
Abstract
Mitotic centromere-associated kinesin (MCAK) is a microtubule depolymerase that is essential for proper kinetochore–microtubule attachment during spindle formation. Overexpression of MCAK has been correlated with aggressive forms of carcinoma, resulting in poor prognosis of colorectal cancer. The purpose of this study was to quantify MCAK expression in malignant and benign colorectal tissues and to determine if MCAK expression levels correlate with clinicopathologic factors and prognosis in colorectal cancer patients. Paired colorectal tissue samples from tumours and the corresponding normal tissues were obtained from 120 patients with colorectal cancer who underwent surgical resection. The real-time reverse transcriptase-PCR and immunohistochemistry were used to analyse mRNA and protein expression status with respect to various clinicopathological factors. MCAK expression was higher in colorectal cancer tissue (P<0.01) than in corresponding normal tissue, and this elevated expression level was markedly associated with factors such as lymph node metastasis (P=0.0023), venous invasion (P=0.019), peritoneal dissemination (P=0.021) and Dukes' classification (P=0.0023). Patients with high MCAK mRNA expression also showed a far poorer survival rate than those with low MCAK mRNA expression (P<0.01). Elevated MCAK expression was an independent predictor of overall survival and lymph node metastasis. These data suggest that MCAK expression may serve as a good marker of prognosis and lymph node metastasis in colorectal cancer.
Similar content being viewed by others

Main
Colorectal cancer is one of the most prevalent cancers in the world, accounting for nearly 10% of all cancer cases (Parkin et al, 2001). In Japan, the incidence of colorectal cancer has significantly increased during the past 50 years, in concert with changes in eating habits, other lifestyle parameters and longevity (Kono, 1996). Colorectal cancer is now the second most important cause of death from neoplastic disease in Japan (Tsukuma et al, 2004). Identification of the genes responsible for the development and progression of colorectal cancer is critical if improvements are to be made in the diagnosis and treatment of the disease.
Chromosomal instability, a recognisable feature of human cancers, is caused by continuous chromosomal missegregation during mitosis (Tomonaga et al, 2005). A physical connection (i.e., a kinetochore) between the spindle microtubules (MTs) and centromeric DNA is essential for appropriate chromosomal segregation (Tomonaga et al, 2005). During spindle formation, mitotic centromere-associated kinesin (MCAK), a microtubule depolymerase, ensures proper kinetochore–MT attachment (Holmfeldt et al, 2005). An attachment failure leads to missegregation of individual chromosomes.
MCAK, located at chromosome 1p34.1, is a member of the kinesin-13 subfamily that shares homology with other members of the kinesin superfamily (Wordeman and Mitchison, 1995; Vale and Fletterick, 1997; Lawrence et al, 2004) that play important roles in intracellular transport and cell division (Wittmann et al, 2001). Mitotic centromere-associated kinesin is present throughout the cell, but is especially concentrated at the centromeres, kinetochores and spindle poles (Gorbsky, 2004). Although other kinesins act to transport cargo, MCAK and other kinesin-13 members catalyse MT disassembly, an important factor in normal chromosome movement (Helenius et al, 2006). Mitotic centromere-associated kinesin destabilises MTs from either end, and this activity and localisation are under the regulation of mitotic kinases (Wordeman et al, 2007). Overexpression of wild-type MCAK induces destabilisation of MTs in both mitotic and interphase cells (Kline-Smith and Walczak, 2002).
We recently reported that elevated MCAK expression is associated with lymphatic invasion, lymph node metastasis and poor prognosis in gastric cancer (Nakamura et al, 2007). Although MCAK mRNA is also highly expressed in colorectal cancer tissues (Mori et al, 1993a), no clinicopathologic analysis of MCAK expression in human colorectal cancer has been reported. In this study, we explored MCAK gene expression in human colorectal cancer and evaluated possible associations of gene expression with clinicopathological factors and prognosis.
