
Key Points
-
Investigates the attitudes of dentists towards the provision of periodontal treatment in general dental practice.
-
Examines GDPs' attitudes towards the referral of patients to specialist periodontists.
-
Explores what factors may influence referral decisions.
-
Explains specific barriers to referral or drivers of referral.
-
Describes how current referral pathways may be improved.
Abstract
Objective To examine the attitudes of dental practitioners towards specialist periodontal referral in the North East of England.
Subjects and methods Semi-structured interviews were conducted with a purposive sample of 10 practitioners. Interviews continued until data saturation occurred. The data were organised using a framework and analysed by two researchers working independently.
Results Perceptions of periodontal disease and treatment appear to be heavily influenced by the NHS remuneration system. Treatment in general practice was limited to simple scaling and there was an apparent reluctance to treat advanced periodontitis. Such cases were commonly referred to specialists, confirming the demand for a referral service in periodontics. The perceived potential for medico-legal consequences was a strong driver of referrals. Distance to the referral centre and the perceived costs of treatment were significant barriers to referral. Dentists valued the specialist's personal reputation and clinical skills more highly than academic status. Deficiencies in communication between primary and secondary care were highlighted.
Conclusions Increased resources are required to manage periodontal diseases within the NHS. There is a need for a periodontal referral service in the North East of England to improve accessibility to specialist care. This would appear to be most appropriately delivered by increased numbers of specialist practitioners.
Similar content being viewed by others

Introduction
There is continual debate and speculation concerning the future provision of dental care in the UK. For many years, patients have been referred by their general dental practitioner (GDP) to colleagues for advice or treatment.1 The hospital dental service accepts NHS referrals across the country, and there are also a number of practitioners who limit their practice to specific aspects of dentistry and accept referrals from other dentists. This process was formalised in 1998 with the advent of specialisation and the introduction of specialist lists by the General Dental Council (GDC).
In September 2003, the then Chief Dental Officer for England commissioned a review of the dentally based specialties by the Standing Dental Advisory Committee. The GDC has also recently reviewed the arrangements for training and listing of the dental specialties. Furthermore, a scheme for implementing 'Dentists with Special Interests' (DwSI) has been proposed. Under this scheme, a Primary Care Trust (PCT) would contract with individual dentists (who may not be on the relevant GDC specialist list) to provide enhanced services with improved access to meet the identified needs of their local population.
Eight years after the introduction of specialist lists by the GDC, there does not appear to have been any published research that has assessed the impact of formal specialisation. Indeed, there is very little research regarding primary care referrals in dentistry. Most studies have examined the characteristics of patients referred to specialist clinics rather than the actual referral process.2 Earlier research into specialist referrals in dentistry has generally been conducted from a secondary care perspective.3,4,5,6 Much of this work consists of simple cross-sectional studies of referrals to consultants in restorative dentistry. The attitudes of referring practitioners or the issues surrounding the referral process have generally not been considered. However, a wide variation in referral trends between different parts of the UK has been demonstrated, with difficulty accessing specialist care in some regions.7 There would appear to be a number of reasons for this variation, although dentists' attitudes regarding specialist referral have never been investigated in a primary care context. Dentistry finds itself in a unique position with hospital-trained consultants, specialists in practice and potentially, DwSI, all accepting referrals for 'specialist' dental care. In these changing times, it is useful to examine the attitudes that currently govern specialist referrals within the primary dental care environment.
Materials and methods
A purposive sample was taken to include a range of GDPs in the North East of England (Table 1), selected according to experience, postgraduate qualifications and proximity to a specialist. Subjects were chosen according to the length of time since qualification and possession of postgraduate qualifications to ensure a breadth of views within the sample.
Dentists were contacted by letter and invited to participate in an in-depth interview. Expenses were offered for the loss of their time, based on the British Dental Guild rate. The interviews were semi-structured, with a topic guide (Table 2) to explore attitudes towards specialist periodontal referral. All interviews were conducted by the same interviewer (GS) and were recorded then transcribed verbatim. In order to ensure validity, the interview transcripts were independently coded and analysed by two researchers (GS and JD) using a framework to assist with data management.8 The analysis was an inductive, iterative process whereby data collection and analysis took place concurrently until data saturation. This occurred after 10 interviews. The project was approved by the North West Multi-Centre Research Ethics Committee.
