found a substantial thinning of the media of the aortic wall at the site of injury. Indeed, the integrity of the aortic wall likely is substantially compromised at this location, rendering it vulnerable to aneurysm with aging, development of hypertension, and disease. In addition, intimal thickening acts as a precursor for atherosclerosis (28); hence, the preterm aorta appears to be predisposed to developing atherosclerosis at these sites.
We cannot exclude the possibility that the unavoidable use of antenatal betamethasone contributed to the development of the aortic injury, but we consider it unlikely owing to the low dose used.
Aortic Structure and Composition
In addition to aortic injury, we found marked remodeling of the aortic wall in response to preterm birth; there was an increase in aortic wall thickness that was associated with an increase in elastin deposition and reduced smooth muscle content but no change in collagen content. This is likely an adaptive response of the immature aorta to the high postnatal systemic arterial pressure, which is considerably higher than in utero (27). Indeed, local hemodynamic conditions in the perinatal period play a major role in the maturational changes in structural composition (elastin, smooth muscle, and collagen) of the aorta, which, in turn, directly influence aortic compliance (17). During the perinatal period, concentric lamellae of elastin rapidly form within the aortic wall and thereafter rates of elastin synthesis fall rapidly (29). These layers of elastin are essential for the normal compliance of the aorta, allowing it to accommodate the high volume of blood during systole and the elastic recoil during diastole, which maintains an even forward flow of blood to the body against a closed aortic valve. Elastin has a very low turnover because its half-life is ~40 y (30), and the number of elastin lamellar units in a particular vascular segment does not change after birth.
In contrast, the smooth muscle content within the aortic media of the preterm lambs was significantly less than in the controls. This implies that these aortas could be less responsive to vasostimulatory factors.
Significant narrowing of the aortic lumen accompanied the marked remodeling of the aortic wall, probably resulting from the thickened media. In accordance with our findings, a recent study showed that the aortas of adolescent girls born preterm were narrower and less stiff than those of girls born at term (9). In another study, aortic narrowing was reported in adolescents who were born preterm (7). Arterial narrowing is likely to be detrimental in the long term and may contribute to the now well-described elevation in arterial pressure in subjects born preterm (2,3,4,5,8,9,31).
Pulmonary Artery Less Vulnerable to Preterm Birth
In accordance with our hypothesis, we observed very few changes in the structure and composition of the pulmonary artery wall following preterm birth. Unlike the aorta, there appeared to be no deleterious effects of preterm birth on arterial wall structure, and there was no evidence of endothelial injury or luminal narrowing. The relative biochemical composition of the arterial wall was generally unaffected by preterm birth, except for a significant increase in elastin content. We propose that the differences observed in the aorta vs. the pulmonary artery result from differences in the mean luminal pressures to which these immature arteries are exposed in the period soon after birth.
Potential Role of Antenatal Corticosteroids
Antenatal exposure to betamethasone could have contributed to the aortic injury and vascular structural remodeling observed in our preterm lambs. Elastic lamellae within arterial walls are predominantly laid down in the perinatal period, and betamethasone may have led to the increased deposition of elastin within the aorta and pulmonary artery because corticosteroids are potent regulators of elastin synthesis (29). Similarly, evidence exists that antenatal corticosteroids can induce permanent changes in endothelial and vascular smooth muscle function, ultimately leading to endothelial dysfunction (32,33). Given that exposure to corticosteroids can lead to endothelial dysfunction, their use may also lead to intimal injury; together with the hemodynamic changes at birth, it is likely that severe intimal injury will ensue. However, a study in which lambs born at term (~145 d) were administered 0.2 mg/kg dexamethasone twice a day, from birth to postnatal day 10, did not reveal aortic injury or increased elastin deposition in the aorta at necropsy on day 10 (29). In the present study, we have been unable to determine whether betamethasone exposure mediated any of the observed arterial injury and remodeling following preterm birth. Unfortunately, it was not possible for us to avoid the use of betamethasone because preterm lambs do not survive without it. However, our animal model closely reflects the human scenario in which it is routine practice for women at risk of preterm delivery to be administered antenatal steroids.
In our study, we have avoided many of the other confounding factors associated with preterm birth in humans, such as intrauterine factors thought to induce preterm delivery (for example, chorioamnionitis and intrauterine growth restriction) and factors associated with postnatal care (for example, mechanical ventilation, hyperoxia, and postnatal medications) (34). Importantly, recent studies demonstrate that factors such as these can also influence the long-term vascular phenotype in subjects born preterm (8). Together with the present study, these studies highlight the vulnerability of the cardiovascular system of preterm infants and suggest a cumulative cardiovascular risk depending on the causes of preterm birth.