Materials and methods
Cell lines and clinical tissue samples
Cell lines derived from human colorectal cancer (DLD1, COLO201, COLO205, COLO320DM, HT29, HCT15, WiDr, SW480, LS174T, CCK81, RCM1 and CaR1) were obtained from the Cell Resource Centre for Biomedical Research Institute of Development, Aging and Cancer (Tohoku University, Sendai, Japan) and maintained in RPMI-1640 containing 10% fetal bovine serum and antibiotics at 37°C in a 5% humidified CO2 atmosphere.
One hundred and twenty patients (70 men, 50 women) with colorectal cancer who underwent surgery at the Medical Institute of Bioregulation at Kyushu University from 1994 to 1999 were included in this study. Primary colorectal cancer specimens and adjacent normal colorectal mucosa were obtained from patients after informed consent had been obtained in accordance with the institutional guidelines of the hospital. Immediately after resection, the necrotic and ulcerated portions of the tumours were removed and normal colonic mucosa was dissociated from muscle and connective tissue. All specimens were immediately frozen in liquid nitrogen and kept at −80°C until RNA extractions were performed. Every patient was definitively identified as having colorectal cancer based on the clinicopathologic findings. None of the patients received chemotherapy or radiotherapy prior to surgery. Clinicopathological factors were assessed according to the criteria of the Japanese Classification of Colorectal Carcinoma (Japanese Society for Cancer Colon and Rectum, 1998). All patients were closely followed after surgery at regular 1-month intervals for 2–72 months, with a mean follow-up period of 38.4 months. This study was conducted under the supervision of the ethical board of Kyushu University.
RNA preparation and reverse transcription
Total RNA was isolated using a modified acid guanidinium–phenol–chloroform procedure with DNase (Mimori et al, 1997). cDNA was synthesised from 2.5 μg of total RNA as described previously (Mori et al, 1993b).
MCAK gene amplification
A 237-bp MCAK fragment was amplified with the following primers: 5′-GATGGAAGCCTGCTCTAACG-3′ (forward) and 5′-GAGCAGATTCCGCTTTGTTC-3′ (reverse). The forward primer is located in exon 8 and the reverse primer in exon 9. The amplification parameters were 1 min at 95°C, 1 min at 62°C and 1 min at 72°C for 28 cycles. An 8-μl aliquot of each reaction mixture was size-fractionated in a 2% agarose gel and visualised by ethidium bromide staining. To ensure that the RNA was not degraded, a PCR assay with primers specific for the glyceraldehyde-3-phosphate dehydrogenase (GAPDH) gene was performed for 1 min at 95°C, 1 min at 56°C and 1 min at 72°C for 28 cycles. The GAPDH primers 5′-TTGGTATCGTGGAAGGACTCA-3′ (forward) and 5′-TGTCATCATATTTGGCAGGTT-3′ (reverse) produced a 270-bp amplicon (Ogawa et al, 2004). cDNA from the Human Universal Reference Total RNAs (Clontech, Palo Alto, CA, USA) was studied concurrently as a source of positive controls. Confirmation of reverse transcriptase-PCR (RT-PCR) products was performed by direct sequencing analysis.
Real-time quantitative reverse transcriptase-PCR
Real-time monitoring of the PCRs was performed using the LightCycler FastStart DNA Master SYBR Green I Kit (Roche Diagnostics, Tokyo, Japan). The amplification protocol consisted of 35 cycles of denaturation at 95°C for 10 s, annealing at 64°C for 10 s and elongation at 72°C for 10 s. The products were then subjected to a temperature gradient from 68°C to 95°C at 0.1°C s−1 with continuous fluorescence monitoring to produce a melting curve of the products. After proportional background adjustment, the fit point method was used to determine the cycle in which the log-linear signal was distinguished from the background, and that cycle number was used as a crossing-point value. The standard curve was produced by measuring the crossing point of each standard value (twofold serially diluted cDNAs from the Human Universal Reference Total RNAs) and plotting them against the logarithmic value of the concentration. The concentration of each sample was then calculated by setting their crossing points to the standard curve. The expression levels were normalised against GAPDH mRNA expression (Ogawa et al, 2004).
