
Abstract
Data sources
Medline via PubMed, Scopus and Web of Science databases were searched from January 2003 to March 2015 limited to human studies published in English. Manual searches for the relevant reference lists and a grey literature search via Google Scholar were also conducted.
Study selection
Prospective and retrospective studies about the stability of miniscrew implants (MIs) used for orthodontic anchorage into the posterior buccal region were considered. Two review authors independently assessed titles and abstracts, and evaluated full manuscripts for the meta-analysis.
Data extraction and synthesis
The outcome measure was the success rate of MIs which had to be explicitly reported in order to enable its computation as odds ratios with regards to patient factors (age (years), < 20 vs. ≥ 20; sex, male vs. female; jaw of insertion, maxilla vs. mandible) and MI factors (length, < 8 mm vs. ≥ 1.4 mm; diameter, ≤ 1.4 mm vs. > 1.4 mm). The quality of the studies was assessed using the Newcastle-Ottawa Scale (NOS). The meta-analysis was expressed as combined OR and heterogeneity was evaluated (Cochran Q and I2). Subgroup meta-analysis was conducted based on study design, study quality and MIs sample size. Publication bias analysis (Begg's and Eggar's tests) and sensitivity analysis were performed.
Results
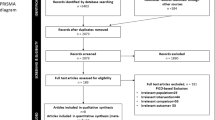
Seventeen non-randomised studies, five prospective and 12 retrospective, were included. Significantly higher success rates were observed for the maxillary MIs (14 studies odds ratio (OR), 2.32; 95% CI, 1.81-4.08), older patients (six studies OR, 1.59; 95% CI, 1.14-2.22), and for longer MIs (four studies OR, 0.56 (1/0.46= 2.17); 95% CI, 0.26-0.20) and MIs with larger diameter (four studies OR, 0.62 (1/0.62= 1.61); 95% CI, 0.40-0.97), whereas there was no difference observed between male and female patients (13 studies OR, 1.18; 95% CI, 0.92-1.51). All subgroups acquired homogeneity except for the components of study design regarding the jaw of insertion.
Conclusions
The results of this meta-analysis based on non-randomised clinical studies showed that jaw of insertion, age, MI length and MI diameter are critical risk factors to the success of MIs, whereas sex was not influential.
Source of Funding
The Basic Science Research Program of the National Research Foundation of Korea was stated as the source of funding.
Similar content being viewed by others

Commentary
Incorporation of MIs is widely accepted and increasingly implemented in the orthodontic practice. When the success of MIs is compromised, they will need to be removed or replaced as they have lost the ability to work as stationary anchors against reaction forces.1 Meta-analyses are able to combine the outcomes from several studies into a single quantitative estimate or summary effect size to identify patterns, although homogeneity is hard to find because of clinical and methodological differences among the studies.2 Hong et al. justified conducting a meta-analysis on the combined OR of the success of orthodontic MIs with respect to patient and MIs factors in order to reduce the obstacles for decision-making that follow from conflicting results between the studies, even as they address similar prognostic factors. The primary outcome - success of MIs - was defined as ‘the absence of clinically detectable mobility when the orthodontic force applied by a clinician was sustained regardless of the predetermined period.’ Through the meta-analysis, the authors were able to identify patterns by combining the outcomes of different non-randomised studies. The authors favourably restricted the population under consideration to patients receiving MIs in the buccal posterior regions only, since these are less variably inconstant, which adds homogeneity to their study. This meta-analysis followed the Cochrane Handbook for Systematic Reviews of Interventions3 and the PRISMA statement.4
Its study selection and data extraction were valid as two independent authors performed them and a consensus procedure for addressing disagreements was implemented to solve discordance in article selection. Although the review provided by the electronic literature search of three databases (PubMed, Scopus and Web of Science) with appropriate keywords and MESH terms is extensive, the inclusion of a European database (eg Embase) would have further strengthened the search by identifying other published records that may have not been retrieved. A potential limitation to this study is that the authors added limits in their search strategy to eliminate non-English publications, studies containing microbiology or patient satisfaction, animal and in vitro studies, radiographic evaluations, case reports, meta-analysis, narrative and systematic reviews. Excluding non-English records was justified by the authors pursuant to Morrison et al.'s5 findings that these studies have a tendency to exaggerate treatment effects and to be of lower quality. However, this is still a controversial issue.6,7 On the one hand, the Cochrane Collaboration recommends searching without language restrictions to avoid introducing language bias3 in the results, in spite of the fact that RCTs are more often published in English journals.8 On the other hand, the likelihood of publication bias may have been reduced with the trim-and-fill method after finding bias through the Begg's and Eggar's tests, as was the case with the subgroup of retrospective studies assessing age factors. These statistical tests were correctly performed and reported in Table 4 of the review.
The number of studies according to each reason of exclusion was reported. Nonetheless, the citations were listed neither in the manuscript nor in the appendix.
The scientific quality of the included studies was assessed properly in formulating clinical recommendations because study design, study quality and sample size were considered in the subgroup analyses. This followed the 9-star NOS assessment, the quality assessment recommended by the Cochrane Collaboration to score non-randomised studies.9 This method has previously raised concerns as it may produce highly arbitrary results.10 However, in this case, only two prospective studies in this analysis had a high score (7-9 points), whereas the remaining prospective studies and all the retrospective studies had a medium score (4-6 points).
