
Abstract
Previous studies suggest postnatal blood pressure in preterm infants to be decreased by chorioamnionitis and increased by antenatal steroids (AS). We examined the adjusted effects of both antenatal modulators on postnatal blood pressure (BP), with separate effects reported for histologic chorioamnionitis with or without fetal involvement and timing of AS. General characteristics, BP, and heart rate values during the first 72 h after birth were obtained from 271 infants with gestational age ≤32.0 wk. In unadjusted analyses, chorioamnionitis was associated with lower BP, most prominently so in infants with fetal involvement, without an effect on hypotension incidence. AS increased BP and decreased the incidence of hypotension when administered within 7 d before birth. In a multivariable mixed model analysis, the AS effect remained significant, whereas chorioamnionitis was not independently predictive of postnatal BP. Other variables associated with increased postnatal BP were gestational age and umbilical artery pH, whereas hemolysis, elevated liver enzymes, low platelets syndrome was associated with decreased BP. In conclusion, AS seem to increase postnatal BP and decrease hypotension in preterm infants when given within 7 d before birth. Conversely, chorioamnionitis did not significantly affect postnatal BP after multivariable adjustment.
Similar content being viewed by others

Main
Early postnatal blood pressure is an important modulator of adverse outcome in preterm infants. In this population, low postnatal BP has been linked to the development of intraventricular hemorrhage (IVH) (1–8), ischemic cerebral lesions (3), adverse neurodevelopmental outcome (7,9,10), and neonatal mortality (3,4,7,10). BP regulation in preterm infants is complex and poorly understood, and several perinatal factors have been shown to influence postnatal BP in preterm infants. BP generally increases with advancing gestational age and increasing birth weight (1,2). Additional perinatal factors reported to influence postnatal BP include chorioamnionitis and antenatal steroid (AS) exposure (6,10).
Chorioamnionitis is an antenatal inflammatory state of the uterine environment, reflected in a histologic picture of polymorphonuclear infiltration of the placenta and associated membranes (11). Chorioamnionitis has been associated with adverse neonatal outcome, most consistently so regarding the preterm brain (12,13). Increased incidences of IVH, periventricular leukomalacia, cerebral palsy, and adverse neurodevelopmental outcome all have been described (13). Although inflammatory mechanisms have been shown to play a role in these associations, the pathophysiology remains largely unclear (13). A number of studies have addressed the question as to whether postnatal hypotension could provide a link between chorioamnionitis and adverse outcome. Indeed, lower mean and diastolic BPs (14), higher incidence of hypotension (15), and increased use of volume expansion and catecholamines (16) all have been reported in infants with histologic chorioamnionitis or funisitis. However, others have failed to reproduce these findings (17).
Although postnatal hypotension may provide a link between chorioamnionitis and adverse outcome, the positive effect of AS exposure on neonatal outcome could relate to an increase in blood pressure. Indeed, AS have been associated with increased postnatal BP in preterm infants (6,10,18,19). Correspondingly, the incidence of hypertension has been reported to increase (20), whereas both hypotension and the need for treatment of hypotension decrease (6,7,18,21–23) with AS. Conversely, not all studies confirm the positive effect of AS on postnatal BP (8,24) and the need for treatment of hypotension (17). Although part of these discrepancies may be explained by differences in timing of AS administration, no study has specifically addressed this issue.
Although chorioamnionitis and AS seem to have opposite effects on postnatal BP in preterm infants, few studies have reported adjusted effects of both modulators in a multivariable modeling framework. Our aim was to evaluate both the unadjusted and adjusted effects of chorioamnionitis and AS timing on postnatal BP during the first 72 h after birth. Because chorioamnionitis with fetal involvement is thought to represent the more serious side of the continuum of intrauterine inflammation, distinct effects of chorioamnionitis with or without fetal involvement are examined. In a mixed model analysis, multivariable testing of potential perinatal modulators of postnatal BP is performed in a nonlinear time-dependent fashion.
METHODS
Design.
This study is nested within a prospective observational cohort study reported previously (25). All pregnant women delivering between May 2001 and February 2003 in the Erasmus MC-Sophia Children's Hospital, Rotterdam, The Netherlands, at gestational ages of 32.0 wk or less, were eligible for the study. Enrollment was made immediately after delivery when newborns were admitted to the NICU. Antenatal, perinatal, and neonatal data were prospectively stored in a database with completion of data from neonates transferred to other hospitals.
