
Abstract
Measurements of body composition are being made increasingly widely in pediatrics. Tetrapolar whole body impedance (BI) is particularly suitable as a method of estimating boyd composition in children and is therefore the subject of great interest at present. However, the ability of BI to accurately estimate fat-free mass (FFM) in children is unclear, and users of BI are faced with a growing choice of prediction equations for estimation of FFM. Studies in adults have suggested that choice of prediction equation can have a profound effect on the estimate obtained. The aim of the present study was to measure the ability of four published pediatric BI equations to predict FFM in 98 Caucasian prepubertal children (mean age 9.0 y). For three of the published equations, limits of agreement between predicted and reference FFM were wide and distinct biases were apparent. With mean FFM of 25 kg, the equation of L. Cordain et al. overestimated reference FFM (95% CI +2.1 to +3.1 kg), whereas those of P. Deurenberg et al. (95% CI -1.9 to -2.9 kg) and F. Schaefer et al. (95% CI -1.4 to -2.5 kg) systematically underestimated reference FFM. The equation of Houtkooper et al. (95% CI -0.2 to +0.8 kg) predicted FFM with negligible bias and had narrower limits of agreement relative to the reference method than the other three equations tested. We conclude that the ability of BI to predict body composition in children depends on the equation chosen and that the general applicability of BI equations cannot be safely assumed. Cross-validation of BI equations is recommended before they are used routinely for estimation of body composition in children.
Similar content being viewed by others

Main
Application of BI in pediatric populations is of great interest as it is a technique which is particularly suitable for the study of children, and there is increasing recognition of the importance of body composition in this age group(1, 2). Validity of BI relative to reference methods of measuring body composition is reportedly high(3, 4) in adults, although the point is disputed(5, 6). The contradictions in the literature arise in part from the wide range of impedance software and hardware used, the lack of cross-validity for some prediction equations(7, 8), and large biases between estimates derived from different commercial software(8). The principle of using BI for estimation of total body water and/or FFM in children is established(9, 10), but a number of doubts remain. Errors in estimation of FFM may be unacceptably high, and the technique may not offer improved estimation relative to anthropometry(10). In addition, users of BI in childhood are currently faced with a choice of at least four published, empirically derived, equations for prediction of FFM in addition to a range of commercial software and the rapid emergence of new equations(11). The cross-validity (general applicability) of the four currently published equations is unknown, but is in question because work on application of BI in adults has shown that cross-validity cannot be taken for granted(7, 8). The aim of the present study was therefore to test the ability of these four published equations to accurately estimate FFM in a group of prepubertal children in the UK, using hydrodensitometry with a variable density model(12) as the reference method.
METHODS
Subjects. The study sample consisted of 98 healthy, self-selected, prepubertal children, 64 boys (mean age 9.3 y, SD 1.7) and 34 girls (mean age 8.9 y, SD 1.6). Physical characteristics of subjects are given in Table 1. All subjects were in good health, and all but two were white. The sample was heterogenous with respect to body fatness(Table 1) and not greatly dissimilar from Scottish reference values for body mass index: in the girls, median body mass index centile relative to Scottish girls was 50, and in the boys, the median body mass index centile was 56(13).
Informed consent was obtained from all subjects and their parents before undertaking the study, and approval was obtained from the local Ethics Committee.
Anthropometry, measurement of body density, and estimation of reference FFM. Body weight was measured to 0.1 kg in swimsuit/swimming trunks using a standard beam balance. Height was measured to 0.5 cm using a Holtain wall-mounted stadiometer. In 57 of the boys and 24 of the girls, body density was measured in triplicate by hydrodensitometry, as previously described(14). In 7 of the 64 boys and 10 of the 34 girls, density measurements could not be performed adequately, and their data were restricted to comparisons between prediction equations. They were not included in the comparisons between the prediction and reference method. Measured body density was converted to FFM using the model described by Westrate and Deurenberg(12) which assumes changing FFM density during childhood. Density-derived estimates of FFM were then used as the reference method against which the impedance-derived estimates were validated.
BI measurements. All subjects abstained from eating, drinking, and vigorous exercise for at least 3 h before BI measurement, and measurements were carried out after voiding and 5 min of bed rest. In all 98 children, whole body electrical impedance was measured on the right-hand side of the body with the child supine using standard 800 mAmp and 50 kHz current. The Bodystat 500 system (Bodystat Limited, Isle of Man, UK) was used for BI measurements, because its technical validity had been established by us and others(15) before the study, and measured impedance values can be incorporated into prediction equations separately from the manufacturers software. In 10 of the children BI measurements were repeated within 3 d of the initial measurements (under the same conditions) for the purpose of assessing measurement precision.
