
Abstract
Purpose
To present an alternative cataract surgical technique in patients with cataract and intravitreal hemorrhage.
Methods
Twelve cases with poor fundus reflex caused by severe vitreus hemorrhage were included in the study. All patients underwent combined phaco surgery and 23-gauge vitrectomy. Chandelier retroillumination was inserted into the infusion trochar during the cataract operations and was used with low power (50–75%) in necessary steps.
Results
We did not experience phaco complications or complications due to technique during surgery. Retroillumination assistance was especially useful during final stages of cataract surgery, particularly irrigation-aspiration of cortical material.
Conclusion
Retroillumination in absence of red fundus reflex may be helpful and can be practiced more often in cataract surgery combined with vitrectomy.
Similar content being viewed by others


Introduction
Combined 23-G vitrectomy and phacoemulsification has been more frequently performed recently and appears effective with an acceptable safety profile for patients with cataract and simultaneous retinal diseases.1, 2, 3, 4 Nonethless, there is no fixed procedure for this surgical method. Although combined surgery seems effective and safe, it can be challenging because of insufficient red reflex caused by severe vitreous hemorrhage.5, 6
We aimed to report our experience on retroillumination using 23G chandelier during the cataract surgery combined with vitrectomy in eyes with poor red reflex.
Materials and methods
Twelve cases with poor fundus reflex caused by severe diabetic vitreus hemorrhage were included in the study. The patients had nuclear cataract (NOII-III, Lens Opacities Classification System (LOCS) III)7 with minimal cortical and posterior capsular components. None of the patients had white cataract or posterior polar cataract.
All operations were performed by same surgeon (OK). Alcon Infinity phacoemulsification machine (Fort Worth, TX, USA) and Alcon Constellation vitrectomy machine (Alcon Laboratories, Inc, Fort Worth, TX, USA) were used for all operations. First single-step 23G infusion trochar was placed sclerotomy, 3.5 mm from the corneal limbusin the inferotemporal area (23G Total plus Vitrectomy Pack, for Alcon Constellation-Alcon Laboratories, Inc). Chandelier probe (25G for Alcon Constellation-Alcon Laboratories, Inc) was introduced into the trochar which was later used for infusion during vitrectomy. Also to make the probe more stable, fiberoptic cable was taped to the drape. Chandelier illumination with low power (50–75%) was used in necessary steps of phaco surgery.
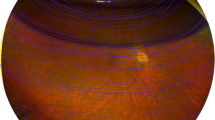
Cataract surgery was initiated with microscope lights on and endoillumination off. Clear corneal phaco incisions (2.2 mm) were placed usually to the oblique quadrants superotemporally or superonasally by the surgeon’s preferance. Sodium hyaluronate and chondroidin sulfate (DuoVisc; Alcon Laboratories, Inc) was used during the operation as viscoelastic material. After staining the anterior capsule with trypan blue, continuous circular capsulorhexis was performed using microscope lights without retroillumination. Then, phacoemulsification was performed using retroillumination with and without microscope illumination interchangibly (Figure 1a and b). Preferred phaco technique was stop and chop method.

(a) Phacoemulsification with retroillumination and microscope lights—on. (b) Phacoemulsification with microscope lights off/only retroillumination. (c) I/A and posterior capsule polishing under retroillumination.
After phacoemulsification was completed, retroillumination was used during epinucleus removal, I/A of cortical material and posterior capsule polishing (Figure 1c). Foldable intraocular lens (Acrysof material, Alcon Laboratories, Inc) was also implanted under chandelier retroillumination. The phaco incisions were not sutured before vitrectomy but viscoelastic material was not removed at the end of cataract surgery. In the pars plana vitrectomy phase, first-infusion line was placed inferotemporally instead of illumination and three port 23G pars plana vitrectomy was performed in usual manner. Core vitrectomy was performed 5000 cuts/min- 300 mm Hg vacuum, was followed by seperating posterior hyaloid if not already detached. Membranes and peripheral vitreus was removed in shave mode. Some cases required additional laser photocoagulation to the periphery where chandelier light and indentation might be used.