General patient characteristics.
We used the following clinical definitions. Clinical chorioamnionitis: maternal temperature more than 38.0°C with two or more of the following criteria: uterine tenderness, malodorous vaginal discharge, maternal leukocytosis (white blood cell count >15,000 cells/μL), raised serum C-reactive protein, maternal tachycardia (>100 beats/min) and fetal tachycardia (>160 beats/min), and no other focus for infection. Preeclampsia: new-onset hypertension (BP >140/90 mm Hg or mean arterial pressure >105 mm Hg) and proteinuria with or without edema. Hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome: clinical presentation of intravascular hemolysis, elevated liver enzymes, and low platelet count. Respiratory distress syndrome (RDS): a clinical presentation (expiratory grunting, sub-/intercostal or sternal retractions, nasal flaring, tachypnea, cyanosis in room air, with or without apnea) and characteristic radiographic appearance according to Giedion et al. (26). Bronchopulmonary dysplasia: dependency on oxygen supplementation at a postmenstrual age of 36 wk. IVH and cystic periventricular leukomalacia were defined according to Volpe (27). Early-onset sepsis: clinical presentation of sepsis with raised C-reactive protein during the first 72 h of life. Necrotizing enterocolitis was defined as stage 2 or higher according to Bell et al. (28). Patent ductus arteriosus: persistence of the open ductus arteriosus postnatally as demonstrated by ultrasonographic examination. Gestational age was estimated by ultrasonography or by using the last menstrual period when reliable.
Antenatal steroids and chorioamnionitis.
Women received AS (betamethasone 12 mg i.m., repeated after 24 h) in case of imminent premature delivery. Timing of the last dose was recorded and used in further analyses. Thus, AS were considered to have been administered within 24 h before birth, when either a first dose or the second dose had been given within that period. Repeat courses of AS were not administered during the study period.
Placentas and membranes were fixed in formalin for at least 16 h immediately after delivery. Sampling was performed according to a standard protocol with two membrane rolls, two cross-sections of the cord, and three representative blocks of the placental disk as a minimum. The tissues were embedded in paraffin until histopathologic examination. To prevent interexaminer variation, the same pathologist (RRDK) examined all placentas for histologic evidence of infection. The pathologist was blinded for clinical information. Placental infection was categorized according to the stages of maternal and fetal inflammatory response as suggested by the Amniotic Fluid Infection Nosology Committee (11). Accordingly, fetal involvement was diagnosed when any of the following was present: chorionic vasculitis, umbilical phlebitis or vasculitis, (subacute) necrotizing funisitis, or concentric umbilical perivasculitis.
Blood pressure and heart rate.
Heart rate and both diastolic and mean BPs were recorded at regular intervals during the first 72 h after birth. BP was measured using a pressure transducer connected to an intra-arterial catheter or oscillometry when an intra-arterial catheter was absent. For each patient, mean values per 4-h period for both BP and heart rate were computed and used in further analyses. Hypotension was considered to be present when the mean BP (in mm Hg) was lower than the gestational age at birth (in wks) (29). For statistical analyses, the population was divided into separate groups depending either on AS timing or on presence of chorioamnionitis with or without fetal involvement.
Statistics.
Continuous data are expressed as mean ± SD. Differences between groups were tested using χ2 test for dichotomous data and one-way ANOVA for continuous data. Dunnett's post hoc analysis was used for multiple group comparisons. Variables shown to be significantly different among the groups of interest were kept in the linear model to warrant adjustment, irrespective of their significance as BP predictors.
To evaluate the adjusted effect of the main predictors on the BP and the change in BP over time, a generalized linear mixed model analysis was conducted. Individual infants were considered as random factor. A random intercept and random slope model (unstructured covariance structure) allowed for individual differences both in initial BP as well as in the course of its changes during the 3 d to be modeled. The variables displayed in Table 3 constituted the fixed effects part in the model. A top-down procedure was handled to select the variables in the final model. Model parameters were estimated via the restricted maximum likelihood method. All analyses were performed using the SPSS 15.0 computer program.
Ethical aspects.
The study was approved by the Medical Ethics Committee for Research on Human Subjects of the Erasmus University Medical Centre, Rotterdam, The Netherlands. Written parental consent was obtained.
