
Abstract
This study reports the Hb, erythropoietin (Epo), and reticulocyte course at different postnatal ages (range, 8-83 d) of 56 blood samples from 30 newborns(range, one or two blood samples from each newborn) with erythroblastosis fetalis (18 intrauterine transfused (IUTd) and 12 non-IUTd). Hb, Epo, and reticulocyte values were not statistically different in IUTd and non-IUTd cases. As age increased, decreasing Hb values and increasing Epo levels were observed. The reticulocyte count was relatively low in all but six cases. There was an inverse correlation between Epo and Hb (r = -55,p < 0.001), but no correlation was found between Hb and reticulocytes or between Epo and reticulocytes. When groups were formed on the basis of Hb levels, anemic newborns showed higher serum Epo than did nonanemic patients (p < 0.02). In the present study we found a significant increase in Epo levels in anemic newborns without a rise in the reticulocyte count. These results suggest that other mechanisms, rather than low Epo production, could be involved in the pathogenesis of this anemia. Persisting anti-D antibodies, probably at a medullary level, may destroy erythrocyte precursors, leading to anemia with a low reticulocyte count.
Similar content being viewed by others


Main
Immunoprophylaxis with anti-D antibody has greatly reduced the incidence of erythroblastosis fetalis. Unfortunately, silent immunization can occur, often leading to fetal anemia and/or hydrops in need of intrauterine transfusion. The majority of newborns with Rh hemolytic disease develop, beginning from 2 wk of age, a late anemia with a low reticulocyte count. The pathogenesis of this anemia is still obscure. Thorp et al.(1) postulated that there were three mechanisms involved: anti-D destruction of bone marrow precursors, anti-D destruction of reticulocytes in the peripheral circulation, and an inappropriately low Epo production.
The aim of this study was to measure Epo, Hb, and reticulocyte levels in newborns and infants with erythroblastosis fetalis transfused and not transfused in utero, and to define a possible relationship between these parameters.
METHODS
Subjects. Of 30 newborns with Rh hemolytic disease, 18 were IUTd by simple intravascular transfusions with Rh-negative, cytomegalovirus-negative, irradiated packed red blood cells, whereas 12 were not. Fetal and neonatal data are reported in Table 1.
Measurements. Immunoreactive Epo concentrations in sera were estimated by RIA from Bio-Merieux (France, 1990) with a detection limit of 1 U/L.
Hb concentrations were measured spectrophotometrically after oxidation to methemoglobin by treatment with potassium ferricyanide; a reticulocyte count was performed by a cytofluorimeter R3000 (TOA-SYSMEZ).
Protocol. Fifty-six blood samples were collected from 30 newborns (range, one or two samples from each newborn) with Rh hemolytic disease (anti-D immunization) to evaluate Epo levels. Reticulocyte and Hb levels were measured at the same time. Blood samples were obtained during the nursery stay, beginning at 8 d of life, and/or when infants were readmitted to the hospital for anemia (age 21-83 d, Hb (±SD): 6.8 (±0.8) g/dL). Informed parental consent was obtained in all cases.
Data analysis. The Epo, Hb, and reticulocytes values were plotted over postnatal age; a computed least-squares fit curve was traced when the r2 value was significantly high. Then groups were formed on the basis of fetal therapy (IUTd or non-IUTd newborns) and Hb levels(anemic or nonanemic patients). Infants were defined as anemic when Hb levels were lower than the reported value for age according to Lubin(2). Groups were compared with two-way ANOVA. Age was used as a covariate in the analysis. Epo values were transformed in their natural logarithmic equivalents to reduce skewness before ANOVA was performed. The SPSS V4.01 (SPSS Inc., Chicago, IL) statistical package was used in the analysis.