Immunohistochemistry
Colorectal cancer surgical specimens from formalin-fixed, paraffin-embedded tissues were used for MCAK immunohistochemistry. After deparaffinisation and blocking, the antigen–antibody reaction was incubated overnight at 4°C. ENVISION reagents (ENVISION+Dual Link/HRP; Dako Cytomation, Glostrup, Denmark) were applied to detect the signal from the antigen–antibody reaction. All sections were counterstained with haematoxylin. The primary anti-MCAK goat polyclonal antibody (ab5966; Abcam, Cambridge, UK) was used at a dilution of 1 : 500.
Statistical analysis
For continuous variables, the data were expressed as the mean±s.d. The relationship between MCAK mRNA expression and the clinicopathological factors was analysed by the χ2 test and Student's t-test. Kaplan–Meier survival curves were plotted and compared with the generalised log rank test. Prognostic factors were evaluated by univariate and multivariate analyses (Cox proportional hazard regression model). A logistic regression model was used to identify the independent predictors of lymph node metastasis. All tests were analysed by JMP software (SAS Institute, Cary, NC, USA), and the findings were considered statistically significant at P<0.05.
Results
MCAK mRNA expression in colorectal cancer cell lines and clinical tissue specimens
Figure 1A shows MCAK gene expression status in human colorectal cancer cell lines from RT-PCR analysis. Twelve of the 13 cell lines (92%) expressed the MCAK gene; COLO201 was the exception. We also performed RT-PCR analysis of MCAK in colorectal cancers and paired normal samples obtained from seven patients. In all seven cases, MCAK expression was higher in the cancer tissues than in paired normal tissue (Figure 1B). Quantitative real-time RT-PCR was performed using the Human Total RNA Master Panel (Clontech) to characterise MCAK mRNA expression. MCAK expression was extremely high in the testis. Lower expression was found in the digestive organs (colon and intestines), possibly a reflection of basic mitosis of the mucosa (data not shown). Moreover, quantitative real-time RT-PCR on 120 paired clinical samples showed that 91 of 120 cases (75.8%) exhibited higher levels of MCAK mRNA in tumours than in paired normal samples. The mean expression value of MCAK mRNA in tumour samples, 0.53±0.037 (mean±s.d., normalised by GAPDH gene expression), was significantly higher than the value, 0.32±0.037, for the corresponding normal samples (P<0.01; Student's t-test).

MCAK mRNA expression in colorectal cancer cell lines and clinical tissue specimens. (A) Reverse transcriptase-PCR analysis of MCAK expression in human colorectal cancer cell lines. Twelve of the 13 cell lines (92%) expressed the MCAK gene, whereas COLO201 did not. (B) Reverse transcriptase-PCR analysis of MCAK expression in clinical samples of colorectal cancer. MCAK expression was determined in the colorectal tumours (T) and paired normal (N) samples obtained from seven patients. In all seven cases, MCAK expression was higher in the tumours than in the normal tissues. GAPDH was used as a loading control. m=marker; NC=negative control; PC=positive control.
Immunohistochemistry
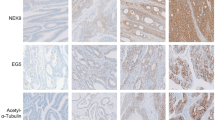
A positive immunohistochemical staining pattern for MCAK in tissue from a colorectal cancer patient is shown in Figure 2A and B. Mitotic centromere-associated kinesin protein staining was observed in the cytoplasm of cancer cells, but not in the stromal cells nor in normal epithelium. Mitotic centromere-associated kinesin protein expression was examined in the tumours and corresponding normal tissues from 15 representative colorectal cancer cases. Of these 15 cases, seven exhibited a higher level of MCAK mRNA expression in tumour tissues, whereas the remaining eight cases showed a lower level of MCAK mRNA in cancerous tissue. All sections were independently examined for protein expression and scored as positive or negative when >10% (positive) or <10% (negative) of carcinoma cells were stained in an examined area of a specimen. As a result, nine of the representative cases showed a positive reaction for MCAK, whereas six cases were negative. The data were similar to those obtained from MCAK mRNA expression analysis. The six negative tumours (Figure 2C and D) also showed lower mRNA expression levels, while seven of the nine positive tumours (Figure 2A and B) showed higher mRNA expression levels. These data suggest that MCAK mRNA expression is associated with protein expression.

