
Abstract
Objective
To develop and validate equations that estimate total body water (TBW) and fat-free mass (FFM) in adults using anthropometric measurements.
Methods
A cross-sectional study was conducted among 178 adults (77 men and 101 women; aged 18–59 years). Participants were distributed by sex and age groups, and then randomly assigned to equal two groups; the development (n = 89) and the validation (n = 89). The anthropometric measurements included height and weight. The deuterium dilution technique (DDT) estimated TBW and FFM. Linear regression models were used with the TBW and FFM as the dependent variable, and height and weight as the independent variables. Cross-validation was performed by Bland and Altman plot, and the new anthropometric equations were developed.
Results
In the validation sample, the developed equations had high R2 of 94.4 for both TBW and FFM in all age groups, and low standard errors (RMSE: 1.80 kg for TBW and 2.44 kg for FFM). The pure error was 2.03 for the TBW equation and 2.71 for the FFM equation. The Bland–Altman plot illustrated the good level of concordance between the TBW and FFM predicted by the new equations as determined by DDT. The following developed equations showed a better agreement with the DDT:
\({{{\rm{TBW}}}}\left( {{{{\rm{kg}}}}} \right) = 0.0758 + 0.2979 \times {{{\rm{weight}}}} + 0.1234 \times {{{\rm{height}}}} - 0.0416 \times {{{\rm{age}}}} - 8.7113 \times {{{\rm{sex}}}}({{{\rm{men}}}} = 0,\,{{{\rm{women}}}} = 1)\);
\({{{\rm{FFM}}}}\left( {{{{\rm{kg}}}}} \right) = - 0.4475 + 0.4055 \times {{{\rm{weight}}}} + 0.1691 \times {{{\mathrm{height}}}} - 0.0459 \times {{{\mathrm{age}}}} - 11.7752 \times {{{\mathrm{sex}}}}({{{\mathrm{men}}}} = 0,\,{{{\mathrm{women}}}} = 1)\).
Conclusion
In this study, we developed and validated prediction equations for the estimation of TBW and FFM from DDT in healthy adult Tunisian population. The newly anthropometric prediction equations seem to be the most accurate for Tunisian adult.
Similar content being viewed by others


Introduction
Overweight and obesity are defined as abnormal or excessive accumulation of body fat, and excessive fatness is linked with non-communicable diseases of lifestyle. Nowadays, obesity is a major public health problem in both developed and developing countries. It is considered as a chronic progressive disease [1]. Recently, obesity amongst other comorbidities was reported to be a higher and a major risk factor associated with the severe Coronavirus disease 2019 (COVID-19) [2].
One of the most widely used methods for estimating body composition is the anthropometric measurements (skinfolds, waist circumference (WC), upper arm circumferences, body weight, etc.). Anthropometric parameters have long been used to assess nutritional status [3]. It is a convenient, non-inversive and quick way to assess body composition and requires minimal equipment. However, these parameters have limitations, for example, body weight alone cannot characterize the shape of the human body without taking into account the stature.
Body mass index (BMI) being a proxy measure for fatness is typically used to assess overweight and obesity in both clinical and field settings. Although BMI useful, it has serious limitations in the sense that it does not discriminate between fat mass (FM) and fat-free mass (FFM) [4, 5].
Importantly, accurately and valid assessment of body composition is essential for the assessment of nutritional and health status for the effectiveness of current and future nutritional interventions. As such, there are several available techniques for assessing body composition. These methods include anthropometry, bioelectrical impedance analysis (BIA), dual-energy X-ray absorptiometry, quantitative magnetic resonance imaging ultrasound and isotopes dilution technique [6, 7]. However, the selection of body composition technique in research is dependent of the feasibility and it advantages.
Deuterium dilution technique (DDT) is one of the reference methods for the measurement of total body water (TBW) to calculate FFM and FM based on 2-compartments model. The DDT has been applied in all ethnic groups and ages. However, DDT requires 3.5 to 6 h of patient time and addition special instrumental analysis, is not suitable for routine use [8]. It was therefore interesting to develop and validate a simple, rapid and non-invasive alternative approach for the estimation of FFM and FM [9, 10].
