
Abstract
Purpose
To study the ultrastructure of the medial rectus in patients with intermittent exotropia at different ages.
Patients and methods
The medial recti were harvested surgically from 20 patients with intermittent exotropia. Patients were divided into adolescent (age<18 years, n=10) and adult groups (age >18 years, n=10). The normal control group included five patients without strabismus and undergoing eye enucleation. Hematoxylin and eosin staining and transmission electron microscopy were used to visualize the medial recti. Western blot was used to determine the levels of myosin and actin.
Results
Varying fiber thickness, atrophy, and misalignment of the medial recti were visualized under optical microscope in patients with exotropia. Electron microscopy revealed sarcomere destruction, myofilament disintegration, unclear dark and light bands, collagen proliferation, and fibrosis. The adolescent group manifested significantly higher levels of myosin and actin than the adult group (P<0.05).
Conclusion
Younger patients with intermittent exotropia show stronger contraction of the medial recti compared with older patients. Our findings suggest that childhood was the appropriate time for surgery as the benefit of the intervention was better than in adulthood.
Similar content being viewed by others

Introduction
Patients with strabismus have abnormally aligned eyes, with one eye looking straight ahead, and the other eye turned inwards, outwards, up or down. Most cases of childhood onset strabismus are present constantly, but some types are intermittent, which is only present sometimes.1, 2 In patients with intermittent exotropia (X(T)), an eye intermittently turns outwards (exotropia), especially when looking into the distance, when tired or daydreaming. Intermittent exotropia is usually treated surgically, by rectifying the muscles around the eye. The pathological mechanisms of intermittent exotropia are complex and are associated with imbalance between convergence and divergence3 as well as genetic and anatomical factors. However, degeneration and fibrosis of the extraocular muscles have been observed with light microscopy and electron microscopy. These changes decrease the muscular elasticity and tone, and possibly contribute significantly to exotropia. In addition, it has been shown that altered cellular structure of the extraocular muscles affects the degree of exotropia and surgical outcomes.4
Extraocular muscle proprioceptors and proprioception have crucial roles in the control of eye position.5, 6 Previously, it was thought that the extraocular muscles and nerves in patients with strabismus were not pathologically altered.7 However, it has now become clear that a few patients with strabismus showed abnormal histology of the extraocular muscles.8 This study sought to compare the ultrastructure of the medial recti between patients with and without intermittent exotropia. The myosin and actin protein levels were also examined and compared.
Materials and methods
Patients
Twenty patients with the basic type of intermittent exotropia underwent surgery on their extraocular muscles at our hospital between May 2014 and August 2014. All patients underwent a unilateral lateral rectus recession of 7 mm and a medial rectus resection of 4 mm. The patients were divided into adolescent (age range 3–17 years, n=10) and adult groups (age range 18–38 years, n=10). Three- to 7-mm long medial rectus muscles were harvested and attached to the sclera measuring 4–5 cubic millimeter. Patients who received eye enucleation for severe ocular trauma served as normal controls. These patients had no history of strabismus or other ocular diseases. The control group included two patients aged below 18 years (10 and 15 years, respectively) and three patients aged over 18 years (27, 32, and 35 years, respectively). The clinical data of the patients are listed in Table 1.
Hematoxylin and eosin staining
Half of each medial rectus specimen was fixed in 10% formaldehyde and dehydrated. One-fourth of each medial rectus specimen was used for transmission electron microscopy. Another one-fourth was flash frozen in liquid nitrogen and stored at −80 °C for western blotting analysis. Hematoxylin and eosin (HE) staining was performed on paraffin-embedded, longitudinal sections of 4-μm thick samples. The HE-stained sections were visualized under a microscope (IX31, Olympus, Tokyo, Japan).
Transmission electron microscopy
One-cubic millimeter block of tissue was fixed in 2.5% glutaraldehyde solution at 4 °C for 2 h. Sections of 50–70 nm thickness were prepared and observed with a transmission electron microscope (120 KV, HT7700, HITACHI, Tokyo, Japan).