Immunohistochemical staining for MCAK in tumour specimens. (A and B) A representative positive stain for MCAK in tissue from a colorectal cancer patient. Positive staining is observed in the cytoplasm of cancer cells, but not in the stromal cells nor in normal epithelium. Solid line arrows indicate cancer cells that are positive for MCAK expression. (C and D) A representative negative stain for MCAK in a colorectal cancer specimen. Dotted line arrows indicate cancer cells that are negative for MCAK expression. Mitotic centromere-associated kinesin protein expression was evaluated in tumours and corresponding normal tissues from 15 representative colorectal cancer cases. The six tumours that were negative for protein expression (C and D) also exhibited lower mRNA expression levels, whereas seven of nine tumours with a positive immunohistochemical expression (A and B) displayed elevated mRNA expression levels. The expression of MCAK mRNA was thereby associated with protein expression. Each solid square in (A) and (C) was magnified × 100 and shown in (B) and (D), respectively (original magnification; (A) and (C), × 40; (B) and (D), × 100).
MCAK mRNA expression and clinicopathological characteristics
The experimental samples were divided into two expression groups. Patients who had less than the median expression ratio of tumour to normal tissue (T/N) were assigned to the low-expression group (n=81); the others were assigned to the high-expression group (n=39). Clinicopathological factors related to MCAK expression status are listed in Table 1. The incidence of three of these factors was positively correlated with increased expression (i.e., the high-expression group): (1) lymph node metastasis was significantly higher (P=0.0023) in the high-expression group (25 of 39, 64.1%) than in the low-expression group (28 of 81, 34.6%); (2) the incidence of venous invasion was significantly higher (P=0.019) in the high-expression group (13 of 39, 33.3%) than in the low-expression group (12 of 81, 14.8%); and (3) the incidence of peritoneal dissemination was significantly higher in the high-expression group (4 of 39, 10.3%) than in the low-expression group (1 of 81, 1.23%). Moreover, the incidence of advanced stage cancer (according to Dukes' classification) was significantly higher (P=0.0023) in the high-expression group (26 of 39, 66.7%) than in the low-expression group (30 of 81, 37.0%). The other clinicopathological factors were not correlated with MCAK overexpression.
Relationship between MCAK expression and prognosis
The 5-year survival rate was significantly lower in patients with elevated MCAK expression (P<0.01; Figure 3). Table 2 provides the univariate and multivariate analyses of factors related to patient prognosis. Univariate analysis showed that the following factors were significantly related to postoperative survival: tumour size (P=0.009), serosal invasion (P<0.0001), lymph node metastasis (P<0.0001), lymphatic invasion (P<0.0001) and MCAK mRNA expression (P=0.019). Multivariate regression analysis indicated that inclusion in the MCAK mRNA high-expression group (relative risk (RR), 1.42; 95% confidence interval (CI), 1.01–2.00; P<0.05) was an independent predictor of overall survival, as were serosal invasion (RR, 2.16; 95% CI, 1.52–3.12; P<0.0001) and lymph node metastasis (RR, 1.82; 95% CI, 1.26–2.76; P=0.0012).

Kaplan–Meier survival curves of patients with colorectal cancer based on MCAK mRNA expression status. Patients in the high-expression group (bold line) showed significantly poorer prognosis than those in the low-expression group (dotted line; P<0.01, log rank test).