RESULTS
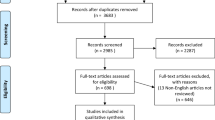
BP and heart rate data were collected from 271 of 301 infants included in the parent study (25). A total of 7574 individual BP measurements were included, 73% of which were derived from intra-arterial measurements. The need for indomethacin treatment for patent ductus arteriosus within the study period was not associated with changes in mean BP or incidence of hypotension at any time point (data not shown).
Chorioamnionitis.
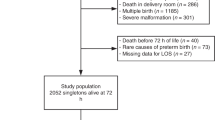
Histologic chorioamnionitis was present in 109 (40.2%) infants and accompanied by fetal involvement in 59 (21.8%). Infants with chorioamnionitis both with and without fetal involvement were more premature and had lower rates of HELLP and preeclampsia but higher rates of PPROM and clinical chorioamnionitis (Table 1). Infants with chorioamnionitis with fetal involvement had higher rates of necrotizing enterocolitis, IVH, and neonatal mortality, whereas early-onset sepsis was more frequent in those without fetal involvement. Importantly, there were no differences between the two groups in any of the treatments needed for circulatory disturbances (Table 1) or administration of morphine (data not shown).
Blood pressure and heart rate: unadjusted effects.
Infants with chorioamnionitis had higher heart rates than those without chorioamnionitis during the first 12 h of life, most prominently so directly after birth (Fig. 1A). Because of great similarity in temporal pattern between diastolic and mean BP, further analyses were performed using only mean BP values. Mean BP tended to be lower in infants with chorioamnionitis during the whole study period, most prominently so for those with fetal involvement (Fig. 1A). No significant differences in the incidence of hypotension during the first 3 days after birth were present among the three groups (Fig. 1B).

A, Heart rate and mean blood pressure during the first three postnatal days for infants divided by histologic signs of chorioamnionitis (HC) with or without fetal involvement (F) (HC−: open circle, dashed line; HC+F−: closed circle, dashed line; HC+F+: closed circle, continuous line). Points represent means ± SEM per 4-h period. B, Percentage of infants with hypotension during the first 3 postnatal days. Subgroups defined by presence of histologic signs of chorioamnionitis (HC) with or without fetal involvement (F) (HC−: black bars; HC+F−: white bars; HC+F+: gray bars). *p < 0.05, **p < 0.01, †p < 0.001 vs HC−.
Antenatal steroids.
Of infants included in the study, 227 (83.8%) received AS. In this group, exact timing of AS administration was documented in 193 (85.0%). The last dose was administered <24 h before birth in 77 (39.9%), between 2 and 7 d before birth in 72 (37.3%), and >7 d before birth in 44 (22.8%). There were no significant differences in general characteristics or circulatory treatment between groups based on timing of AS administration (Table 2). Administration of steroids between 2 and 7 d before birth was associated with decreased RDS incidence (Table 2).
Blood pressure and heart rate: unadjusted effects.
No important heart rate differences were present between groups during the study period (Fig. 2A). Clearly, steroid administration between 2 and 7 d before birth was associated with higher mean BP during the first 48 h after birth (Fig. 2A). Moreover, steroid administration, both within 24 h before birth and between 2 and 7 d before birth, was associated with a significant reduction in the incidence of hypotension at day 0 (Fig. 2B). Noteworthy is that on each day, the highest rate of hypotension was present in infants exposed to steroids >7 d before birth.

A, Heart rate and mean blood pressure during the first three postnatal days for infants divided by timing of antenatal steroid (AS) administration (no AS: open circle, dashed line; AS <24 h before birth: open circle, continuous line; AS 1–7 d before birth: closed circle, dashed line; AS >7 d before birth: closed circle, continuous line). Points represent means ± SEM per 4-h period. B, Percentage of infants with hypotension during the first three postnatal days. Subgroups defined by timing of antenatal steroid administration (no AS: black bars; AS <24 h before birth: white bars; AS 1–7 d before birth: gray bars; AS >7 d before birth: hatched bars). *p < 0.05, **p < 0.01, †p < 0.001 vs “no AS.”
Multivariable analyses.