Data and discussion
Two broad themes emerged from the interviews. The first theme related to GDPs' perceptions of periodontal disease and treatment; the second theme concerned attitudes surrounding the referral process. A number of complex issues were revealed within these two broad areas. These issues are reported in more detail below using representative quotations to illustrate them. The letters in parentheses indicate the individual reference for each quote and the numbers refer to the practitioner who gave the quote.
Perceptions of general dental practitioners
Dentists in the study considered periodontal disease to be widespread. There was an implicit and an explicit negative attitude towards the treatment of periodontitis. This was seemingly based on the opinion that patients don't perceive periodontal treatment to be a pleasant (A) or necessary process (B), even after some discussion (C). This negativity seemed to be reinforced by patients' high 'failure to attend' rate for periodontal treatment appointments (D).
'Because it's not always... because, although you like... it's nice when you can get all the tartar off, most patients don't tolerate that.' (A, 1)
'Even if you tell them what you think the problem is, show them the OPG and try and explain about the bone loss and why the teeth are wobbly, a lot of them just don't want to hear of it.' (B, 2)
'I would say 'right', and I would do my little perio spiel. I'd get me little flip chart out, and just try to give a very basic idea of what's going on and why it's a problem. Some of them will then take a bit of interest.' (C, 2)
'Interestingly enough, of all my FTAs [failures to attend], nine out of 10 of them is scaling with the hygienist.' (D, 10)
Within the sample there was a degree of reliance on the hygienist (E) to provide periodontal treatment. The practitioners felt that hygienists were more highly skilled in performing periodontal therapy, and the remuneration provided by the NHS was insufficient for GDPs to spend the time required to provide periodontal treatment themselves (F). However, the convenience of undertaking scaling and polishing alongside other treatment was a factor (G); this would make periodontal treatment more financially viable for the dentist.
'Of all the patients that need perio I send them to the hygienist.' (E, 10)
'...she's got more time, she's cheaper, she can spend more time on it and she's better skilled at it and she does millions more than what we do.' (F, 10)
'Normally if, I mean if any S&Ps I do myself because just if you're doing anything else or if they're just in for a check up it's just easier just to get them done.' (G, 3)
The data suggested that cost was a major influence on patients' choice of treatment. As previously described, the patients were perceived to be reluctant to pay for expensive treatment. This was attributed to the complexity of the NHS fee structure, which was purported to make simpler treatment appear better value for money (H).
'Unfortunately within the realms of the NHS, the prices for 10b treatment [requiring more than 1 visit] is such a difference to prices for 10c treatment [over a minimum of 3 visits] so the initial... although they're getting twice the... well they're getting full mouth treatment, they don't perceive it as that. And if you tell someone it's £100 for what they see as a clean and polish, they think it's a lot. So sometimes you do have to do 10b treatment when really full mouth perio is in order.' (H, 6)
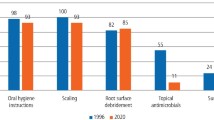
There was a trend towards providing simpler treatment, which is supported by recent activity data from the Dental Practice Board. For the quarter ending March 2005 in the North East, rates of scaling and polishing (item 10a) were 47.0 per 100 item-of-service claims compared to 3.0 for periodontal treatment involving two or more visits (items 10b and 10c). Figures for England and Wales as a whole also demonstrated a similar trend.
Previous research has highlighted that the current NHS fee structure is perceived not to reward complex treatment.2,9 Even in the management of mild chronic periodontitis, research has shown that many GDPs felt unable to allocate the time they believed was necessary, due to hopelessly inadequate NHS fees for such patients.10 As a result, it would appear that periodontal diseases are being under-managed within primary care dentistry.10 The findings of another qualitative study examining the provision of endodontic treatment also concluded that the NHS fee structure needs to be revised.11
Issues surrounding the referral process
Dentists in this study referred patients to Newcastle Dental Hospital with varying frequency. They appeared to be unaware of other referral centres and local specialist practitioners in their vicinity (I). As a result, dentists practicing some distance from Newcastle Dental Hospital tended to limit their number of referrals, apparently due to a perceived reluctance of their patients to travel long distances (J).