Western blot
In brief, the samples were lysed using lysis buffer (20 mM Tris/HCl, pH 7.5, 137 mM NaCl, 1% (v/v) Triton X-100, protease inhibitor cocktail (Complete, EDTA-free; Roche Applied Science, Indianapolis, IN, USA) and phosphatase inhibitor cocktail (PhosStop, Roche Applied Science)) and sonicated on ice. Bradford protein assay was used to determine protein concentration of lysates (Bio-Rad, Hercules, CA, USA). Lysates were heated at 70 °C with LDS (lithium dodecyl sulfate) sample buffer (Invitrogen, Carlsbad, CA, USA) and DTT (dithiothreitol; Sigma-Aldrich, St Louis, MO, USA) for 10 min. Protein samples (40 μg, unless otherwise stated) were then separated on 10% SDS-PAGE and transferred for 2 h to PVDF membranes at 80 V. The membrane was blocked with 5% (w/v) non-fat dried skimmed milk powder in 0.1% Tris-buffered saline with 0.1% (v/v) Tween-20 for 1 h at room temperature. Membranes were then incubated overnight at 4 °C with either of the following primary antibodies (diluted in blocking solution): rabbit anti-human monoclonal myosin (1:1500, Cat. No. 14-6503; Biorbyt, San Francisco, CA, USA); or rabbit anti-human monoclonal actin (1:2500, Cat. No. orb10068; Biorbyt). The immunolabeled samples were incubated with mouse anti-human monoclonal GAPDH (1:200 diluted in blocking solution, Cat. No. sc-25778; Santa Cruz, CA, USA), used to indicate protein-loading, for 1 h, followed by treatment with enhanced chemiluminescence (ECL) solution for 2 min at room temperature. The blots were developed using ECL for 5 min and analyzed with ImageJ software.9 The relative expression levels of myosin and actin were normalized to that of GAPDH.
Statistical analysis
Data were presented as mean±SD and compared using one-way ANOVA. Statistical analyses were performed using SPSS 13.0 software (SPSS, Chicago, IL, USA). P<0.05 was considered statistically significant.
Statement of ethics
This study was approved by our Institutional Review Board. Informed consent was obtained from the patients or their parents. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
Results
Light microscopy
The muscle fibers of the medial recti in the normal controls were closely aligned in one direction with very little extracellular matrix. However, in patients with intermittent exotropia the medial recti showed pathological changes including varying fiber thickness, atrophy, abnormal alignment, internalized nuclei, excessive extracellular matrix, and even degenerated muscle fibers in a few patients. The pathological changes worsened with age and chronic strabismus (Figure 1).

Hematoxylin and eosin staining of the medial recti. (a) The normal controls showed tight alignment in one direction with minimal extracellular matrix. (b) The adolescent group showed differential thickness of the muscle fibers and mildly abnormal alignment. (c) The adult group showed muscular atrophy, fibrosis, and degeneration.
Ultrastructure of the medial recti
The medial recti of the normal controls showed intact cell membrane, tightly aligned myofibrils, well-aligned sarcomeres, clear dark and light bands, Z line, H band, evenly distributed mitochondria, and glycogen. Conversely, patients with intermittent exotropia had medial recti with degenerated sarcomeres and myofilaments along with unclear, dark and light bands. Fibroblasts exhibited collagen proliferation and fibrosis. The mitochondria showed pyknosis. The adolescent group with intermittent exotropia showed milder fibrosis of the medial recti compared with the adult group (Figure 2).

Transmission electron microscopy of the medial recti. (a) Normal controls showed clear dark and light bands and Z line. (b) The adolescent group showed fuzzy sarcomeres, merged myofilaments, and collagen fibrous proliferation. (c) The adult group showed myofilament discontinuity, mitochondria pyknosis, and collagen fibrosis. M, mitochondria.
Myosin and actin
The adolescent group with intermittent exotropia showed significantly higher levels of myosin and actin in the medial recti than the adult group (P<0.05). The adult group had significantly lower levels of myosin and actin in the medial recti than the normal controls (P<0.01). However, no significant differences were seen between the adolescent patients with intermittent exotropia and normal controls (Figure 3).

Western blots of myosin and actin. The adolescent group with intermittent exotropia showed significantly higher levels of myosin and actin in the medial recti than the adult group (*P<0.05). The adult patients had significantly lower levels of myosin and actin in the medial recti than the normal controls (**P<0.01).