To determine the adjusted effects of chorioamnionitis and AS on postnatal BP during the first 3 days after birth, a mixed model analysis was performed. Figures 1 and 2 hint at a curvilinear relationship between BP and time. Hence, to improve linearity of the BP-time association, time was log transformed (natural logarithm). A model with random intercept and random slope (unstructured covariance structure) was used, whose variances components values were 20.827, 3.055, −5.508, and 18.270 for random intercept, slope, and their covariance and residual, respectively.
The estimates of the fixed effects for each determinant in the final model are shown in Table 3. As expected, postnatal BP was significantly associated with both gestational age and time (on the Ln scale). AS administration <24 h before birth and, more prominently so, steroid exposure between 2 and 7 d before birth was associated with significantly increased BP. For visualization purposes, BP values during the first three postnatal days as predicted by the model for groups based on timing of AS administration are shown in Figure 3. Furthermore, umbilical artery pH was positively associated with postnatal BP, whereas maternal HELLP syndrome was associated with a significant decrease in BP (Table 3). Noticeably, chorioamnionitis either with or without fetal involvement did not significantly affect postnatal BP after multivariable adjustment.

Predicted mean blood pressure values during the first three postnatal days for groups based on timing of antenatal steroid (AS) administration (no AS: open circle, dashed line; AS <24 h before birth: open circle, continuous line; AS 1–7 d before birth: closed circle, dashed line; AS >7 d before birth: closed circle, continuous line). Points represent mean predicted values ± SEM. Values predicted from mixed model analysis displayed in Table 3.
DISCUSSION
In this large prospective cohort of preterm infants, we found that exposure to AS within the last week before birth is associated with increased postnatal BP and a decreased incidence of hypotension. Histologic chorioamnionitis, either with or without fetal involvement, did not significantly affect BP, incidence of hypotension, or need for BP support after birth in these infants. Instead, HELLP syndrome emerged as a significant negative modulator of postnatal BP.
Our findings are in line with earlier reports of a positive association between AS exposure and postnatal BP in preterm infants (6,10,18,19). Likewise, animal experimental data show an increase in BP after maternal steroid administration in preterm fetuses (30–33) and newborn animals (33,34). To our knowledge, the effect of timing of AS has not been reported before. Disregarding this temporal dimension may explain the inability of some reports to demonstrate an overall association between steroid exposure and postnatal BP (8,24). This is important, because our data suggest that the effect of AS exposure on postnatal BP is indeed time dependent. In this light, the high incidence of hypotension in infants exposed to steroids >7 d before birth is of concern and warrants further investigation. An attenuation of the endogenous corticosteroid response because of inhibition of the hypothalamic-pituitary-adrenal axis after exogenous steroid exposure may offer a possible explanation for this effect.
Although AS are known to reduce RDS at least partly through a stimulation of surfactant secretion, the mechanisms behind their effect in reducing the incidences of IVH and neonatal mortality remain largely obscure (35). Given the association between hypotension and adverse outcome in preterm infants, the decreased incidence of hypotension after AS exposure during the last week before birth found in our study may explain part of these effects (1–10). However, no significant improvement of neonatal outcome other than RDS was observed in our population.
Circulatory disturbance is a common finding in inflammatory processes related to infection such as sepsis because of a variety of mechanisms (36). Likewise, chorioamnionitis is an inflammatory process associated with increased cord blood levels of a whole range of cytokines, chemokines, and other proinflammatory proteins (37). In a small study, Yanowitz et al. (14) found an association among chorioamnionitis, elevated IL-6 cord blood levels, and lower early postnatal BP in preterm infants. In line with this observation, Lee et al. (15 reported a relationship between chorioamnionitis and hypotension on the first postnatal day). Others found no significant effect of chorioamnionitis with fetal involvement on early postnatal BP in extremely preterm infants, although both catecholamine use and cumulative volume load were increased (16). Given these observations, the absence of an effect of chorioamnionitis in our study is surprising. Possible explanations for this discrepancy include a shorter sampling period in earlier studies (14–16), differences in hypotension criteria (15) and population characteristics (16), and not accounting for effects of potential confounders (14,16). The importance of the latter is further emphasized by our findings. That is, in unadjusted analyses chorioamnionitis was associated with lower BP, whereas our multivariable model suggests that this may largely be due to the lower gestational age in this group. Taken together, our findings do not seem to imply an important role of neonatal BP modulation in the etiology of adverse outcome after chorioamnionitis.