Conclusions
We have shown in a clinically relevant model of moderate preterm birth that there are injurious and persistent changes to the structure and composition of the aorta. These adverse effects appear to be the result of the rapid rise in systemic arterial pressure at the time of birth because they were not observed in the pulmonary artery, in which pressure falls after birth; it remains possible that exposure to antenatal corticosteroids could play a role in the observed effects. The aortic injury and luminal narrowing associated with preterm birth could predispose for long-term cardiovascular disease.
Methods
Ethical Approval
This study was approved by the Monash University Animal Ethics Committee in accordance with the National Health and Medical Research Council (Australia) guidelines for the care and handling of animals for scientific purposes.
Experimental Protocol
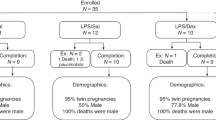
Studies were performed using two groups of lambs: one group was born preterm (0.9 of term) following antenatal corticosteroid exposure and the other was born at term. Preterm birth was induced using an established protocol (35). Briefly, 19 date-mated crossbred ewes were randomly assigned to deliver their lambs either at term (147 d after mating) or 14 d prior to term (133 d after mating). All lambs were born vaginally. To induce preterm birth, Epostane (50 mg i.v., Win-32729; Winthrop, Guildford, UK) was administered to 7 ewes 131 d after mating to induce delivery ~48 h later. On the same day, the ewes were also administered a dose of betamethasone (3.7–5 mg i.m., Celestone; Schering-Plough, North Ryde, Australia) to enhance the viability of preterm lambs. Control ewes did not receive betamethasone. The ewes gave birth to 1 male and 6 female preterm lambs. The control group (n = 12, 6 female, 6 male) were born spontaneously at term.
Lambs were raised in individual pens with their mothers. For 1–3 d after birth, preterm lambs were bottle-fed expressed milk from their mothers. Ewes had free access to feed and water. At 3 wk after TEA, lambs underwent aseptic surgery for implantation of femoral arterial and venous catheters; anesthesia was induced with Alfaxalone (3.5 mg/kg i.v. Alfaxan; Jurox, Rutherford, Australia) and maintained with 1%–1.5% inhaled Isoflurane (Baxter Healthcare, Rutherford, Old Toongabbie, Australia).
Using the arterial catheter, mean arterial pressure and heart rate were measured for 2 h on days 55 and 56 after TEA. Data were recorded and analyzed using PowerLab 8/30 and Chart Version 5.01 (ADInstruments, Sydney, Australia).
Necropsy Protocol
Preterm lambs were euthanized 9 wk after TEA using sodium pentobarbital (325 mg/ml). The 12 control lambs were euthanized 9 wk after term birth; at this age, lambs are preadolescent. The thoracic aorta and pulmonary arteries were excised and placed in saline with papaverine hydrochloride (DBL Pharmaceuticals, Mulgrave North, Australia) to maximally dilate the vessels. Vessels were then immersion fixed in 4% buffered formaldehyde solution. In each animal, aorta and pulmonary arteries were sampled from the same anatomical site. One-millimeter segments of the aorta and pulmonary artery were cut from just above the level of the valve (first segment) and then another two segments (1-mm thick, second and third segments) were taken 2 cm apart from the level of the valve, giving a total of three segments of 1-mm thickness. Arbitrary numbers were assigned to the removed samples so as to blind the investigators to grouping.
Paraffin sections from each segment were cut at 6 µm and mounted on poly-L-lysine-coated slides. Slides from every segment were stained with picrosirius red to measure collagen content (12), Gomori’s aldehyde fuchsin to measure wall thickness, and Verhoeff’s elastic stain to measure elastin content (36); other slides were prepared for immunohistochemistry (see below). To minimize variation, for each segment at least five slides per stain were used and average values were taken. Slides were interleaved so that no section was followed by a section stained using the same technique.
Immunohistochemistry
Some slides were immunohistochemically stained for cellular proliferation utilizing Ki-67 (MIB-1 clone; Dako, Botany, Australia) and active caspase-3 (Polyclonal; R&D Systems, Minneapolis, MN) to detect cells undergoing apoptosis and α-smooth muscle actin (1A4 clone, Dako) to determine the amount of vascular smooth muscle. Detection was performed using Dako EnVision+ Dual Link HRP/DAB+ kit (Dako). All negative controls were sections incubated without the primary antibody.
Sections were stained with the α-smooth muscle actin antibody (1:50 dilution) for 30 min. Positive controls were sections of adult ovine aorta.