'I would [refer to a local specialist], but I just haven't heard of that service.' (I, 7)
'So because it's quite a way to go, I don't tend to send that many patients.' (J, 1)
Distance has previously been reported as a significant barrier to referral.2,7 Our results appear to reinforce this phenomenon and confirm the demand for local specialist referral services in periodontics.5,12 They also suggest that information regarding existing referral services should be more effectively disseminated. There was a perception that patients would be reluctant to pay for expensive courses of periodontal treatment, particularly if provided under private contract (K).
'...the financial restraints would come into it for a lot of our patients.' (K, 6)
Despite this, a number of common drivers of referral were apparent from the data. These included patients who had not responded to initial therapy (L), cases of advanced disease and those requiring a second opinion regarding diagnosis. The practitioners seemed to be divided in their opinion of whether to refer patients who didn't respond to initial non-surgical management; there was a cohort of practitioners who would refer, and another cohort that wouldn't. The decision to refer appeared to be influenced by the opinion of the hygienist (M). This is consistent with the finding that hygienists were reported to perform most of the treatment. Those GDPs who would not refer for specialist input appeared to base this decision firstly on their faith in the hygienist, and secondly on the opinion that the Dental Hospital would not do anything different from what they had already done. However, these decisions were implicitly influenced by distance from the referral centre (N).
'Well they [the referrals] tend to be for the patients that the hygienist has sort of been seeing for a while and they haven't improved.' (L, 1)
'Sometimes the hygienist asks me if I feel they'd be better off at the Dental Hospital for whatever reason.' (M, 8)
'I've felt that the hygienist does a good job and she seems she's very good... I mean the results I've seen from her work and patients who are coming back. I'm perfectly satisfied that she's doing what would be done in the hospital. And I think it's better for the patients.' (N, 3)
Unsurprisingly, if the practitioner diagnosed advanced or aggressive disease, they tended to refer. This echoes the findings of a recent survey published in Australia that investigated the factors influencing the diagnosis and treatment of periodontal disease by GDPs.13 A major apparent driver of referral was to seek reassurance in those cases where the practitioner felt that the patient wasn't accepting of their diagnosis. They therefore referred these patients for confirmation of their diagnosis to a specialist. This appeared to be mainly for those cases that required irreversible or extensive intervention and therefore potentially may have had an implicit medico-legal implication (O). It was intimated that patients may be more likely to believe the specialist due to their academic status, but the personal reputation and skills of the specialist appeared to be the major determinants of referral (P).
'They may believe... I mean even sometimes they'll just listen to us thinking 'Oh well, they're just a dentist' whereas they might go to the hospital, it's a consultant, might be a professor sat there that says 'look, these teeth need to come out' and they might... it might sink in a bit more.' (O, 3)
'He's probably done more perio treatment [in practice] than a lot of the consultants at the hospital have in the last ten years.' (P, 6)
When the practitioners were asked to describe their ideal referral service, there were positive feelings about the services they already had access to. The main aspect they believed could be improved was the length of the waiting lists (Q). Dentists' opinions on the administration of the ideal service varied greatly, but improved communication (R) and the ability to refer to a named specialist were cited routinely (S).
'The advice is good, the treatment is good. Waiting lists can be a bit long.' (Q, 10)
'I feel that you should be given letters saying that 'I've seen the patient and this is what I intend to do' and a letter when he's finished.' (R, 9)
'Well I'd be looking for someone firstly that I feel could do the job. And it would be nice to know the person that you sent them up to.' (S, 9)
In summary, the features of the ideal specialist referral service in periodontics appear to be accessibility, reputation and communication. The waiting lists for specialist treatment in the secondary care sector were criticised, and dentists wished that their patients would be seen more promptly. It appeared that GDPs would be more willing to refer patients if there were more local specialists available, without the need for patients to travel large distances.