Although HELLP and umbilical artery pH were not the main variables of interest in this study, their emergence as significant modulators of postnatal BP in preterm infants is interesting. The positive association between umbilical artery pH and BP is in agreement with the recognized relationship between perinatal asphyxia and subsequent hypotension (38). Data regarding neonatal BP in infants born to mother with HELLP are scarce. We are aware of one study showing HELLP to be associated with a higher need for volume expansion and a trend toward more hypotension on day 1 in preterm infants (39). Our results point in the same direction and may provide a link between HELLP syndrome and adverse outcome in preterm infants (40), although data concerning the latter are conflicting. Whether the association between HELLP and lower BP represents a direct disease-specific effect or is due to a maternal administration of antihypertensive medication needs further study.
To allow for nonlinear time-dependent modeling of postnatal BP pressure with concurrent adjustment for potential confounders, a mixed model analysis was used in this study. To our knowledge, this approach is unique in the evaluation of perinatal modulators of neonatal BP. Although many earlier studies reported unadjusted effects on BP of a single perinatal factor, a multivariable modeling approach allows for disentanglement of the distinct effects that potential modulators may have. Together with the relatively large cohort size, this strengthens the conclusions drawn from this study.
Several considerations need to be taken into account when interpreting the results. First, the effect of treatment for hypotension was not accounted in our analyses. However, in this light, the absence of treatment differences between groups is reassuring. Furthermore, when quantifying BP, the actual variable of interest is tissue perfusion. Clearly, the correlation between the two is far from perfect, and at best, BP may be considered a surrogate measure of the latter. Accordingly, hypotension is not a perfect representation of poor tissue perfusion. Moreover, there is considerable debate about the most appropriate definition of hypotension and likewise, about its management (41,42). Our data further support the use of individualized thresholds for hypotension (41), given the important BP changes observed over time and effects of perinatal variables such as gestational age and birth weight. Additional studies using other markers of tissue perfusion are needed to further evaluate the relationships among perinatal factors, circulatory regulation, and neonatal outcome.
In conclusion, we were unable to confirm earlier reports of an association between chorioamnionitis and lower postnatal BP in preterm infants. Instead, we present evidence for a time-dependent stimulatory effect of AS on neonatal BP, associated with a decrease in hypotension. The large cohort size and use of temporal analysis with adjustment for potential confounders strengthen our findings. Improved cardiovascular stability may in part mediate the reduction in adverse outcome after AS.
Abbreviations
- HELLP:
-
hemolysis, elevated liver enzymes, low platelets
- IVH:
-
intraventricular hemorrhage
References
Bada HS, Korones SB, Perry EH, Arheart KL, Ray JD, Pourcyrous M, Magill HL, Runyan W III, Somes GW, Clark FC, Tullis KV 1990 Mean arterial blood pressure changes in premature infants and those at risk for intraventricular hemorrhage. J Pediatr 117: 607–614
Cunningham S, Symon AG, Elton RA, Zhu C, McIntosh N 1999 Intra-arterial blood pressure reference ranges, death and morbidity in very low birthweight infants during the first seven days of life. Early Hum Dev 56: 151–165
Miall-Allen VM, de Vries LS, Whitelaw AG 1987 Mean arterial blood pressure and neonatal cerebral lesions. Arch Dis Child 62: 1068–1069
Fujimura M, Salisbury DM, Robinson RO, Howat P, Emerson PM, Keeling JW, Tizard JP 1979 Clinical events relating to intraventricular haemorrhage in the newborn. Arch Dis Child 54: 409–414