Multivariate analysis for lymph node metastasis
Univariate and multivariate logistic regression analyses were performed on lymph node metastasis (Table 3). Univariate analysis revealed a significant relationship between lymph node metastasis and the following factors: histological grade (P=0.04), tumour size (P=0.01), depth of invasion (P=0.02), lymphatic invasion (P<0.0001), venous invasion (P=0.003) and MCAK mRNA expression (P=0.003). Multivariate regression analysis indicated that inclusion in the MCAK mRNA high-expression group (RR, 4.02; 95% CI, 1.53–11.3; P<0.006) was an independent predictor of lymph node metastasis in addition to lymphatic invasion (RR, 7.67; 95% CI, 3.01–21.1; P<0.0001).
Discussion
In this study, we demonstrated that MCAK is expressed at higher levels in colorectal cancer cells than in the corresponding normal tissues. Mitotic centromere-associated kinesin overexpression causes a moderate increase in the frequency of multipolar spindles (Holmfeldt et al, 2004) and monopolar spindles (Kline-Smith and Walczak, 2002), which can contribute to the gain or loss of chromosomes in daughter cells. We reported that overexpression of MCAK leads to the increased migratory and proliferative ability of gastric cancer cells (Nakamura et al, 2007). Microtubules, key components of the cytoskeleton, play essential roles in mitosis, cell migration, and cell signalling and trafficking (Honore et al, 2005). Mitotic centromere-associated kinesin is present throughout the cell, and overexpression of MCAK may accelerate MT turnover, resulting in the gain of cancer cell motility. This result may partially explain the finding that gastric cancer patients with tumours that express high levels of MCAK had higher rates of lymphatic invasion and metastasis, and a poorer prognosis. Along the same line, downregulation of MCAK in a breast cancer study resulted in tumour growth suppression (Shimo et al, 2008). These findings suggest that overexpression of MCAK enhances the malignancy of cancer cells.
Clinicopathological analysis revealed that tumours with high MCAK expression were associated with lymph node metastasis, venous invasion, peritoneal dissemination and advanced Dukes' stage. In our previous study on gastric cancer, MCAK gene expression in cancer tissues was significantly higher than expression in nonmalignant tissue, and elevated MCAK expression was significantly associated with lymphatic invasion and lymph node metastasis (Nakamura et al, 2007). These results suggest that MCAK plays a pivotal role in the progression of colorectal cancer and gastric cancer. Moreover, in both studies, patients with high MCAK expression had a poorer survival rate than those with low MCAK expression, and high MCAK expression was an independent prognostic factor for overall survival in the Cox proportional hazard regression model. To our knowledge, this is the first report on correlations between MCAK gene expression and clinicopathological factors in colorectal cancer. In the majority of colorectal cancer reports, gene expression is secondary to TNM or Dukes' classification as a prognostic marker. Because its expression is an independent prognostic factor, the expression profile of MCAK may contribute to the creation of a new clinical classification system.
Another aspect of this study is the relationship between MCAK expression and lymphatic extension. Interestingly, multivariate analysis for lymph node metastasis revealed that MCAK mRNA expression is a good predictor of lymph node metastasis. Lymph node metastases are the most important predictors of survival in non-stage IV colorectal cancer (Schumacher et al, 2007). Today, we have several options for curative treatment of early colorectal cancer, such as endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD) and laparoscopic-assisted colectomy with regional lymphadenectomy. In limited cases, patients are eligible for such less invasive surgery. Patients suitable for those endoscopic treatments are selected by the preoperative diagnosis of lymph node metastasis, such as macroscopic type, tumour size, presence of an ulcer and histology of biopsy specimens. However, some patients are misdiagnosed and actually do have lymph node metastasis before the operation. By incorporating the genetic diagnosis of MCAK gene expression, preoperative selection for patients without lymph node metastasis may be possible. Furthermore, it has been reported that with SELEX, MCAK was detected in the peripheral blood of a colon cancer patient (Scanlan et al, 2002), suggesting that the blood level of MCAK can be used for the prediction of lymph node metastasis. The analysis of MCAK using biopsied specimens and blood samples could provide a more accurate evaluation, which might translate to minimally invasive treatments for early colorectal cancer.