The methods used to combine the results of studies in a subgroup meta-analysis were appropriate since the p-values of the Q-test were lesser than 0.10, and I2 values were less than 30%. Therefore, low heterogeneity was found.
The source of support for this study was clearly acknowledged in the systematic review (the Korean Ministry of Education). However, the conflict of interest of each included study was not explicitly stated in the review.
Only five main systematic reviews were found in the dental literature related to orthodontic MIs, and no meta-analyses were found prior to 2012.11,12,13,14,15 The following can be concluded from agreement and disagreement between Hong et al. and other similar studies. In 2012 a meta-analysis16 found similar results to Hong et al. regarding success in the jaw of insertion and sex, whereas results differed for age, MIs length and diameter. In 2014, the same prognostic factors as Hong et al. were analysed by a meta-analysis17 that found similar results regarding success in the jaw of insertion, sex and age, whereas results differed for MIs length and diameter.
The summarised review presented herein provides valuable recommendations regarding the clinical implications of prognostic factors of MIs published in The Korean Journal of Orthodontics(IF=1.173). This journal may be considered for being regularly searched for articles for inclusion by Evidence-based Dentistry.18 The meta-analysis of primarily medium-quality primary studies concluded that MIs inserted in the maxilla, patients who are over 19 years of age, and long and large MIs were predictors of higher success of MIs, whereas no difference was found between male and female patients.
References
Suzuki EY, Suzuki B . Placement and removal torque values of orthodontic miniscrew implants. Am J Orthod Dentofacial Orthop 2011; 139: 669–678.
Uman LS . Systematic reviews and meta-analyses. J Can Acad Child Adolesc Psychiatry 2011; 20: 57–59.
Higgins JPT, Green S . Cochrane handbook for systematic reviews of interventions Wiley-Blackwell: Chichester, 2014.
Moher D, Liberati A, Tetzlaff J . Altman DG ; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 2009; 62: 1006–1012.
Morrison A, Polisena J, Husereau D, et al. The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. Int J Technol Assess Health Care 2012; 28: 138–144.
Melander H, Ahlqvist-Rastad J, Meijer G, Beermann B . Evidence b(i)ased medicine--selective reporting from studies sponsored by pharmaceutical industry: review of studies in new drug applications. BMJ 2003; 326: 1171–1173.
Jüni P, Holenstein F, Sterne J, Bartlett C, Egger M . Direction and impact of language bias in meta-analyses of controlled trials: empirical study. Int J Epidemiol 2002; 31: 115–123.
Fan H, Song F . An assessment of randomized controlled trials (RCTs) for non-communicable diseases (NCDs): more and higher quality research is required in less developed countries. Sci Rep 2015; 5: 13221.
Wells GA, Shea B, O'Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analyses. [cited 2016 June] Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm
Stang A . Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010; 25: 603–605.
Cornelis MA, Scheffler NR, De Clerck HJ, Tulloch JF, Behets CN . Systematic review of the experimental use of temporary skeletal anchorage devices in orthodontics. Am J Orthod Dentofacial Orthop 2007; 131: S52–58.
Chen Y, Kyung HM, Zhao WT, Yu WJ . Critical factors for the success of orthodontic mini-implants: a systematic review. Am J Orthod Dentofacial Orthop 2009; 135: 284–291.
Reynders R, Ronchi L, Bipat S . Mini-implants in orthodontics: a systematic review of the literature. Am J Orthod Dentofacial Orthop 2009; 135: 564. e1–19; discussion 564–565.
Crismani AG, Bertl MH, Celar AG, Bantleon HP, Burstone CJ . Miniscrews in orthodontic treatment: review and analysis of published clinical trials. Am J Orthod Dentofacial Orthop 2010; 137: 108–113.
Schätzle M, Männchen R, Zwahlen M, Lang NP . Survival and failure rates of orthodontic temporary anchorage devices: a systematic review. Clin Oral Implants Res 2009; 20: 1351–1359.
Papageorgiou SN, Zogakis IP, Papadopoulos MA . Failure rates and associated risk factors of orthodontic miniscrew implants: a meta-analysis. Am J Orthod Dentofacial Orthop 2012; 142: 577–595. e577.
Dalessandri D, Salgarello S, Dalessandri M, et al. Determinants for success rates of temporary anchorage devices in orthodontics: a meta-analysis (n > 50). Eur J Orthod 2014; 36: 303–313.
Richards D . Keeping up to date. Evid Based Dent 2015; 16: 98.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Prof. Hoi-Jeong Lim. Department of Orthodontics, School of Dentistry, Dental Science Research Institute, Chonnam National University, 33 Yongbong-ro, Buk-gu, Gwangju 61186, Korea. E-mail: hjlim@jnu.ac.kr
Hong SB, Kusnoto B, Kim EJ, BeGole EA, Hwang HS, Lim HJ. Prognostic factors associated with the success rates of posterior orthodontic miniscrew implants: A subgroup meta-analysis. Korean J Orthod 2016; 46: 111–126. doi: 10.4041/kjod.2016.46.2.111.
Rights and permissions
About this article

Cite this article
Afrashtehfar, K. Patient and miniscrew implant factors influence the success of orthodontic miniscrew implants. Evid Based Dent 17, 109–110 (2016). https://doi.org/10.1038/sj.ebd.6401202
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401202