Discussion
Our study found pathological alterations at the cellular and subcellular levels in the medial recti of patients with intermittent exotropia. In addition, adolescent patients manifested significantly higher levels of myosin and actin in the medial recti than the adult patients.
The striated extraocular muscles consist of thousands of muscle fibers, each containing thousands of myofibrils and myotubules. The myofibrils are composed of thick and thin myofilaments.10, 11 The extraocular muscles of patients in the normal control group in this study contain uniform and well-aligned muscle fibers without any collagen proliferation. Under transmission electron microscopy, the muscle fibers display intact sarcomeres, clear M and Z lines, and evenly distributed mitochondria. At the junction of the tendons, rich nerve endings and proprioceptors are seen. No significant changes were seen in the muscle fiber morphology among different age groups. Further, the muscle fiber width has a possible role in the development of intermittent exotropia, with variable fiber thickness associated with intermittent exotropia. However, it was difficult to measure muscle fiber width in the intermittent exotropia group for comparison with age-matched controls in our study. We focused on the ultramicroscopic structure of the extraocular muscles in intermittent exotropia, instead. It is important to combine the ultramicroscopic data with muscle fiber width in a future investigation.
Myosin and actin are contraction proteins found in myofibrils. Myosin is the primary component of the thick myofilaments. The myosin ATPase catalyzes the release of ATP, the chemical energy. In addition, myosin generates power stroke in skeletal muscle by releasing the phosphate after ATP hydrolysis while myosin is tightly bound to actin. Actin is relatively simple in its structure and binds with myosin.12 Movement of the extraocular muscles is achieved through myocyte contraction. At the molecular level, the myocyte contraction is mediated by contractile proteins, primarily actin and myosin. In the 1950s, the sliding between the thick and thin myofilaments in the sarcomeres was proposed to explain the muscle contraction. Initiation of the sliding is directly related to the molecular structure and properties of the myofilament proteins. Our results showed that in adolescents with intermittent exotropia, significantly higher levels of myosin and actin in the medial recti contribute to stronger contraction compared with the adult group of patients. These results suggest that the medial recti of adolescents manifest stronger contraction than in the adult group.
Our study also confirmed previous studies reporting pathological ultrastructural changes in the weak extraocular muscles of patients with strabismus.8 Patients with ocular motility disorders manifest pathological changes in their extraocular muscles including atrophy, decreased volume and number of the muscle fiber, abnormal alignment, and collagen proliferation.13, 14, 15 Ultrastructural changes observed under transmission electron microscopy include sarcomere destruction, unclear M and Z lines, abnormal accumulation of mitochondria and other particles in the cytoplasm, vacuolar degeneration, and diminished neural components. Patients with strabismus show atrophy of the extraocular muscles, leading to impaired eye positioning and binocular vision16, 17, 18 we speculate that these pathological changes are associated with chronic strabismus. In patients with intermittent exotropia, the medial rectus is not excited for prolonged period. The antagonistic, congenerous, and yoke muscles may also show pathological changes over time. Consistently, patients with chronic strabismus often have more severe symptoms, such as increased strabismus angle, visual defects, eye movement dysfunction, and eye strain.
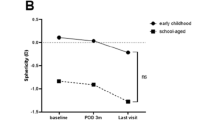
As the preoperative stereopsis was significantly different, it may be prudent to consider the differences between the two groups and their influence on the outcome. It is well known that the presence of preoperative stereopsis is predictive of better postoperative outcomes. Persistent and chronic intermittent exotropia leads to loss in binocular vision, was and is associated with a significantly higher level of preoperative stereopsis in the younger age group. In addition, based on the clinical results and ultrastructural data of our study, we hypothesized that the adolescent group with intermittent exotropia manifested a unique molecular pathology. Surgery at an early age blocks the pathological process of intermittent exotropia, which potentially explains the better outcomes in the adolescent group.
In conclusion, our study showed that the medial recti in patients with intermittent exotropia manifest cellular and molecular pathology, with significantly higher levels of myosin and actin in adolescents compared with adult patients. These results suggest that early surgical intervention during adolescence may prevent further pathological damage to the extraocular muscles and improve the outcome. Our follow-up results show that the adolescent group manifests better postoperative visual function than the adult group.