To date, a few prediction equations have been developed to estimate body composition using anthropometric variables from a simple measurement of height and weight combined with information on gender and age. However, it has been described that these equations are not valid in other populations with a different ethnic origin [11,12,13,14,15,16].
So, the main aim of our study, which is one of the fewer investigations to estimate the body composition in adults of Tunisian origin, was to assess the validity of previously published TBW, FFM, and anthropometric prediction equations against DDT in a sample of Tunisian adults; and to develop a new anthropometric equations to predict TBW and FFM as assessed by reference method.
Materials and methods
Studied population
A total of 178 subjects living in urban area in Tunisia were recruited from the Nutrition Department of the Higher School of Health Sciences and Techniques in Tunis. Recruitment was done using random sampling with the following inclusion criteria: (1) men and women aged ranging from 18 and 59 years old; (2) apparently healthy subjects. Participants with chronic illnesses were excluded from the study. All participants have similar demographic characteristics. All subjects were informed that their participation was voluntary. Participants were clearly informed of the study protocol and signed informed consent form. Confidentiality was maintained during measurements and data processing.
Anthropometric measurements
Anthropometric measurements were performed following the international recommendations [17].
Standing height was measured in the erect position without shoes with a mobile height gauge (ALTUREXATA®) graded in centimeters up to 2.13 m and within an accuracy of 0.1 cm. Weight was measured in minimum clothing without shoes to the nearest 0.1 kg using a portable scale (Seca, Hamburg, Germany, 896 (150 ± 0.1 kg)). BMI was calculated as weight in kilograms divided by height in meters squared (BMI: kg/m2). Participants were classified as underweight (BMI < 18.5 kg/m2), normal (BMI between 18.5 to 24.9 kg/m2) or overweight (BMI between 25 to 29.9 kg/m2) and obese (BMI ≥ 30 kg/m2) [18]. WC was measured with a 2 m long, flexible, inelastic anthropometric tape, divided into centimeters and subdivided into millimeters. WC was taken midway between the inferior margin of the last rib and the crest of the ilium in a horizontal plane (to the nearest 0.1 cm).
Assessment of body composition
TBW, FFM and FM of different subjects were measured by DDT. The collection of the samples and the analyses were undertaken according to the guidelines of the International Atomic Energy Agency (IAEA) [19, 20]. In fact, after asking subjects to empty their bladder, each participant provided pre-dose saliva using sterile anhydrous cotton rolls given by IAEA (GIMA, Italy). Saliva is collected in sterile tubes by compressing cotton in a syringe. Then, the participants drank, with a straw, a gravimetrically weighed amount of 60 g of 10% deuterium oxide at 99.8% atom excess based an amount of 0.1 g/kg of subject weight. The bottle containing the dose was rinsed twice with 50 ml of drinking water and fed to the adults in order to ensure that the participants received the entire isotope dose. During the time of equilibration of body water compartments, subjects could not have any food or drink, and could not perform any physical activity. A first post-dose saliva sample was collected from each participant after 3 h of dose administration and a second post-dose after 3.5 h. Samples were stored at −20 °C until analysis. The enrichment of deuterium in saliva samples was measured by Fourier transformed infrared spectrophotometer using FTIR (FTIR, Agilent 4500). Moreover, measurement of the serial dilution (range: 0–500 ppm) of our calibrator with our FTIR equipment showed a coefficient of correlation of 0.99, reflecting good precision of our FTIR method. In order to calibrate the FTIR, a standard solution of 1000 mg of deuterium oxide per kg of local tap water was prepared by gravimetry and analyzed at the beginning and at the end of each series of measurements. Deuterium enrichment in saliva samples were obtained compared to the standard. Saliva samples were completely thawed at room temperature, centrifuged to remove any solids, and analyzed twice. Two saliva sample readings measured by FTIR must have values that are within 3 ppm. After measuring the enrichment of saliva by the FTIR, the following calculations were performed to assess TBW, FFM and FM [20, 21]:
-
Deuterium dilution space (DDS) = the amount of deuterium oxide consumed/the enrichment (average of 3 and 3.5 h post-dose enrichment).
-
TBWDDT (kg) = DDS/non-aqueous exchange constant (1.041).
-
FFMDDT (kg) = TBWDDT/hydration factor (0.732 for subject aged >20 years, 0.738 for males and 0.745 for females aged 18–20 years) [21, 22].
