
Abstract
The extent of deprivation (Carstairs deprivation index) was directly associated with the magnitude of the systemic inflammatory response (reduced albumin and elevated C-reactive protein, P<0.01) in patients with primary operable breast cancer (n=314). Deprivation was not associated with age, tumour size, tumour type, grade, and the proportion of patients with involved lymph nodes and oestrogen receptor status.
Similar content being viewed by others

Main
Breast cancer is the commonest female malignancy in the Western World. In the UK, the lifetime risk is now one in nine and the incidence is rising by about 2% per year (www.cancerresearchuk.org/statistics).
It is now recognised that socioeconomic deprivation is associated with poor outcome in women with breast cancer (Schrijvers et al, 1995; McLaren and Bain, 1998; Thomson et al, 2001). For example, Thomson et al (2001), in a cohort of almost 22 000 women with primary breast cancer, reported a 10% survival difference between affluent and deprived. The basis of this relationship remains unclear. This difference does not appear to be related to tumour size or nodal status, nor access to hospital care, surgical management or the use of adjuvant therapy (Macleod et al, 2000; Brewster et al, 2001; Thomson et al, 2001). However, there is evidence to suggest that there is an association between deprivation and oestrogen receptor (ER) status, the deprived having more ER negative tumours (Thomson et al, 2001). However, ER status accounted for less than 20% of the difference in survival.
Recently, the systemic inflammatory response as evidenced by C-reactive protein, the prototypical marker of the systemic inflammatory response (Gabay and Kushner, 1999), has been shown to be associated with poor outcome in patients with colorectal and lung cancer (Scott et al, 2002; McMillan et al, 2003a). Furthermore, in patients with colorectal cancer, the presence of a systemic inflammatory response appeared to account for the effect of deprivation on cancer survival (McMillan et al, 2003b). To our knowledge, the nature of the relationship between deprivation, stage at presentation and the systemic inflammatory response in patients with primary operable breast cancer has not been previously examined.
The aim of the present study was to examine the relationship between deprivation, stage at presentation and the systemic inflammatory response in patients with primary operable breast cancer.
Patients and methods
In total, 314 patients presenting with invasive primary operable breast cancer to three consultant surgeons (JCD, AL and CW) in two hospitals (Western Infirmary, Glasgow and Wishaw General Hospital, Lanarkshire) in the West of Scotland between July 2001–July 2003 were included in the study.
Prior to surgery, a blood sample was obtained for the measurement of albumin and C-reactive protein. At this time no patients showed clinical evidence of infection or other inflammatory conditions.
Age, deprivation category, tumour size, histological type and grade, oestrogen receptor status and lymph node status were recorded. The extent of deprivation was defined using the Carstairs deprivation index (Carstairs and Morris, 1991). This is an area-based measure derived from the 1991 census, using the postcode of residence at diagnosis, which divides the score into a seven-point index. For illustrative purposes, the results are presented by amalgamating the seven categories into three groups: affluent (categories 1 and 2), intermediate (categories 3–5) and deprived (categories 6 and 7). The Carstairs deprivation index has been extensively utilised in cancer patients (Edwards and Jones, 1999) and is particularly appropriate for use in the central belt of Scotland (MacKie and Hole, 1996).
The study was approved by the local Research Ethics committees.
Blood parameters: Routine laboratory measurements of C-reactive protein and albumin concentrations were carried out. The coefficient of variation was less than 5% as established by routine quality control procedures. The limit of detection of the assay is a C-reactive protein concentration of less than 6 mg l−1.
Statistics
As appropriate, comparisons between patient groups were carried out using the χ2-test. Statistical analysis was based on the seven individual deprivation categories. In the absence of a predefined and recognised cutoff for circulating concentrations of albumin in patients with primary operable breast cancer, the data were analysed on the basis of tertiles. C-reactive protein concentrations were analysed on the basis of a two-point scale depending on whether C-reactive protein was undetectable or detectable (⩽6/>6 mg l−1). The correlation between C-reactive protein and albumin concentrations was performed using the Spearman's Rank correlation. Analysis was performed using SPSS software (SPSS Inc., Chicago, IL, USA).
Results
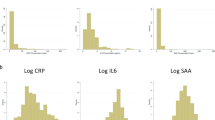
The clinico-pathological characteristics of patients with a diagnosis of invasive primary operable breast cancer (n=314) according to deprivation category are shown in Table 1. In total, 14% of the patients were affluent and 27% were deprived. The median value of albumin in the lowest and highest tertiles was 40 and 46 g l−1 respectively. The median value of C-reactive protein in those patients with a detectable concentration was 9 mg l−1.
There was no significant relationship between the extent of deprivation, age, tumour size, tumour type, grade, and the proportion of patients with involved lymph nodes and ER status. In contrast, deprivation was associated with lower albumin (P<0.001) and higher C-reactive protein (P<0.01) concentrations.
Albumin concentrations were not related to age, size, type, grade, lymph node status or ER status. C-reactive protein was associated with increasing age (P=0.016) and ER negative tumours (P=0.035) but not with size, type, grade or lymph node status.
Discussion
In the present study, we examined a cohort of patients with primary operable breast cancer. Approximately a quarter of the patients were deprived. This is not surprising since half of the most deprived areas in the UK are in the West of Scotland (Gordon et al, 1999).