RESULTS
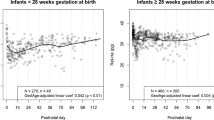
There were no differences in Epo, Hb, and reticulocyte levels in IUTd or non-IUTd newborns. Data were thus pooled. There was an inverse correlation between Epo and Hb (r = -0.55, p < 0.001). There was no correlation between reticulocyte count and Hb values or between reticulocyte count and Epo levels. Figure 1 shows the Hb, Epo, and reticulocyte course for different postnatal ages. The curve represented inFigure 1A is a computed best fit and represents a logarithmic curve which describes the least-squares fit of the relation of Hb concentration and postnatal age. The curve represented inFigure 1B is the least-squares fit of the relation between Epo concentrations and postnatal age. As shown inFigure 1C, the reticulocyte count was relatively low(below 30‰) in all but six cases. The relationship between the infant's Hb concentration and plasma Epo is shown in Figure 2; the traced curve is a computed best-fit exponential curve.

Relation of Hb concentration (g/dL) (A), erythropoietin levels (U/L) (B), reticulocyte count (‰)(C), and postnatal age for 56 samples from 30 infants with erythroblastosis fetalis (18 IUTd and 12 not IUTd).

Relation of serum erythropoietin (U/L) and Hb concentration (g/dL) for 56 samples from 30 infants (age 8-83 d) with erythroblastosis fetalis (18 IUTd and 12 not IUTd).
Moreover, when groups were formed on the basis of Hb levels (anemic or nonanemic infants), Epo concentrations were significantly different in anemic and nonanemic patients (two-way ANOVA the main effects, p < 0.02 for serum Epo) but not in IUTd and non-IUTd newborns (p > 0.05)(Table 2). There was no significant interaction between fetal therapy and anemia (p > 0.05).
Anemic and nonanemic patients showed no significant differences in reticulocyte count. There was no difference in Hb and Epo levels in cases with or without reticulocytosis.
Moreover, a correlation was found between maternal anti-D titer at the last IUT and number of simple transfusions required after birth (r = 0.6,p = 0.011); the correlation was stronger when simple and exchange transfusions were considered together (r = 0.8, p = 0.000).
DISCUSSION
This study analyzes Epo, Hb, and reticulocyte levels in newborns with erythroblastosis fetalis IUTd and no IUTd, beginning at 8 d of life. Data were not statistically different in IUTd and non-IUTd patients. IUTd newborns did not show any difference in the rate and time of anemization with respect to non-IUTd newborns. Moreover, Epo concentration, an index of erythropoietic activity, was increased in both IUTd and non-IUTd newborns during anemia, suggesting an incomplete suppression of fetal erythropoiesis by IUT. Instead, the reticulocyte count was low in both groups. Those data did not confirm those reported by Koenig et al.(3) and Thorpet al.(1). These authors(1, 3) suggested the role of an inappropriate Epo production in the pathogenesis of anemia in erythroblastosis fetalis. Koeniget al.(3) reported an Epo concentration of 33 U/L in one newborn with anemia (defined as hyporegenerative on the basis of low reticulocytosis). Thorp et al.(1) found in one newborn, with anemia and erythroblastosis fetalis, an Epo concentration of 5 U/L. The marrow aspirate showed 16% normoblasts. This percentage was low if compared with normoblasts from adult marrow (19-37%), but in the normal range if compared with normoblasts from marrow of healthy 4-wk-old infants(3-20%).