In conclusion, the expression of MCAK in colorectal cancer was elevated respective to levels in normal colorectal tissue, and this overexpression was associated with lymph node metastasis, venous invasion, peritoneal dissemination and poor prognosis. In particular, MCAK mRNA overexpression was associated with prognosis and lymph node metastasis in a multivariate analysis. Therefore, MCAK could be a useful predictive marker of lymph node metastasis, which might permit minimally invasive and curative treatments combining EMR and ESD for early colorectal cancer.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Gorbsky GJ (2004) Mitosis: MCAK under the aura of Aurora B. Curr Biol 14: R346–R348
Helenius J, Brouhard G, Kalaidzidis Y, Diez S, Howard J (2006) The depolymerizing kinesin MCAK uses lattice diffusion to rapidly target microtubule ends. Nature 441: 115–119
Holmfeldt P, Stenmark S, Gullberg M (2004) Differential functional interplay of TOGp/XMAP215 and the KinI kinesin MCAK during interphase and mitosis. EMBO J 23: 627–637
Holmfeldt P, Zhang X, Stenmark S, Walczak CE, Gullberg M (2005) CaMKIIgamma-mediated inactivation of the Kin I kinesin MCAK is essential for bipolar spindle formation. EMBO J 24: 1256–1266
Honore S, Pasquier E, Braguer D (2005) Understanding microtubule dynamics for improved cancer therapy. Cell Mol Life Sci 62: 3039–3056
Kline-Smith SL, Walczak CE (2002) The microtubule-destabilizing kinesin XKCM1 regulates microtubule dynamic instability in cells. Mol Biol Cell 13: 2718–2731
Kono S (1996) Dietary factors for gastrointestinal cancers: a worldwide overview. Gann Monogr Cancer Res 44: 29–39
Lawrence CJ, Dawe RK, Christie KR, Cleveland DW, Dawson SC, Endow SA, Goldstein LS, Goodson HV, Hirokawa N, Howard J, Malmberg RL, McIntosh JR, Miki H, Mitchison TJ, Okada Y, Reddy AS, Saxton WM, Schliwa M, Scholey JM, Vale RD, Walczak CE, Wordeman L (2004) A standardized kinesin nomenclature. J Cell Biol 167: 19–22
Mimori K, Mori M, Shiraishi T, Fujie T, Baba K, Haraguchi M, Abe R, Ueo H, Akiyoshi T (1997) Clinical significance of tissue inhibitor of metalloproteinase expression in gastric carcinoma. Br J Cancer 76: 531–536
Mori M, Barnard GF, Staniunas RJ, Jessup JM, Steele Jr GD, Chen LB (1993a) Prothymosin-alpha mRNA expression correlates with that of c-myc in human colon cancer. Oncogene 8: 2821–2826
Mori M, Staniunas RJ, Barnard GF, Jessup Jr JM, Steele GD, Chen LB (1993b) The significance of carbonic anhydrase expression in human colorectal cancer. Gastroenterology 105: 820–826
Nakamura Y, Tanaka F, Haraguchi N, Mimori K, Matsumoto T, Inoue H, Yanaga K, Mori M (2007) Clinicopathological and biological significance of mitotic centromere-associated kinesin overexpression in human gastric cancer. Br J Cancer 97: 543–549
Ogawa K, Utsunomiya T, Mimori K, Tanaka Y, Tanaka F, Inoue H, Murayama S, Mori M (2004) Clinical significance of elongation factor-1 delta mRNA expression in oesophageal carcinoma. Br J Cancer 91: 282–286
Parkin DM, Bray F, Ferlay J, Pisani P (2001) Estimating the world cancer burden: Globocan 2000. Int J Cancer 94: 153–156
Japanese Society for Cancer Colon and Rectum (1998) General Rules for Clinical and Pathological Studies on Cancer of the Colon, Rectum and Anus 6th edn. Tokyo: Kanehara