There was no significant relationship between the extent of deprivation and age, tumour size, type and grade and the proportion of involved lymph nodes. These results are consistent with previous studies (Brewster et al, 2001; Thomson et al, 2001). However, the relationship between deprivation and ER status shown by Thomson et al (2001) was not demonstrated in the present study, probably because our numbers were relatively small.
In the present study, deprivation was associated with lower albumin and higher C-reactive protein concentrations. These results are consistent with our previous study in patients with colorectal cancer, which demonstrated a significant association between deprivation, an elevated C-reactive protein and decreased survival (McMillan et al, 2003b). This relationship between deprivation, C-reactive protein and survival remains to be established in patients with primary operable breast cancer.
The factors underlying the relationship between the extent of deprivation and the systemic inflammatory response are not clear. However, obesity and smoking, which are associated with deprivation, are also known to be associated with elevated C-reactive protein concentrations (Tracy et al, 1997; Koenig et al, 1999). Furthermore, in colorectal cancer at least, there is increasing evidence that the presence of an elevated C-reactive protein concentration is associated with reduced survival (Nielsen et al, 2000; McMillan et al, 2003a).
In summary, the results of the present study demonstrated an association between the extent of deprivation and the magnitude of the systemic inflammatory response in patients with primary operable breast cancer.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Brewster DH, Thomson CS, Hole DJ, Black RJ, Stroner PL, Gillis CR (2001) Relation between socioeconomic status and tumour stage in patients with breast, colorectal, ovarian, and lung cancer: results from four national, population based studies. Br Med J 322: 830–831
Carstairs V, Morris R (1991) Deprivation and health in Scotland. Aberdeen: University Press
Edwards DM, Jones J (1999) Incidence of and survival from upper aerodigestive tract cancer in the UK: the influence of deprivation. Eur J Cancer 25: 968–972
Gabay C, Kushner I (1999) Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 340: 448–454
Gordon D, Dorling D, Shaw M, Davey Smith G (1999) Inequalities in Health: The Evidence. Bristol: Policy Press, University of Bristol and Townsend Centre for International Proverty Research
Koenig W, Sund M, Frohlich M, Fischer HG, Lowel H, Doring A, Hutchinson WL, Pepys MB (1999) C-reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (monitoring trends and determinants in cardiovascular disease) Augsburg Cohort Study, 1984 to 1992. Circulation 99: 237–242
MacKie RM, Hole DJ (1996) Incidence and thickness of primary tumours and survival of patients with malignant melanoma in relation to socioeconomic status. BMJ 312: 1125–1128
Macleod U, Ross S, Twelves C, George WD, Gillis C, Watt GCM (2000) Primary and secondary care management of women with early breast cancer from affluent and deprived areas: retrospective review of hospital and general practice records. Br Med J 320: 1442–1445
McLaren G, Bain M (1998) Breast cancer (ICD9 174). In Deprivation and Health in Scotland; Insight from NHS Data, McLaren G, Bain M (eds). Chapter 7, pp 26–27, Edinburgh: ISD Scotland Publications
McMillan DC, Canna K, McArdle CS (2003a) Systemic inflammatory response predicts survival following curative resection of colorectal cancer. Br J Surg 90: 215–219
McMillan DC, Canna K, McArdle CS (2003b) The effect of deprivation and the systemic inflammatory response on outcome following curative resection for colorectal cancer. Br J Cancer 89: 612–614
Nielsen HJ, Christensen IJ, Sorensen S, Moesgaard F, Brunner N (2000) Preoperative plasma plasminogen activator inhibitor type-1 and serum C-reactive protein levels in patients with colorectal cancer. The RANX05 Colorectal Cancer Study Group. Ann Surg Oncol 7: 617–623
Schrijvers CT, Mackenbach JP, Lutz JM, Quinn MJ, Coleman MP (1995) Deprivation, stage at diagnosis and cancer survival. Int J Cancer 63: 324–329
Scott HR, McMillan DC, Forrest LM, Brown DJ, McArdle CS, Milroy R (2002) The systemic inflammatory response, weight loss, performance status and survival in patients with inoperable non-small cell lung cancer. Br J Cancer 87: 264–267
Thomson CS, Hole DJ, Twelves CJ, Brewster DH, Black RJ, Scottish Cancer Therapy Network (2001) Prognostic factors in women with breast cancer: distribution by socioeconomic status and effect on differences in survival. J Epidemiol Community Health 55: 308–315
Tracy RP, Psaty BM, Macy E, Bovill EG, Cushman M, Cornell ES, Kuller LH (1997) Lifetime smoking exposure affects the association of C-reactive protein with cardiovascular disease risk factors and subclinical disease in healthy elderly subjects. Arterioscl Thromb Vasc Biol 17: 2167–2176
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Al Murri, A., Doughty, J., Lannigan, A. et al. The relationship between deprivation, tumour stage and the systemic inflammatory response in patients with primary operable breast cancer. Br J Cancer 91, 1063–1065 (2004). https://doi.org/10.1038/sj.bjc.6602096
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6602096
Keywords
This article is cited by
-
p53 mutation, deprivation and poor prognosis in primary breast cancer
British Journal of Cancer (2010)