In the present study we found a logarithmic decrease of Hb concentration beginning at 8 d of life. An inverse correlation was found between Epo and Hb, but no correlation was found between Hb and reticulocyte count. The Epo levels in anemic patients were 5-9-fold higher than those of nonanemic newborns, even though we could not find a corresponding increase in reticulocyte count. Epo values were also significantly higher than those in normal newborns comparable for age, as reported in our previous study(4). As shown in Figure 2, increased Epo levels were found especially when the Hb concentration fell below 8.5 g/dL. Moreover, the range of Epo levels in anemic patients was very wide. Other authors(5, 6) have reported in chronic anemia of nonrenal origin, especially in adults, an inverse exponential correlation between hematocrit and Epo levels with some 100-fold increase in the more severe forms but with wide interindividual variation. The variation appeared to be very high with up to 10-fold differences in patients with the same hematocrit. An exact quantification of the adequate increase in Epo concentration with decreasing red blood cell mass has not so far been achieved. Probably the time lapse between the beginning of anemia and the measurement of Epo concentration could influence the values. On the basis of the data reported in the present study we may hypothesize that the anemia of erythroblastosis fetalis, even after IUT and even when the reticulocyte count is low, is not simply“hyporegenerative.” It is possible, as stated by Hyman and Sturgeon(7), that a relative hypoplasia may occur as cell destruction exceeds cell production. Burk et al.(8) in 1987 described an IUTd newborn with erythroblastosis fetalis, severe anemia, and low reticulocyte count at 7 wk after birth. The bone marrow aspirate revealed many normoblasts but no reticulocytes, and the bone marrow erythrocyte precursor cells contained anti-D antibodies. The authors concluded that the antibodies were enough to support a hemolytic process but also that they affected bone marrow precursors, leading to an apparent failure of reticulocytosis. In our study there was no rise in the reticulocyte count during anemia; nevertheless, there was an increase in Epo levels. So the low degree of reticulocytosis could not be explained on the basis of a low Epo production. It is possible that circulating D antibodies or D antibodies present in the bone marrow could affect erythroid precursors as soon as they show their Rhesus group on the membrane, leading to apparent hyporegeneration, in accordance with the findings of Burk et al.(8). In the present study we found, in the IUTd group, a direct relationship between maternal anti-D titer at the time of the last IUT and the number of blood transfusions required postnatally. The higher anti-D titer could explain the higher degree of red blood cells and reticulocyte destruction. Fahnenstich et al.(9) reported in a group of 19 newborns with erythroblastosis fetalis a slow decrease of D antibodies for a period of time; the titer disappeared quickly beginning with the 6th wk, even though neonates who had an exchange transfusion showed an earlier low anti-D concentration.
The study of anti-D titer and, whenever possible, a marrow aspirate as well as the measurement of Epo, Hb, and reticulocyte levels could help to clarify the pathogenesis of late anemia with erythroblastosis fetalis.
Abbreviations
- Epo:
-
erythropoietin
- IUT:
-
intrauterine transfusion
- IUTd:
-
intrauterine transfused
- ANOVA:
-
analysis of variance
References
Thorp JA, O'Connor T, Callenbach J, Cohen GR, Yeast JD, Albin J, Plapp F 1991 Hyporegenerative anemia associated with intrauterine transfusion in rhesus hemolytic disease. Am J Obstet Gynecol 165: 79–81
Lubin BH 1992 Reference values in infancy and childhood. In: Nathan DG, Oski FA (eds) Hematology of Infancy and Childhood. WB Saunders, Philadelphia, pp 1552–1574
Koenig JM, Ashton RD, GR De Vore, RD Christensen 1989 Clinical and laboratory observations: late hyporegenerative anemia in Rh hemolytic disease. J Pediatr 115: 315–318
Dallacasa P, Ancora G, Miniero R, Salvioli GP 1994 Erythropoietin (Epo) levels in healthy and unhealthy newborns. Proceedings of the 14th European Congress of Perinatal Medicine, Helsinki, No. 54(abstr)
Erslev AJ, Wilson J, Caro J 1987 Erythropoietin titers in anemic, nonuremic patients. J Lab Clin Med 109: 429–433
Rege AB, Brookins J, Fisher JW 1982 A radioimmunoassay for erythropoietin: serum levels in normal human subjects and patients with hemopoietic disorders. J Lab Clin Med 100: 829–843
Hyman CB, Sturgeon P 1955 Observations on the convalescent phase of erythroblastosis fetalis. Pediatrics 16: 15–23
Burk CD, Malatack JJ, Ramsey G 1987 Misleading Rh phenotype and severe prolonged anemia in hemolytic disease of the newborn. Am J Dis Child 141: 712–713
Fahnenstich H, Dame C, Hoch J, Giers G 1994 Anti-D-antibodies in Rhesus hemolytic disease in the first trimester: implications for a treatment with r-hu-Epo. Proceedings of the 14th European Congress of Perinatal Medicine, Helsinki, No. 38(abstr)
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dallacasa, P., Ancora, G., Miniero, R. et al. Erythropoietin Course in Newborns with Rh Hemolytic Disease Transfused and Not Transfused in Utero. Pediatr Res 40, 357–360 (1996). https://doi.org/10.1203/00006450-199608000-00027
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199608000-00027
