
Abstract
Background:
Spontaneous intestinal perforation (SIP) is increasingly common in the premature infant and is associated with significant morbidity. Indomethacin use has been implicated as a co-risk factor for SIP when combined with glucocorticoids, but previous evidence argued against indomethacin being an independent risk factor when used prophylactically.
Objectives:
(1) To establish a homogeneous cohort of SIP patients in a national data set and to contrast them to patients with surgical necrotizing enterocolitis (NEC). (2) To test the hypothesis that early post-natal indomethacin is independently associated with SIP.
Methods:
A large de-identified data set was retrospectively queried by diagnosis, and then multiple antenatal and post-natal variables were tested by both univariate and multivariate analysis to identify associations with SIP. Sub-analyses were also performed to look at the timing of drug administration.
Results:
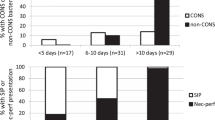
There were 2105 patients evaluated in the data set. Patients were divided into matched controls (n=581), those with SIP without report of NEC (n=633) and those with NEC requiring surgery (n=891). Infants with SIP were more likely to have a patent ductus arteriosus and more likely to be treated with vasopressors than either control or NEC patients. Compared to infants with NEC, patients with SIP were smaller, less mature and required more support. SIP was also diagnosed earlier than NEC (median of 7 vs 15 days). Patients with SIP were more likely to be treated with indomethacin, hydrocortisone or both on days of life 0–3 than controls.
Conclusions:
(1) Surgical NEC and SIP have significant differences in presentation, demographics and morbidity. (2) A detailed look at drug timing revealed that early post-natal indomethacin is independently associated with SIP.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Alpan G, Eyal F, Vinograd I, Udassin R, Amir G, Mogle P et al. Localized intestinal perforations after enteral administration of indomethacin in premature infants. J Pediatr 1985; 106: 277–281.
Aschner JL, Deluga KS, Metlay LA, Emmens RW, Hendricks-Munoz KD . Spontaneous focal gastrointestinal perforation in very low birth weight infants. J Pediatr 1988; 113: 364–367.
Scholz TD, McGuinness GA . Localized intestinal perforation following intravenous indomethacin for patent ductus arteriosus. J Pediatr Gastroenterol Nutr 1988; 7: 773–775.
Meyer CL, Payne NR, Roback SA . Spontaneous, isolated intestinal perforations in neonates with birth weight less than 1000 g not associated with necrotizing enterocolitis. J Pediatr Surg 1991; 26: 714–717.
Nagaraj HS, Sandhu AS, Cook LN, Buchino JJ, Groff DB . Gastrointestinal perforation following indomethacin therapy in very low birth weight infants. J Pediatr Surg 1981; 16: 1003–1007.
Schmidt B, Davis P, Moddemann D, Ohlsson A, Roberts RS, Saigal S et al. Long-term effects of indomethacin prophylaxis in extremely-low-birth-weight infants. N Engl J Med 2001; 344: 1966–1972.
Stark AR, Carlo WA, Tyson JE, Papile LA, Wright LL, Shankaran S et al. Adverse effects of early dexamethasone in extremely-low-birth-weight infants. National institute of child health and human development neonatal research network. N Engl J Med 2001; 344: 95–101.
Watterberg KL, Gerdes JS, Cole CH, Aucott SW, Thilo EH, Mammel MC et al. Prophylaxis of early adrenal insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. Pediatrics 2004; 114: 1649–1657.
Guthrie SO, Gordon PV, Thomas V, Thorp JA, Peabody J, Clark RH . Necrotizing enterocolitis among neonates in the United States. J Perinatol 2003; 23: 278–285.
Fujii AM, Brown E, Mirochnick M, O'Brien S, Kaufman G . Neonatal necrotizing enterocolitis with intestinal perforation in extremely premature infants receiving early indomethacin treatment for patent ductus arteriosus. J Perinatol 2002; 22: 535–540.
Garland JS, Alex CP, Pauly TH, Whitehead VL, Brand J, Winston JF et al. A three-day course of dexamethasone therapy to prevent chronic lung disease in ventilated neonates: a randomized trial. Pediatrics 1999; 104: 91–99.
Vermont Oxford Network Steroid Study Group. Early postnatal dexamethasone therapy for the prevention of chronic lung disease. Pediatrics 2001; 108: 741–748.
Gordon P, Rutledge J, Sawin R, Thomas S, Woodrum D . Early postnatal dexamethasone increases the risk of focal small bowel perforation in extremely low birth weight infants. J Perinatol 1999; 19: 573–577.
Gordon PV, Young ML, Marshall DD . Focal small bowel perforation: an adverse effect of early postnatal dexamethasone therapy in extremely low birth weight infants. J Perinatol 2001; 21: 156–160.
Watterberg KL . Weighing statistical certainty against ethical, clinical, and biologic expediency: the contributions of the Watterberg trial tip the scales in the right direction: in reply. Pediatrics 2005; 115: 1447.
Acknowledgements
Dr Gordon was supported by NIH NIDDK Grant 1KO8DK/HD61553-01. We are grateful to Sheryl Mroz and Sarabeth Gordon, MS for their editorial support and to all the caregivers within Pediatrix for their daily attentiveness to the electronic note system.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary information is available on the Journal of Perinatology website (http://www.nature.com/jp)
Supplementary information
Rights and permissions
About this article
Cite this article
Attridge, J., Clark, R., Walker, M. et al. New insights into spontaneous intestinal perforation using a national data set: (1) SIP is associated with early indomethacin exposure. J Perinatol 26, 93–99 (2006). https://doi.org/10.1038/sj.jp.7211429
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211429
Keywords
This article is cited by
-
Risk factors and epidemiology of spontaneous intestinal perforation among infants born at 22–24 weeks’ gestational age
Journal of Perinatology (2024)
-
Prophylactic indomethacin, antenatal betamethasone, and the risk of intestinal perforation in infants <28 weeks’ gestation
Journal of Perinatology (2023)
-
Patent ductus arteriosus and spontaneous intestinal perforation in a cohort of preterm infants
Journal of Perinatology (2022)
-
Spontaneous intestinal perforation (SIP) will soon become the most common form of surgical bowel disease in the extremely low birth weight (ELBW) infant
Journal of Perinatology (2022)
-
Spontaneous intestinal perforation in premature infants: a national study
Journal of Perinatology (2021)