The four equations tested were as follows.
-
1
Schaefer et al.(10): FFM (kg) = 0.15 + 0.65 (RI) + 0.68 (age, years)
-
2
Houtkooper et al.(16): FFM (kg) = 0.61 (RI) + 0.25 (weight, kg) + 1.31
-
3
Deurenberg et al.(17): FFM (kg) = 0.406 (RI) + (0.36 weight, kg) + 5.58 height (M) + 0.56 gender - 6.48 where gender is male = 1; female = 0.
-
4
Cordain et al.(18): FFM (kg) = 6.86 + 0.81 (RI).
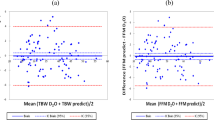
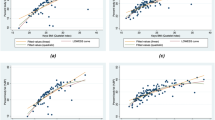
Statistical analysis. Agreement between estimates of FFM derived from hydrodensitometry and those derived from the four prediction equations tested was determined according to the method of Bland and Altman(19) by calculation of biases and limits of agreement. Standard 95% CI for the average difference between the reference method and the prediction are also presented. Relationships between bias in estimation of FFM and other variables (age, fatness, FFM) were assessed by the method of Bland and Altman(19).
RESULTS
Measurement precision. In the 10 children included in the assessment of precision, mean (SD) FFM was 26.4 (5.4) kg. The 95% CI for the difference in test-retest estimates of FFM was -0.5 to +0.4 kg, indicating that, on average, the paired difference between measurements was not significantly different from zero.
Comparison of four equations with densitometry. Some distinct biases in prediction were apparent, and limits of agreement relative to hydrodensitometry were wide (Table 2). FFM (densitometry) was systematically overestimated by the equation of Cordain et al.(95% CI +2.1 to +3.3 kg) and systematically underestimated by the equations of Deurenberg et al. (95% CI -1.9 to -2.9 kg) and Schaefer et al. (95% CI -1.4 to -2.5 kg). The equation of Houtkooper et al. predicted FFM with negligible bias (95% CI -0.2 to +0.8 kg) and narrower limits of agreement relative to densitometry than the other three equations.
For the equations of Houtkooper et al. (r = 0.07), Deurenberg et al. (r = 0.09), and Cordain et al.(r = 0.20; NS) there was little evidence of a relationship between bias and FFM size. For the equation of Schaefer et al. (r= 0.27, p < 0.05) there was such an association. There were no statistically significant relationships between errors in estimation and age or gender for any of the four equations. For the equations of Schaeferet al. (r = 0.00) and Cordain et al.(r = 0.06), there was no evidence of an association between bias and body fatness (as a percentage of body weight). Error in FFM estimation was significantly correlated with body fat percentage for the equations of Houtkooper et al. (r = 0.39) and Deurenberg et al. (r = 0.41; Fig. 1).

Differences between prediction equations.Table 2 provides a comparison of estimates of FFM of prediction equations relative to each other and confirms that estimates tended to be highest by the equation of Cordain et al.(18), followed by, in descending order, Houtkooperet al.(16), Schaefer et al.(10), and Deurenberg et al.(17). Because body composition is often considered as percentage of body fat, for additional information the group mean estimates of body composition expressed as body fatness (percent of body weight) are presented in Table 3. Errors are in the opposite direction to those for FFM. This analysis confirms the hypothesis that there are large differences in estimates of FFM and body fat percentage associated with choice of prediction equation.
DISCUSSION
BI is now widely used as a method of measuring body composition in children and in a variety of fields: epidemiology, clinical nutrition, and applied physiology. The present study, in common with other published work, suggests that the technique has reasonable precision under standardized conditions(10, 20, 25). However, establishing the validity of BI in childhood is more complicated. The reference method most commonly used in adults, densitometry, is difficult to apply in children. From a practical point of view, measurement of body density is not possible in all children, particularly in younger prepubertal children. Even with self-selection of subjects, we were operating at the limit of the age range over which accurate hydrodensitometry is possible. In our experience recruiting subjects under the age of 7 y was not productive because of their inability to perform the underwater weighing procedure adequately.
The “chemical immaturity” of children presents theoretical problems. FFM does not have constant composition in childhood, but shows systematic variation during development(21, 22), and there is probably relatively high inter-individual variability in FFM composition in children of similar age(23).“Variable density models” represent one attempt(2, 12) to incorporate this variability in FFM and are necessary if densitometry is used as a reference method in children. This was the approach taken in the present study with the caveats that 1) apparent differences between reference and alternative methods are increased by “error” in the reference method(24),2) multicomponent models may supersede densitometry as reference methods for pediatric use, and 3) any reference methods provide tests of relative rather than absolute validity because there is no“gold standard”(2).