References
Fu J, Li SM, Liu LR, Li JL, Li SY, Zhu BD et al. Prevalence of amblyopia and strabismus in a population of 7th-grade junior high school students in Central China: the Anyang Childhood Eye Study (ACES). Ophthalmic Epidemiol 2014; 21: 197–203.
Hashemi H, Yekta A, Jafarzadehpur E, Ostadimoghaddam H, Eshrati B, Mohazzab-Torabi S et al. The prevalence of strabismus in 7-year-old schoolchildren in Iran. Strabismus 2014; 22: 152–157.
Vaughan DG, Ashury T, Riordan Eva P . General Ophalthalmology, 14th edn. Appleton: New York, NY, USA, 1995; p 239.
Gralek M, Krawczyk T . [Pathomorphological evaluation of the extraocular muscles during strabismus]. Klin Oczna 1998; 100: 373–375.
Rungaldier S, Heiligenbrunner S, Mayer R, Hanefl-Krivanek C, Lipowec M, Streicher J et al. Ultrastructural and molecular biologic comparison of classic proprioceptors and palisade endings in sheep extraocular muscles. Invest Ophthalmol Vis Sci 2009; 50: 5697–5706.
Ruskell GL . Extraocular muscle proprioceptors and proprioception. Prog Retin Eye Res 1999; 18: 269–291.
Guanghuan Mai . Contemporary Treatment of Strabismus, 1st edn. People's Military Medical Press: Beijing, China, 1999.
Kim SH, Cho YA, Park CH, Uhm CS . The ultrastructural changes of tendon axonal profiles of medial rectus muscles according to duration in patients with intermittent exotropia. Eye (Lond) 2008; 22: 1076–1081.
Schneider CA, Rasband WS, Eliceiri KW . NIH Image to ImageJ: 25 years of image analysis. Nat Methods 2012; 9: 671–675.
Ribeiro Ede A Jr, Pinotsis N, Ghisleni A, Salmazo A, Konarev PV, Kostan J et al. The structure and regulation of human muscle alpha-actinin. Cell 2014; 159: 1447–1460.
von der Ecken J, Muller M, Lehman W, Manstein DJ, Penczek PA, Raunser S . Structure of the F-actin—tropomyosin complex. Nature 2014; 519: 114–117.
Pelouch V . Molecular aspects of regulation of cardiac contraction. Physiol Res 1995; 44: 53–60.
Hamdi MM, El-Hawary GR, El-Hefnawy NG, Salman MI . Histopathological and electron microscopic study for different grades of inferior oblique muscle overaction. Clin Ophthalmol 2013; 7: 917–921.
Berard-Badier M, Pellissier JF, Toga M, Mouillac N, Berard PV . Ultrastructural studies of extraocular muscles in ocular motility disorders. II. Morphological analysis of 38 biopsies. Albrecht Von Graefes Arch Klin Exp Ophthalmol 1978; 208: 193–205.
Caldeira JA . V-pattern esotropia: a review; and a study of the outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 78 consecutive patients. Binocul Vis Strabismus Q 2003; 18: 35–48; discussion 49–50.
van Waveren M, Jagle H, Besch D . Management of strabismus with hemianopic visual field defects. Graefes Arch Clin Exp Ophthalmol 2013; 251: 575–584.
Bui Quoc E, Milleret C . Origins of strabismus and loss of binocular vision. Front Integr Neurosci 2014; 8: 71.
Wang T, Wang LH . Surgical treatment for residual or recurrent strabismus. Int J Ophthalmol 2014; 7: 1056–1063.
Acknowledgements
This study was supported by a grant from the Bureau of Science and Technology of Suzhou city (No. SYS201334).
Author contributions
Jingyan Yao collected clinical specimen, conceived the experiments, and drafted the manuscript. Hang Ren performed the hematoxylin and eosin staining test. Xiangying Wang carried out the transmission electron microscopy assay. Gaoqin Liu participated in western blot and statistical analysis. Peirong Lu participated in the design of the study. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Yao, J., Wang, X., Ren, H. et al. Ultrastructure of medial rectus muscles in patients with intermittent exotropia. Eye 30, 146–151 (2016). https://doi.org/10.1038/eye.2015.213
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2015.213
This article is cited by
-
Quantitative measurement of passive duction force tension in intermittent exotropia and its clinical implications
Graefe's Archive for Clinical and Experimental Ophthalmology (2021)