-
FMDDT (kg) = Body weight − FFMDDT.
-
% FMDDT = (FMDDT/body weight) × 100.
Anthropometric based published prediction equations tested
In the present study, we tested the validity of previously published prediction equations and mainly those made for adults. Those equations were chosen according to their frequent mention in the literature and the age range of the population. Thus, five TBW equations were tested for the prediction of TBW: Hume and Weyers [11], Watson et al. [12], Slater and Preston [13], Medoua et al. [14], Chumlea et al. [15] and one equation for the determination of FFM: Janmahasation et al. [16] (Table 1).
Statistical analysis
Statistical analyses were performed using STATA 14 (StataCorp, College Station, TX, USA). Data were presented as mean ± standard deviations. To cross-validate the new anthropometric equation, the database was subdivided in development group (89 subjects) and validation group (89 subjects). The subdivision was done after classification of subjects by gender and age, then the subjects were randomly allocated to each sub-group. The differences between validation and development groups were evaluated using a two sample t-test. The stepwise linear regression method was used to predict TBW in kg and FFM in kg as dependent variables, whereas the independent variables were body weight in kg, height in cm, age in years and sex (men = 0, women = 1). Pearson’s correlation coefficients were used to study the relation between the measured and predicted values of TBW. The difference between measured and predicted values (bias) was tested against zero using paired t-test. The coefficient of determination (R2), the root mean square error (RMSE) and %RMSE (RMSE/mean FFM or TBW) were used to evaluate the precision of the equations. Bland and Altman [23] test was applied to evaluate the concordance between body composition results measured by using DDT and different prediction equations. The statistical significance was considered at p value <0.05.
Results
General characteristics
The physical and anthropometric characteristics and body composition parameters of all subjects and according to sex are presented in Table 2. In total 178 subjects (77 men, 101 women), aged 18 to 59 years participated in this study. The means of age, weight, height and BMI of the participants were, respectively, 29.2 ± 12.3 years, 69.4 ± 12.2 kg, 167.7 ± 10.4 cm and 24.75 ± 4.28 kg/m2. According to the BMI categories, 5.6% were underweight, 48.3% of the subjects were in a normal range, 33.2% were overweight and 12.9% were obese.
Prediction equations tested
The comparison of our results with those predicted equations using a previously published anthropometric equations, is presented in Table 3.
All equations for the estimation of TBW, except that of Slater and Preston, showed significant differences in all subjects, and in men and women. Indeed, TBW predicted by the equations of Hume and Weyers [11], Watson et al. [12], Medoua et al. [14] and Chumlea et al. [15] significantly (p < 0.0001) overestimated TBW in the total sample with a positive bias value (2.50, 1.67, 5.34 and 5.15 kg, respectively for each equation). However, Slater’s equation gave a non-significant difference in all subjects (p = 0.94), but in terms of sex, the Slater inbuilt equation significantly (p = 0.0089) overestimated TBW in women with a bias of 1.06 ± 4.00 kg and (p = 0.0018) underestimate TBW in men.
Body composition in the development and validation groups
Table 2 shows the characteristics of studied participants and subgroups (development and validation groups). There were no significant differences observed in anthropometric variables and different compartments of body compositions assessed by DDT between the development group (n = 89) and the validation group (n = 89). The mean of TBW was 35.3 kg with a range of 23.2 to 55.6 kg, the mean of FFM was 48.1 kg with a range of 30.7 to 76.0 kg and the mean of FM and %FM were respectively 21.3 kg and 30.3% with a range of 4.1–45.7 kg and 7.8–50.0%.
Development of the equations
The prediction equations were derived by stepwise linear multiple regression and the results for this prediction equation are presented in Table 4. The TBW (kg) and FFM (kg) were the dependent variables in their respective equation. Weight, height, sex and age were the significant predictors variables included in the equations. The weight, age, and sex considerably added to the accuracy of our equations and improved r and RMSE.
The prediction equations derived were:
where TBW in kg; FFM in kg; Weight in kg; Height in cm; sex in dummy code (men = 0, women = 1) and age in years.
In the TBW prediction equation, the values of R2, RMSE, and % RMSE are 0.94, 1.80 kg, and 5.08% respectively, while the same parameters of the FFM prediction equation were of 0.94, 2.44 kg and 5.05% respectively (Table 4).