The cross-validity of some published BI equations in adults is poor(7, 8), and differences in estimates by different published or commercial equations probably derive largely from the equations themselves rather than from technical error(8). Occasional reports in children have also indicated poor cross-validity of some published equations in ethnic groups(25) or populations(10, 26) other than that for which the equations were derived, or in children of different ages(17) or in disease states(20). In view of these doubts over the general applicability of published pediatric equations, the proliferation of new equations(11), and the widespread use of BI, a test of cross-validity was justified and should be considered desirable by critical users of the method. The present study suggests caution in the use of equations derived from the literature for prediction of FFM from impedance in prepubertal children. Choice of equation will be a major determinant of the estimate obtained. Most investigators would agree that systematic errors in estimation of >2 kg FFM with a mean of FFM 25 kg are undesirable(Table 2). Systematic differences of >4 kg FFM between prediction equations (Table 2) also underscore the need to use equations which are valid in the population in which the technique is being applied. In the present study commercial pediatric software for estimation of FFM from BI was not tested, because in the adult literature commercial software generally predicts body composition less accurately than prediction equations based on published studies(8), and because the origin of commercial software is usually unknown (in contrast to published studies).
The present study suggests that the equation of Houtkooper et al.(16) has a high degree of cross-validity and is suitable for use in Caucasian prepubertal children, below the age range used to derive the original equation. The equation of Houtkooper et al.(16) not only predicted FFM with negligible bias, but individual errors in estimation were considerably smaller than for the other equations currently available (Table 2) and must be considered acceptable in view of the errors inherent in the reference method(2, 24). Error arising out of the use of the Houtkooper et al.(16) equation was higher in boys than girls, and was related to the fatness of the child(Fig. 1), so there may still be some scope for adjustment of this equation to improve prediction. The other equations tested, although apparently valid in the populations in which they were derived, predicted FFM with statistically significant systematic errors and with larger random errors than did the Houtkooper et al. equation (Table 2). A detailed discussion of the source of differences between different pediatric prediction equations is beyond the scope of this report. However, differences in BI hardware as well as software(15), in premeasurement criteria(9, 17) in the reference method used, and in body composition (or even body shape) of children, between studies probably contributes to the failure of prediction equations to transfer between pediatric populations. It is also important to note that ethnicity may also be relevant(2, 16, 25) to failure of cross-validity and that disease states, particularly when associated with disturbance of water balance or distribution of body water, have a tendency to invalidate prediction equations derived from healthy populations. Finally, the present study is restricted largely to consideration of estimates of absolute body composition; the estimation of changes in body composition using BI is a complex and separate question(27).
In conclusion, BI is a simple technique that generates reasonably reproducible results in children. Choice of a prediction equation for particular purposes must be made carefully, and if validation of equations is not possible, the equation of Houtkooper et al.(16) might be the most appropriate of those currently available for estimating the FFM of prepubertal Caucasian children.
Abbreviations
- BI:
-
tetrapolar whole body impedance
- FFM:
-
fat-free mass
- RI:
-
resistance index (height(cm)2/resistance (ohms))
- CI:
-
confidence interval
References
Davies PSW 1994 Body composition assessment. Arch Dis Child 69: 337–338
Lohman TG 1993 Advances in Body Composition Assessment, Monograph No. 3. Human Kinetics Publishers, Champaign, IL
Lukaski HC, Bolonchuk WW, Hall CB, Siders WA 1986 Validation of tetrapolar bio-electrical impedance method to assess human body composition. J Appl Physiol 60: 1327–1332
Segal K, Van Loan M, Fitzgerald PI, Hodgson JA, Van Itallie TB 1988 Lean body mass estimation by bio-electrical impedance analysis: a four site cross-validation study. Am J Clin Nutr 47: 7–14
Fuller NJ, Jebb SA, Laskey MA, Coward MA, Elia M 1992 A four component model for the assessment of body composition in humans. Clin Sci 82: 687–693