Scanlan MJ, Welt S, Gordon CM, Chen YT, Gure AO, Stockert E, Jungbluth AA, Ritter G, Jager D, Jager E, Knuth A, Old LJ (2002) Cancer-related serological recognition of human colon cancer: identification of potential diagnostic and immunotherapeutic targets. Cancer Res 62: 4041–4047
Schumacher P, Dineen S, Barnett Jr C, Fleming J, Anthony T (2007) The metastatic lymph node ratio predicts survival in colon cancer. Am J Surg 194: 827–831; discussion 831–822
Shimo A, Tanikawa C, Nishidate T, Lin ML, Matsuda K, Park JH, Ueki T, Ohta T, Hirata K, Fukuda M, Nakamura Y, Katagiri T (2008) Involvement of kinesin family member 2C/mitotic centromere-associated kinesin overexpression in mammary carcinogenesis. Cancer Sci 99: 62–70
Tomonaga T, Matsushita K, Ishibashi M, Nezu M, Shimada H, Ochiai T, Yoda K, Nomura F (2005) Centromere protein H is up-regulated in primary human colorectal cancer and its overexpression induces aneuploidy. Cancer Res 65: 4683–4689
Tsukuma H, Ajiki W, Oshima A (2004) [Cancer incidence in Japan]. Gan To Kagaku Ryoho 31: 840–846
Vale RD, Fletterick RJ (1997) The design plan of kinesin motors. Annu Rev Cell Dev Biol 13: 745–777
Wittmann T, Hyman A, Desai A (2001) The spindle: a dynamic assembly of microtubules and motors. Nat Cell Biol 3: E28–E34
Wordeman L, Mitchison TJ (1995) Identification and partial characterization of mitotic centromere-associated kinesin, a kinesin-related protein that associates with centromeres during mitosis. J Cell Biol 128: 95–104
Wordeman L, Wagenbach M, von Dassow G (2007) MCAK facilitates chromosome movement by promoting kinetochore microtubule turnover. J Cell Biol 179: 869–879
Acknowledgements
We thank Dr Y Nakamura, Ms T Shimooka, Ms K Ogata, Ms M Kasagi and Ms Y Nakagawa for their technical assistance and advice. This work was supported in part by the following grants and foundations: CREST, Japan Science and Technology Agency; Japan Society for the Promotion of Science Grant-in-Aid for Scientific Research, grants 17109013, 17591411, 17591413, 18390367, 18590333, 18659384, 18790964, 19890336 and 19591509; The Ministry of Education, Culture, Sports, Science and Technology Grant-in-Aid for Scientific Research on Priority Areas, Grant 18015039; Third Term Comprehensive Ten-Year Strategy for Cancer Control, Grant 16271201.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Ishikawa, K., Kamohara, Y., Tanaka, F. et al. Mitotic centromere-associated kinesin is a novel marker for prognosis and lymph node metastasis in colorectal cancer. Br J Cancer 98, 1824–1829 (2008). https://doi.org/10.1038/sj.bjc.6604379
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6604379
Keywords
This article is cited by
-
KIF2C is a prognostic biomarker associated with immune cell infiltration in breast cancer
BMC Cancer (2023)
-
Bioinformatical analysis of the key differentially expressed genes for screening potential biomarkers in Wilms tumor
Scientific Reports (2023)
-
Kinesin family member 18B regulates the proliferation and invasion of human prostate cancer cells
Cell Death & Disease (2021)
-
KIF2C: a novel link between Wnt/β-catenin and mTORC1 signaling in the pathogenesis of hepatocellular carcinoma
Protein & Cell (2021)
-
Intravital imaging of SRF and Notch signalling identifies a key role for EZH2 in invasive melanoma cells
Oncogene (2015)