Watkins AM, West CR, Cooke RW 1989 Blood pressure and cerebral haemorrhage and ischaemia in very low birthweight infants. Early Hum Dev 19: 103–110
Moise AA, Wearden ME, Kozinetz CA, Gest AL, Welty SE, Hansen TN 1995 Antenatal steroids are associated with less need for blood pressure support in extremely premature infants. Pediatrics 95: 845–850
Fanaroff JM, Wilson-Costello DE, Newman NS, Montpetite MM, Fanaroff AA 2006 Treated hypotension is associated with neonatal morbidity and hearing loss in extremely low birth weight infants. Pediatrics 117: 1131–1135
Cordero L, Timan CJ, Waters HH, Sachs LA 2002 Mean arterial pressures during the first 24 hours of life in < or = 600-gram birth weight infants. J Perinatol 22: 348–353
Low JA, Froese AB, Galbraith RS, Smith JT, Sauerbrei EE, Derrick EJ 1993 The association between preterm newborn hypotension and hypoxemia and outcome during the first year. Acta Paediatr 82: 433–437
Batton B, Zhu X, Fanaroff J, Kirchner HL, Berlin S, Wilson-Costello D, Walsh M 2009 Blood pressure, anti-hypotensive therapy, and neurodevelopment in extremely preterm infants. J Pediatr 154: 351–357. e1
Redline RW, Faye-Petersen O, Heller D, Qureshi F, Savell V, Vogler C 2003 Amniotic infection syndrome: nosology and reproducibility of placental reaction patterns. Pediatr Dev Pathol 6: 435–448
Been JV, Zimmermann LJ 2009 Histological chorioamnionitis and respiratory outcome in preterm infants. Arch Dis Child Fetal Neonatal Ed 94: F218–F225
Dammann O, Leviton A 2004 Inflammatory brain damage in preterm newborns—dry numbers, wet lab, and causal inferences. Early Hum Dev 79: 1–15
Yanowitz TD, Jordan JA, Gilmour CH, Towbin R, Bowen A, Roberts JM, Brozanski BS 2002 Hemodynamic disturbances in premature infants born after chorioamnionitis: association with cord blood cytokine concentrations. Pediatr Res 51: 310–316
Lee SY, Ng DK, Fung GP, Chow CB, Shek CC, Tang PM, Shiu YK, Yu VY 2006 Chorioamnionitis with or without funisitis increases the risk of hypotension in very low birthweight infants on the first postnatal day but not later. Arch Dis Child Fetal Neonatal Ed 91: F346–F348
Furukawa S, Sameshima H, Ikenoue T 2008 Circulatory disturbances during the first postnatal 24 hours in extremely premature infants 25 weeks or less of gestation with histological fetal inflammation. J Obstet Gynaecol Res 34: 27–33
Laughon M, Bose C, Allred E, O'Shea TM, Van Marter LJ, Bednarek F, Leviton A 2007 Factors associated with treatment for hypotension in extremely low gestational age newborns during the first postnatal week. Pediatrics 119: 273–280
Demarini S, Dollberg S, Hoath SB, Ho M, Donovan EF 1999 Effects of antenatal corticosteroids on blood pressure in very low birth weight infants during the first 24 hours of life. J Perinatol 19: 419–425
Kari MA, Hallman M, Eronen M, Teramo K, Virtanen M, Koivisto M, Ikonen RS 1994 Prenatal dexamethasone treatment in conjunction with rescue therapy of human surfactant: a randomized placebo-controlled multicenter study. Pediatrics 93: 730–736
Seliem WA, Falk MC, Shadbolt B, Kent AL 2007 Antenatal and postnatal risk factors for neonatal hypertension and infant follow-up. Pediatr Nephrol 22: 2081–2087
Hall RW, Kronsberg SS, Barton BA, Kaiser JR, Anand KJ 2005 Morphine, hypotension, and adverse outcomes among preterm neonates: who's to blame? Secondary results from the NEOPAIN trial. Pediatrics 115: 1351–1359
1981 Effect of antenatal dexamethasone administration on the prevention of respiratory distress syndrome. Am J Obstet Gynecol 141: 276–287
Elimian A, Figueroa R, Spitzer AR, Ogburn PL, Wiencek V, Quirk JG 2003 Antenatal corticosteroids: are incomplete courses beneficial?. Obstet Gynecol 102: 352–355
LeFlore JL, Engle WD, Rosenfeld CR 2000 Determinants of blood pressure in very low birth weight neonates: lack of effect of antenatal steroids. Early Hum Dev 59: 37–50
Been JV, Rours IG, Kornelisse RF, Lima Passos V, Kramer BW, Schneider TA, de Krijger RR, Zimmermann LJ Histologic chorioamnionitis, fetal involvement and antenatal steroids: effects on neonatal outcome in preterm infants. Am J Obstet Gynecol, 2009 Sep 1, [Epub ahead of print]