Sections were stained with the Ki-67 (1:100 dilution) or active capase-3 antibodies (1:250) for 18 h and 30 min, respectively. Positive controls were Zymed Ki-67+ control slides (mouse tonsil, a known Ki-67-positive tissue) (Invitrogen, Carlsbad, CA) and sections from the right ventricle of a lamb that suffered a myocardial infarction.
Image Acquisition
Slides were scanned at 20× magnification using the Olympus dotSlide system (Version 2.1; Olympus, Tokyo, Japan). This enabled the capture of very large vessels with excellent resolution. Images were batch exported from dotSlide as individual frames and reconstructed in PanaVue ImageAssembler Professional (PanaVue, Quebec, Quebec, Canada).
Image Analysis
Images were analyzed using Image Pro-Plus Version 6.2 (Media Cybernetics, Bethesda, MD). Measurements of wall thickness, media thickness, and intima thickness were measured continuously along the entire wall. Area measurements were reconstructed areas based on the perimeter length of the structure to eliminate any changes caused by vessel distortion during processing into paraffin. Percentages of collagen, elastin, and α-smooth muscle actin were expressed as percentages of the entire vessel wall area.
Statistical Analysis
Data were analyzed using an independent samples t test (two-tailed). Analysis was performed using PASW Statistics 19 (IBM SPSS, Chicago, IL). Significance was set at P ≤ 0.05. Data are presented as means ± SEM. Graphs were prepared in GraphPad Prism Version 5.04 (GraphPad Software, La Jolla, CA).
Statement of Financial Support
This study was supported by the National Health and Medical Research Council of Australia (NHMRC) grant 384100. J.B. was supported by an Australian Postgraduate Award (APA).
References
Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR . The EPICure study: outcomes to discharge from hospital for infants born at the threshold of viability. Pediatrics 2000;106:659–71.
Johansson S, Iliadou A, Bergvall N, Tuvemo T, Norman M, Cnattingius S . Risk of high blood pressure among young men increases with the degree of immaturity at birth. Circulation 2005;112:3430–6.
Leon DA, Johansson M, Rasmussen F . Gestational age and growth rate of fetal mass are inversely associated with systolic blood pressure in young adults: an epidemiologic study of 165,136 Swedish men aged 18 years. Am J Epidemiol 2000;152:597–604.
Dalziel SR, Parag V, Rodgers A, Harding JE . Cardiovascular risk factors at age 30 following pre-term birth. Int J Epidemiol 2007;36:907–15.
Siewert-Delle A, Ljungman S . The impact of birth weight and gestational age on blood pressure in adult life: a population-based study of 49-year-old men. Am J Hypertens 1998;11(8 Pt 1):946–53.
Cooper R, Atherton K, Power C . Gestational age and risk factors for cardiovascular disease: evidence from the 1958 British birth cohort followed to mid-life. Int J Epidemiol 2009;38:235–44.
Edstedt Bonamy AK, Bengtsson J, Nagy Z, De Keyzer H, Norman M . Preterm birth and maternal smoking in pregnancy are strong risk factors for aortic narrowing in adolescence. Acta Paediatr 2008;97:1080–5.
Bonamy AK, Martin H, Jörneskog G, Norman M . Lower skin capillary density, normal endothelial function and higher blood pressure in children born preterm. J Intern Med 2007;262:635–42.
Bonamy AK, Bendito A, Martin H, Andolf E, Sedin G, Norman M . Preterm birth contributes to increased vascular resistance and higher blood pressure in adolescent girls. Pediatr Res 2005;58:845–9.
Cook NR, Cohen J, Hebert PR, Taylor JO, Hennekens CH . Implications of small reductions in diastolic blood pressure for primary prevention. Arch Intern Med 1995;155:701–9.
Burke GL, Evans GW, Riley WA, et al. Arterial wall thickness is associated with prevalent cardiovascular disease in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study. Stroke 1995;26:386–91.
Bensley JG, Stacy VK, De Matteo R, Harding R, Black MJ . Cardiac remodelling as a result of pre-term birth: implications for future cardiovascular disease. Eur Heart J 2010;31:2058–66.
Kelleher CM, McLean SE, Mecham RP . Vascular extracellular matrix and aortic development. Curr Top Dev Biol 2004;62:153–88.
Labella FS, Lindsay WG . The structure of human aortic elastin as influenced by age. J Gerontol 1963;18:111–8.
Struijk PC, Mathews VJ, Loupas T, et al. Blood pressure estimation in the human fetal descending aorta. Ultrasound Obstet Gynecol 2008;32:673–81.
Rudolph AM . Fetal and neonatal pulmonary circulation. Annu Rev Physiol 1979;41:383–95.