Validation of the prediction equations
In the validation group, the use of the paired t-test showed that there was no significant (p > 0.05) difference between TBW (35.4 ± 7.8 kg) and FFM (48.3 ± 10.7 kg) measured by DDT and estimated with the new anthropometric equation (35.4 ± 7.7 kg and 48.1 ± 10.5 kg; respectively) (Table 5).
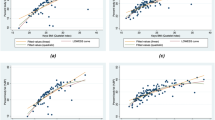
Bland and Altman plots of TBW and FFM prediction equations are shown in Fig. 1. The bias was expressed as the mean of the difference in TBW or FFM measured by DDT using FTIR and estimated from the new anthropometric equation with a confidence interval at 95% equal to [−0.4847; 0.3790] for TBW and [−0.7298; 0.4168] for FFM. For the models’ pure errors, it was 2.0 kg for the TBW prediction equation and 2.7 kg for the FFM prediction equation (Table 4).

(a) TBW and (b) FFM.
The body composition parameters determined by the new anthropometric equations showed a non-significant difference compared to those calculated from DDT for all subjects as well as for men and women (Table 6).
Discussion
The study aimed to develop body composition prediction equations (TBW and FFM) in Tunisian adults using anthropometric parameters and referring to the DDT. The DDT technique is a well-established methodology for the measure of human body composition. It is considered as one of the reference methods for the evaluation of TBW, which is safe, non-invasive, be used directly in the field, and adapted for use in any age group [24,25,26,27]. Therefore, the DDT is considered the gold standard for the validation of other less expensive methods such as the anthropometric method and the BIA [28].
In our knowledge, this study is the first in North Africa which allows the development of anthropometric equations to estimate the body composition measures of TBW and FFM in adults using the DDT. The model developed in the present study is the first specific that validated anthropometric equation for healthy Tunisian adults.
First, we tested the prediction equations available in the literature on our study population by comparing TBW and FFM obtained with those equations against DDT. None of the previously published equations for the prediction of TBW and FFM were valid to use in Tunisian adults except for Slater and Preston equation [13] for the prediction of TBW, and Janmahasation et al. [16] for the prediction of FFM in all population. In fact, the application of Bland and Altman test showed a significant (p < 0.01) proportional bias with DDT among both men and women for the equations of Hume and Weyers [11], Watson et al. [12], Medoua et al. [14] and Chumlea et al. [15]. However, the Bland and Altman approach in the current study revealed high bias values in all subjects (1.27, 1.39, 1.14 and 5.42 kg; (p < 0.01)), especially in women (2.50, 1.67, 5.34 and 5.15 kg; (p < 0.0001)).
Moreover, compared to zero, the differences between the means of measured and predicted values of TBW was significant which indicates the inaccuracy of these equations, which is probably due to the ethnic and racial differences of the studied populations, which largely affect the accuracy of the body composition prediction equation [29].
Although the TBW calculated by the Slater and Preston equation [13] is similar to that found by DDT in the total population, this equation showed a significant absolute bias with the technique of deuterium dilution in men and women. Even if the equation of Slater and Perston [13] showed a similar result as DDT for TBW in the total sample, the equations significantly underestimated TBW (−1.44 ± 3.93 kg) for men and overestimated TBW for women (1.06 ± 4.00 kg). The observed sex differences could be explained by the fact that in the case of Slater and Preston [13], the study was carried out in a large sample with a heterogeneous population (healthy children, HIV-positive children and adults with type 2 diabetes, mild hypertension, pancreatic cancer and lung cancer). Additionally, our population and that of Slater and Preston [13] have a different ethnicity.
The FFM equation calculated by Janmahasation et al. [16], although similar to that found by DDT in the total population and both sexes, the anthropometric equation developed in our study to estimate FFM (R2 = 0.94; RMSE = 2.44) showed better statistical parameters than those obtained by Janmahasation et al. [16] in all subjects using dual energy X-ray absorptiometry as a reference method (R2 = 0.95, RMSE = 2.87 for men and women).
In the present study, the new anthropometric prediction equations for TBW and FFM were developed using gender, age, weight and height as possible predictor variables. The equation which presented the highest adjusted R2 and the lowest RMSE value was selected.