Heitmann BL 1994 Impedance: a valid method in assessment of body composition?. Eur J Clin Nutr 48: 228–244
Reilly JJ, Murray LA, Wilson J, Durnin JVGA 1994 Measuring the body composition of elderly subjects: a comparison of methods. Br J Nutr 72: 33–44
Fuller NJ 1993 Comparison of abilities of various interpretations of bio-electrical impedance to predict reference method body composition assessment. Clin Nutr 12: 236–242
Deurenberg P, Kusters CS, Smith H 1990 Assessment of body composition by bio-electrical impedance in children and young adults is strongly age-dependent. Eur J Clin Nutr 44: 261–268
Schaefer F, Georgi M, Zieger A, Scharer K 1994 Usefulness of bio-electrical impedance and skinfold measurements in predicting fat-free mass derived from total body potassium in children. Pediatr Res 35: 617–624
Elia M 1993 The bio-impedance craze. Eur J Clin Nutr 47: 825–827
Westrate JA, Deurenberg P 1989 Body composition in children. Am J Clin Nutr 50: 1104–1115
White EM, Wilson AC, Greene SA, McCowan C, Thomas GE, Cairns AY, Ricketts IW 1995 Body mass index centile charts to assess fatness of British children. Arch Dis Child 72: 38–41
Durnin JVGA, Womersley J 1974 Body fat assessed from total body density and its estimation from skinfold thickness measurements in 481 men and women aged 16-72 years. Br J Nutr 32: 77–97
Smye SW, Sutcliffe J, Pitt E 1993 A comparison of four commerical systems used to measure whole body bio-electrical impedance. Physiol Meas 14: 473–478
Houtkooper LB, Going SB, Lohman TG, Roche AF, Van Loan M 1992 Bio-electrical impedance estimation of fat-free body mass in children and youth: a cross-validation study. J Appl Physiol 72: 366–373
Deurenberg P, Van der Kooy K, Leenan R, Westrate JC, Seidell JC 1991 Sex and age specific prediction formulas for estimating body composition. Int J Obesity 15: 17–24
Cordain L, Whicker RG, Johnson JE 1988 Body composition determination in children using bio-electrical impedance. Growth Dev Aging 52: 37–40
Bland JM, Altman DG 1986 Statistical methods for assessing agreement between two methods of clinical measurement. Lancet I: 307–310
Davies PSW, Joughin C 1992 Assessment of body composition in Prader-Willi syndrome using bio-electrical impedance. Am J Med Genet 44: 75–78
Fomon SJ, Haschke F, Ziegler EE, Nelson SE 1982 Body composition of reference children from birth to age 10 years. Am J Clin Nutr 35: 1169–1175
Lohman TG, Going SB, Slaughter MH, Boileau RA 1989 Concept of chemical immaturity in body composition estimates. Am J Hum Biol 1: 201–204
Hewitt MJ, Going SB, Williams DP, Lohman TG 1993 Hydration of fat-free body in children and adults: implications for body composition assessment. Am J Physiol 265:E88–E95
Siri WE 1961 Body composition from fluid spaces and density: analysis of methods. In: Brozek J, Henschel A (eds) Techniques for Measuring Body Composition. National Academy of Science, Washington, DC, pp 223–244
Kim HK, Tanaka K, Nakadomo F, Watanabe K 1994 Fat free mass in Japanese boys predicted from bio-electrical impedance and anthropometric variables. Eur J Clin Nutr 48: 482–489
Hammond J, Rona RJ, Chinn S 1994 Estimation in community surveys of total body fat of children using bio-electrical impedance or skinfold thickness measurements. Eur J Clin Nutr 48: 164–171
Jebb SA, Murgatroyd PR, Coward WA, Goldberg GR, Prentice AM 1993 In vivo measurement of changes in body composition. Am J Clin Nutr 58: 455–462
Acknowledgements
The authors thank the volunteers and their families, and the Institute of Physiology University of Glasgow for providing access to their laboratory facilities. Lawrence Weaver kindly commented on an earlier draft of the manuscript.
Author information
Authors and Affiliations
Additional information
Supported by a grant from the Scottish Office Home and Health Department.
Rights and permissions
About this article
Cite this article
Reilly, J., Wilson, J., McColl, J. et al. Ability of Biolectric Impedance to Predict Fat-Free Mass in Prepubertal Children. Pediatr Res 39, 176–179 (1996). https://doi.org/10.1203/00006450-199601000-00029
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199601000-00029
This article is cited by
-
Body composition during growth in children: limitations and perspectives of bioelectrical impedance analysis
European Journal of Clinical Nutrition (2015)
-
Development of bioelectrical impedance-derived indices of fat and fat-free mass for assessment of nutritional status in childhood
European Journal of Clinical Nutrition (2008)
-
Validity of Six Field and Laboratory Methods for Measurement of Body Composition in Boys
Obesity Research (2003)
-
Segmental bioelectrical impedance analysis in children aged 8–12 y: 1. The assessment of whole-body composition
International Journal of Obesity (2002)
-
Foot-to-foot bioelectrical impedance analysis: a valuable tool for the measurement of body composition in children
International Journal of Obesity (2001)