Berry CL, Looker T, Germain J . Nucleic acid and scleroprotein content of the developing human aorta. J Pathol 1972;108:265–74.
Emmanouilides GC, Moss AJ, Duffie ER Jr, Adams FH . Pulmonary arterial pressure changes in human newborn infants from birth to 3 days of age. J Pediatr 1964;65:327–33.
Pinson CW, Morton MJ, Thornburg KL . An anatomic basis for fetal right ventricular dominance and arterial pressure sensitivity. J Dev Physiol 1987;9:253–69.
McQuillan BM, Picard MH, Leavitt M, Weyman AE . Clinical correlates and reference intervals for pulmonary artery systolic pressure among echocardiographically normal subjects. Circulation 2001;104:2797–802.
Polyakov A, Cohen S, Baum M, Trickey D, Jolley D, Wallace EM . Patterns of antenatal corticosteroid prescribing 1998-2004. Aust N Z J Obstet Gynaecol 2007;47:42–5.
Karmonik C, Bismuth JX, Davies MG, Lumsden AB . Computational hemodynamics in the human aorta: a computational fluid dynamics study of three cases with patient-specific geometries and inflow rates. Technol Health Care 2008;16:343–54.
Pekkan K, Dasi LP, Nourparvar P, et al. In vitro hemodynamic investigation of the embryonic aortic arch at late gestation. J Biomech 2008;41:1697–706.
Svensson J, Gårdhagen R, Heiberg E, et al. Feasibility of patient specific aortic blood flow CFD simulation. Med Image Comput Comput Assist Interv 2006;9(Pt 1):257–63.
Rudolph AM . The changes in the circulation after birth. Their importance in congenital heart disease. Circulation 1970;41:343–59.
Rudolph AM . Fetal and neonatal pulmonary circulation. Am Rev Respir Dis 1977;115(6 Pt 2):11–8.
Louey S, Cock ML, Harding R . Postnatal development of arterial pressure: influence of the intrauterine environment. Arch Physiol Biochem 2003;111:53–60.
Guyton JR, Klemp KF . Transitional features in human atherosclerosis. Intimal thickening, cholesterol clefts, and cell loss in human aortic fatty streaks. Am J Pathol 1993;143:1444–57.
Bendeck MP, Keeley FW, Langille BL . Perinatal accumulation of arterial wall constituents: relation to hemodynamic changes at birth. Am J Physiol 1994;267(6 Pt 2):H2268–79.
Shapiro SD, Endicott SK, Province MA, Pierce JA, Campbell EJ . Marked longevity of human lung parenchymal elastic fibers deduced from prevalence of D-aspartate and nuclear weapons-related radiocarbon. J Clin Invest 1991;87:1828–34.
Cooper R, Atherton K, Power C . Gestational age and risk factors for cardiovascular disease: evidence from the 1958 British birth cohort followed to mid-life. Int. J. Epidemiol 2009;38:235–244.
Roghair RD, Segar JL, Kilpatrick RA, Segar EM, Scholz TD, Lamb FS . Murine aortic reactivity is programmed equally by maternal low protein diet or late gestation dexamethasone. J Matern Fetal Neonatal Med 2007;20:833–41.
Pulgar VM, Figueroa JP . Antenatal betamethasone administration has a dual effect on adult sheep vascular reactivity. Pediatr Res 2006;60:705–10.
Newnham JP, Moss TJ, Nitsos I, Sloboda DM . Antenatal corticosteroids: the good, the bad and the unknown. Curr Opin Obstet Gynecol 2002;14:607–12.
De Matteo R, Blasch N, Stokes V, Davis P, Harding R . Induced preterm birth in sheep: a suitable model for studying the developmental effects of moderately preterm birth. Reprod Sci 2010;17:724–33.
Verhoeff FH . Some new staining methods of wide applicability. Including a rapid differential stain for elastic tissue. JAMA 1908;L:876–877.
Acknowledgements
The authors thank Victoria Stacy, Natasha Blasch, Ian Boundy, and Stefania Tombs for their assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bensley, J., De Matteo, R., Harding, R. et al. Preterm birth with antenatal corticosteroid administration has injurious and persistent effects on the structure and composition of the aorta and pulmonary artery. Pediatr Res 71, 150–155 (2012). https://doi.org/10.1038/pr.2011.29
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2011.29
This article is cited by
-
Dexamethasone induces an imbalanced fetal-placental-maternal bile acid circulation: involvement of placental transporters
BMC Medicine (2021)
-
Is late-preterm birth a risk factor for hypertension in childhood?
European Journal of Pediatrics (2014)