The new equations were applied in the validation group. Good agreement was obtained with the DDT with the lowest pure error value within the limits of 2.03 for the TBW equation and 2.71 for the FFM equation. The new TBW equation predicts effectively TBW in both men and women and provides acceptable absolute bias. Both prediction equations provided excellent agreement with the references measures of TBW (−1.68 to 1.63) and FFM (−0.14 to 0.79) by DDT. The Bland and Altman plot illustrates the good level of concordance between the TBW and FFM predicted using the new equation and TBW (p = 0.97) and FFM (p = 0.58) measured by DDT.
Conclusion
In conclusion, the new anthropometric prediction equations of TBW and FFM developed in this study showed good agreement with the reference technique and were the most accurate to estimate TBW and FFM in Tunisian adults aged between 18–59 years. However, further studies are needed to examine the validity of the new anthropometric equation in the Tunisian elderly.
Limitations of the study
The study has some strength and limitations. The strength of the study was that it was able for the first time to evaluation and validate prediction equations for anthropometric measurements against the criterion methods of DDT in Tunisian elderly. Whilst the limitations are; First, lack of gender balance as men resisted to participate, due to time required to apply the DDT technique. Second, the equations were generated only for healthy adults aged 18–59 years living in urban areas. Thus, it would be interesting to verify the validity of the equation proposed on adults in rural areas by including a population balanced in terms of sex and nutritional status.
Data availability
The dataset supporting the conclusions of this article can be made available upon request from the corresponding author after approval is obtained from the Committee.
References
Abarca-Gomez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017;390:2627–42.
Katsoulis M, Pasea L, Lai AG, Dobson RJ, Denaxas S, Hemingway H, et al. Obesity during the COVID-19 pandemic: both cause of high risk and potential effect of lockdown? A population-based electronic health record study. Public Health. 2021;191:41–7.
Ulijaszek SJ, Kerr DA. Anthropometric measurement error and the assessment of nutritional status. Br J Nutr. 1999;82:165–77.
Flegal KM, Shepherd JA, Looker AC, Graubard BI, Borrud LG, Ogden CL, et al. Comparisons of percentage body fat, body mass index, waist circumference, and waist—stature ratio in adults. Am J Clin Nutr. 2009;89:500–8.
Hunma S, Ramuth H, Miles-Chan JL, Schutz Y, Montani JP, Joonas N, et al. Body composition-derived BMI cut-offs for overweight and obesity in Indians and Creoles of Mauritius: comparison with Caucasians. Int J Obes. 2016;40:1906–14.
Andreoli A, Garaci F, Cafarelli FP, Guglielmi G. Body composition in clinical practice. Eur J Radio. 2016;85:1461–8.
Lopez-Gonzalez D, Wells JCK, Parra-Carriedo A, Bilbao G, Mendez M, Clark P. Body composition assessment in Mexican children and adolescents. Part 1: comparisons between skinfold-thickness, dual x-ray absorptiometry, air-displacement plethysmography, deuterium oxide dilution, and magnetic resonance imaging with the 4-C model. Nutrients. 2022;14:1073.
Bila WC, Mariano RMDS, Silva VR, Dos Santos MESM, Lamounier JA, Ferriolli E, et al. Applications of deuterium oxide in human health. Isotopes Environ Health Stud. 2017;53:327–43.
Peterson MJ, Czerwinski SA, Siervogel RM. Development and validation of skinfold-thickness prediction equations with a 4-compartment model. Am J Clin Nutr. 2003;77:1186–91.
Deurenberg P. The assessment of body composition: uses and misuses. Annual report. Lausanne, Switzerland: Nestle Foundation; 1992. p. 35e72.
Hume R, Weyers E. Relationship between total body water and surface area in normal and obese subjects. J Clin Pathol. 1971;24:234–8.
Watson PE, Watson ID, Batt R. Total body water volumes for adult males and females estimated from simple anthropometric measurements. Am J Clin Nutr. 1980;33:27–39.
Slater C, Preston T. A simple prediction of total body water to aid quality control in isotope dilution studies in subjects 3-87 years of age. Isotopes Environ Health Stud. 2005;41:99–107.