Giedion A, Haefliger H, Dangel P 1973 Acute pulmonary X-ray changes in hyaline membrane disease treated with artificial ventilation and positive end-expiratory pressure (PEP). Pediatr Radiol 1: 145–152
Volpe JJ 2001 Neurology of the newborn. Saunders, Philadelphia pp 331–394
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, Brotherton T 1978 Neonatal necrotizing enterocolitis. therapeutic decisions based upon clinical staging. Ann Surg 187: 1–7
1992 Development of audit measures and guidelines for good practice in the management of neonatal respiratory distress syndrome. Report of a Joint Working Group of the British Association of Perinatal Medicine and the Research Unit of the Royal College of Physicians. Arch Dis Child 67: 1221–1227
Quaedackers JS, Roelfsema V, Fraser M, Gunn AJ, Bennet L 2005 Cardiovascular and endocrine effects of a single course of maternal dexamethasone treatment in preterm fetal sheep. BJOG 112: 182–191
Schwab M, Coksaygan T, Samtani MN, Jusko WJ, Nathanielsz PW 2006 Kinetics of betamethasone and fetal cardiovascular adverse effects in pregnant sheep after different doses. Obstet Gynecol 108: 617–625
Koenen SV, Mecenas CA, Smith GS, Jenkins S, Nathanielsz PW 2002 Effects of maternal betamethasone administration on fetal and maternal blood pressure and heart rate in the baboon at 0.7 of gestation. Am J Obstet Gynecol 186: 812–817
Segar JL, Bedell KA, Smith OJ 2001 Glucocorticoid modulation of cardiovascular and autonomic function in preterm lambs: role of ANG II. Am J Physiol Regul Integr Comp Physiol 280: R646–R654
Berry LM, Polk DH, Ikegami M, Jobe AH, Padbury JF, Ervin MG 1997 Preterm newborn lamb renal and cardiovascular responses after fetal or maternal antenatal betamethasone. Am J Physiol 272: R1972–R1979
Roberts D, Dalziel S 2006 Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 3: CD004454
Rittirsch D, Flierl MA, Ward PA 2008 Harmful molecular mechanisms in sepsis. Nat Rev Immunol 8: 776–787
Paananen R, Husa AK, Vuolteenaho R, Herva R, Kaukola T, Hallman M 2009 Blood cytokines during the perinatal period in very preterm infants: relationship of inflammatory response and bronchopulmonary dysplasia. J Pediatr 154: 39–43. e3
Low JA 2004 Determining the contribution of asphyxia to brain damage in the neonate. J Obstet Gynaecol Res 30: 276–286
Dotsch J, Hohmann M, Kuhl PG 1997 Neonatal morbidity and mortality associated with maternal haemolysis elevated liver enzymes and low platelets syndrome. Eur J Pediatr 156: 389–391
Kim HY, Sohn YS, Lim JH, Kim EH, Kwon JY, Park YW, Kim YH 2006 Neonatal outcome after preterm delivery in HELLP syndrome. Yonsei Med J 47: 393–398
Dempsey EM, Barrington KJ 2007 Treating hypotension in the preterm infant: when and with what: a critical and systematic review. J Perinatol 27: 469–478
Evans JR, Lou Short B, Van Meurs K, Cheryl Sachs H 2006 Cardiovascular support in preterm infants. Clin Ther 28: 1366–1384
Acknowledgements
We thank A. Schneider, F. Jonkers, P. van Felius, and E. Oschatz-Overbosch for their help in data collection and database design.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by Revolving Fund, Erasmus MC Rotterdam, and Jasper V. Been is supported by a “Profileringsfonds” grant from the Maastricht University Medical Centre.
Rights and permissions
About this article
Cite this article
Been, J., Kornelisse, R., Rours, I. et al. Early Postnatal Blood Pressure in Preterm Infants: Effects of Chorioamnionitis and Timing of Antenatal Steroids. Pediatr Res 66, 571–576 (2009). https://doi.org/10.1203/PDR.0b013e3181b7c4da
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e3181b7c4da
This article is cited by
-
Antenatal and perinatal factors influencing neonatal blood pressure: a systematic review
Journal of Perinatology (2021)
-
Determinants of Neonatal Blood Pressure
Current Hypertension Reports (2013)
-
Cerebral autoregulation in the first day after preterm birth: no evidence of association with systemic inflammation
Pediatric Research (2012)
-
Chorioamnionitis: a multiorgan disease of the fetus?
Journal of Perinatology (2010)