Results
The mean age of the patients (7 male and 5 female) was 62.4 years (range 55–74) and the mean follow-up time was 7.8 months (range 4–14 months). The mean preoperative visual acuity was 1.7±0.4 logMAR, whereas it was 0.4±0.1 logMAR at the last visit. The difference between preoperative and postoperative visual acuity was statistically significant (P<0.001; paired t-test). The mean preoperative intraocular pressure (IOP) was 19.5±3.8 mm Hg and the mean postoperative IOP at final visit, 18.1±2.4 mm Hg (P=0.357; paired t-test). There was no patients with uncontrolled IOP following operations.
We used endoillumination with and without microscope illumination interchangeably during the phaco surgery. Endoillumination assistance was especially useful during final stages of surgery. Irrigation-aspiration of cortical material was also made easier with the help of endoillumination. Furthermore, no complication related to retina, capsulorhexis, phacoemulsification and I/A was observed. The same chandelier illumination placed in one of the trochars was also helpful in peripheral indentation and laser in those patients who required enough laser treatment- judged during the operation by the surgeon some cases. We did not use endotamponade but left partial air in some cases to prevent early hypotony.
Discussion
Many studies over the years showed that compared with external microscope illumination, better resolution and contrast could be achieved by endoillumination for cataract surgery.5, 6, 8, 9, 10
The endoilluminator-assisted technique was first used for capsulorhexis in a patient with intumescent cataract.11 Yamamoto et al described the trypan blue and endoilumination-assisted phacoemulsification technique in eyes with vitreous hemorrhage. In this two step surgery, after staining the lens capsule with trypan blue, circular capsulorhexis was performed. Subsequently phacoemulsification was done using a conventional endoilluminator.12
Also, Kim et al used surgeon-controlled-endoillumination (intravitreal) technique for I/A, and they reported that although this techique was effective, lens epithelial cells and particles from the posterior capsule were not removed completely. In this technique, inserting and moving an endoilluminator of 4 mm length into the vitreous cavity could increase the risk of a retinal tear of sclerotomy site or posterior capsule tear but no complication was observed.13
In the current study, no complications were observed. Chandelier light tip movement in an 'un-vitrectomised' eye could be dangerous and lead to retinal breaks as well as lenticular damage. Therefore, fiberoptic cable was taped to the drape so the chandelier light tip did not move during the surgery. We later on proceeded with vitrectomy procedure, during which we did not encounter any retinal damage due to chandelier light probe. Also prepratory insertion of infusion trochar before the phaco surgery is a common method we apply in our combined procedures. Additional insertion of chandelier light probe and fixing it to drape was not considered to be risky for the patient.
During pars plana vitrectomy, the use of endoillumination has phototoxic effects on the retina especially for macular surgery.14, 15 However, we believe that risk of phototoxic effect is low in our cases because less light can reach retina due to vitreous hemorrhage. Furthermore, no complication had been reported in the previous studies associated with endoillumination assisted cataract surgery.5, 8, 13
Jang et al used illuminated infusion chandelier in many surgical steps including capsulorhexis without trypan blue, phacoemulsification, polishing and no complication was observed in their study consisting of six patients with cataracts and vitreous hemorrhage.5 Authors concluded that patients with vitreous hemorrhage and absent red reflex may benefit from chandelier retroillumination—assisted cataract surgery.5
In the current study consisting of 12 patients, capsulorhexis was performed with trypan blue under coaxial microscope illumination, retroillumination was not used in this step because sufficient visibility could not be achived through retroillumination alone due to density of cataract and vitreous hemorrhage. Therefore during phacoemulsification, chandelier retroillumination was used with and without external microscope illumination interchangeably, but retroillumination alone was enough for I/A.