Medoua GN, Essa'a VJ, Tankou CT, Ndzana ACA, Dimodi HT, Ntsama PM. Validity of anthropometry- and impedance-based equations for the prediction of total body water as measured by deuterium dilution in Cameroonian haemodialysis patients. Clin Nutr ESPEN. 2015;10:e167–73.
Chumlea WC, Guo SS, Zeller CM, Reo NV, Baumgartner RN, Garry PJ, et al. Total body water reference values and prediction equations for adults. Kidney Int. 2001;59:2250–8.
Janmahasatian S, Duffull SB, Ash S, Ward LC, Byrne NM, Green B. Quantification of lean bodyweight. Clin Pharmacokinet. 2005;44:1051–65.
Lohman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics; 1988.
World Health Organization (WHO). Obesity and overweight. Fact sheet N°311. 2015.
World Health Organization (WHO). Nuclear technology review 2016. Vienna: International Atomic Energy Agency; 2016.
El Kouki D, El Kari K, Ben Jemaa H, Draoui J, Oueslati S, Chichi S, et al. Relevance of body mass index and bioelectrical impedance analysis vs. deuterium dilution technique to assess excess of fat among young adults. Isotopes Environ Health Stud. 2021;57:193–203.
IAEA, International Atomic Energy Agency. Introduction to body composition assessment using the deuterium dilution technique with analysis of saliva Q5 samples by Fourier transform infrared spectrometry. IAEA Hum Heal Ser; No 12. 2010.
Wang Z, Deurenberg P, Wang W, Pietrobelli A, Baumgartner RN, Heymsfield SB. Hydration of fat-free body mass: review and critique of a classic. Am J Clin Nutr. 1999;69:833–41.
Bland JM, Altman DG. Applying the right statistics: analyses of measurements studies. Ultrasound Obstet Gynecol. 2003;22:85–93.
Koletzko B, Demmelmair H, Hartl W, Kindermann A, Koletzko S, Sauerwald T, et al. The use of stable isotope techniques for nutritional and metabolic research in paediatrics. Early Hum Dev. 1998;53:S77–97.
International Atomic Energy Agency. Introduction à l’évaluation de la composition corporelle par dilution de deutérium grâce à l’analyse d’échantillons de salive par spectroscopie infrarouge à transformée de Fourier. 2013.
Ben Jemaa H, Mankaï A, Khlifi S, Minaoui R, Ghozzi D, Zediri M, et al. Development and validation of impedance-based equations for the prediction of total body water and fat-free mass in children aged 8-11 years. Clin Nutr. 2019;38:227–33.
Salas JDZ, Laclé-Murray A. Predictive validity of body fat percentage by bioimpedance compared with deuterium oxide dilution in Costa Rican schoolchildren. Am J Hum Biol. 2017;29:e23028.
Resende CMM, Camelo Júnior JS, Vieira MNCM, Ferriolli E, Pfrimer K, et al. Body composition measures of obese adolescents by the deuterium oxide dilution method and by bioelectrical impedance. Braz J Med Biol Res. 2011;44:1164–70.
Wagner DR, Heyward VH. Measures of body composition in blacks and whites: a comparative review. Am J Clin Nutr. 2000;71:1392–402.
Acknowledgements
This study was performed with the support of the International Atomic Energy Agency. We thank all the participants in the present study.
Author information
Authors and Affiliations
Contributions
The authors made the following contribution to the manuscript: DK participated in all stages of the study. KK participated in the statistical analysis of the paper. DK, JD and HBJ participated in the data collection. AA, HA and AM revised the article. HBJ, NBA, AA, HA and AM directed the collection of data. AM contributed in the writing up. AmM contributed to the language correction. DK designed and conducted the research and had the primary responsibility for the assessment of body composition by the method of dilution of deuterium oxide and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol was approved by the Scientific Research and Ethical Committee of the National Institute of Nutrition and Food Technology. The procedures followed were in accordance with the ethics standards of the responsible committee on human experimentation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
El Kouki, D., El Kari, K., Draoui, J. et al. Development and validation of anthropometric predictive equations that estimate the total body water and fat-free mass in Tunisian adults. Eur J Clin Nutr 77, 447–453 (2023). https://doi.org/10.1038/s41430-023-01262-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-023-01262-2