Conclusions
The perceived poor remuneration and complex fee structure within the NHS seemed to limit periodontal treatment in primary care to simple scaling and polishing, with little time available for more comprehensive treatment by dental practitioners. This situation could change with the advent of PDS contracts, however it is not possible to comment any further on this from our data. Clearly, there is a requirement for increased resources to manage periodontal diseases within the NHS. There is certainly a demand for a high quality specialist periodontal referral service in the North East of England, as supported by previous research.12 In the present study, high levels of periodontal disease were reported and many dentists seemed to refer advanced cases to a specialist. It appears that some GDPs feel unable to provide more complex forms of periodontal treatment, and there is concern about possible medico-legal implications.
Distance to referral centres is a barrier to specialist referral and this has been reported by other researchers as having a major influence on referral rates.2,7,14 Poor communication between primary and secondary care providers was an issue, even if GDPs were satisfied with the treatment provided. The reputation and ability of specialists are valued highly by GDPs, but it was widely felt that patients would perceive the academic status of specialists to be of greater significance. Suggestions were made for the ideal referral service in periodontics relating to accessibility, reputation and communication. These issues could be addressed by the provision of more specialist practitioners in the region, and it is suggested that more resources should be made available for the training of such specialists.
References
Seward M . The changing role of specialist care in NHS dentistry. Br Dent J 1998; 184: 34–35.
Linden G J . Variation in periodontal referral by general dental practitioners. J Clin Periodontol 1998; 25: 655–661.
Basker R M, Harrison A, Ralph J P . A survey of patients referred to restorative dentistry clinics. Br Dent J 1988; 164: 105–108.
Callis P D, Charlton G, Clyde J S . A survey of patients seen in consultant clinics in conservative dentistry at Edinburgh Dental Hospital in 1990. Br Dent J 1993; 174: 106–110.
Ellis S G S, Ashley M P, Deans R F . A survey of referrals to a restorative dentistry department in a district general hospital. Eur J Prosthodont Restor Dent 2001; 9: 59–66.
Yemm R . Analysis of patients referred over a period of five years to a teaching hospital consultant service in dental prosthetics. Br Dent J 1985; 159: 304–306.
Linden G J, Stevenson M, Burke F J T . Variation in periodontal referral in 2 regions in the UK. J Clin Periodontol 1999; 6: 590–595.
Ritche J, Spencer J . Qualitative data analysis for applied policy research. In Bryman A, Burgess RG (eds) Analyzing qualitative data. London: Routledge, 1994.
Morris A J, Burke F J T . Primary and secondary dental care: how ideal is the interface. Br Dent J 2001; 191: 666–670.
Chapple I L C . Management of chronic periodontal diseases within the NHS. Br Dent J 2004; 196: 505.
McColl E, Smith M, Whitworth J, Seccombe G, Steele J . Barriers to improving endodontic care: the views of NHS practitioners. Br Dent J 1999; 186: 564–568.
Fairbrother K J, Nohl F S A . Perceptions of general dental practitioners of a local secondary care service in restorative dentistry. Br Dent J 2000; 188: 99–102.
Darby I B, Angkasa F, Duong C et al. Factors influencing the diagnosis and treatment of periodontal disease by dental practitioners in Victoria. Aust Dent J 2005; 50: 37–41.
Nixon P J, Benson R E . A survey of demand for specialist restorative dental services. Br Dent J 2005; 199: 161–163.
Acknowledgements
This study was funded in part by a Research Grant from the British Society of Periodontology.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Sharpe, G., Durham, J. & Preshaw, P. Attitudes regarding specialist referrals in periodontics. Br Dent J 202, E11 (2007). https://doi.org/10.1038/bdj.2007.141
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bdj.2007.141
This article is cited by
-
General dental practitioner views on the current and future provision of advanced NHS restorative dentistry services: a cross-sectional survey in England
British Dental Journal (2022)
-
Novel tier 2 service model for complex NHS endodontics
British Dental Journal (2021)
-
Patient choice of primary care practitioner for orofacial symptoms
British Dental Journal (2008)