Compared with conventional light pipe—style endoilluminator, the 23G illuminated infusion chandelier does not need to be held and thus provides a hands-free view. Therefore surgeon can use both hands to perform cataract operation. Moreover using chandelier retroillumination is not extra work because sclerotomy is one of the essential step for vitrectomy. In conclusion, chandelier illumination may be used for patient with vitreous hemorrhage and poor red reflex, and can be practiced more often in phacoemulsification surgery combined with vitrectomy.

References
Moon H, Sohn HJ, Lee DY, Lee JY, Nam DH . Combined 23-gauge sutureless vitrectomy and clear corneal phacoemulsification for rhegmatogenous retinal detachment repair. Int J Ophthalmol 2015; 8: 122–127.
Lee DY, Jeong HS, Sohn HJ, Nam DH . Combined 23-gauge sutureless vitrectomy and clear corneal phacoemulsification in patients with proliferative diabetic retinopathy. Retina 2011; 31: 1753–1758.
Lee JY, Jeong HS, Lee DY, Sohn HJ, Nam DH . Early postoperative intraocular pressure stability after combined 23-gauge sutureless vitrectomy and cataract surgery in patients with proliferative diabetic retinopathy. Retina 2012; 32: 1767–1774.
Hütz WW, Hoffmann P, Hengerer F . Fifty consecutive cases of transconjunctival sutureless 23-gauge vitrectomy combined with phacoemulsification and IOL implantation. Ophthalmic Surg Lasers Imaging 2011; 42: 481–486.
Jang SY, Choi KS, Lee SJ . Chandelier retroillumination-assisted cataract extraction in eyes with vitreous hemorrhage. Arch Ophthalmol 2010; 128: 911–914.
Lee VY, Kwok AK . Multiport-illumination-system-assisted phacoemulsification in eyes with dense vitreous hemorrhage during combined cataract and vitreous surgery. J Cataract Refract Surg 2003; 29: 1252–1255.
Chylack LT Jr, Wolfe JK, Singer DM, Leske MC, Bullimore MA, Bailey IL et al. The lens opacities classification system III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol 1993; 111: 831–836.
Jung Y, Kim IN, Yoon J, Lee JY, Kim KH, Lee DY et al. Intracameral illuminator-assisted advanced cataract surgery combined with 23-gauge vitrectomy in eyes with poor red reflex. J Cataract Refract Surg 2013; 39: 845–850.
Oshima Y, Shima C, Maeda N, Tano Y . Chandelier retroillumination-assisted torsional oscillation for cataract surgery in patients with severe corneal opacity. J Cataract Refract Surg 2007; 33: 2018–2022.
Saragas S, Krah D, Miller D . Improved visualization through cataracts using intravitreal illumination. Ann Ophthalmol 1984; 16: 311–313.
Bhattacharjee K, Bhattacharjee H, Goswami BJ, Sarma P . Capsulorhexis in intumescent cataract. J Cataract Refract Surg 1999; 25: 1045–1047.
Yamamoto N, Ozaki N, Murakami K . Trypan-blue-andendoillumination-assisted phacoemulsification in eyes with vitreous hemorrhage during combined cataract and vitreous surgery. Ophthalmologica 2005; 219: 338–344.
Kim KH, Sohn HJ, Song HJ, Lee DY, Nam H . Surgeon-controlled-endoillumination-guided irrigation and aspiration during combined 23-gauge sutureless vitrectomy and cataract surgery in eyes with poor fundus reflex. J Cataract Refract Surg 2010; 36: 2028–2031.
Yanagi Y, Iriyama A, Jang WD, Kadonosono K . Evaluation of the safety of xenon/bandpass light in vitrectomy using the A2E-laden RPE model. Graefes Arch Clin Exp Ophthalmol 2007; 245: 677–681.
Kuhn F, Morris R, Massey M . Photic retinal injury from endoillumination during vitrectomy. Am J Ophthalmol 1991; 111: 42–46.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Bilgin, S., Kayikcioglu, O. Chandelier retroillumination-assisted cataract surgery during vitrectomy. Eye 30, 1123–1125 (2016). https://doi.org/10.1038/eye.2016.112
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2016.112
