
Abstract
Study design:
A case report of myelopathic hypoplasia of the atlas with situs inversus totalis.
Objectives:
To describe a case of cervical myelopathy caused by hypoplasia of the atlas with situs inversus totalis, and to briefly review the pertinent literature.
Setting:
Department of Orthopaedic Surgery, Kagoshima, Japan.
Methods:
The history, results of examination, and findings of radiographic imaging studies for a 56-year-old man with a 10-year history of progressive myelopathy who presented to our hospital are described.
Results:
Imaging studies revealed congenital hypoplasia of the atlas, ossification of the posterior longitudinal ligament at the levels of C3–C4, and situs inversus totalis. He underwent laminectomy of the atlas and laminoplasty of C3–C7 for decompression of the spinal cord. Operative intervention resulted in significant neurological improvement and relief of occipital neuralgia.
Conclusion:
To our knowledge, no case of myelopathic hypoplasia of the atlas with situs inversus totalis has previously been described. When encountering inherited disorders such as situs inversus totalis, a thorough search must be made for anomalies of the craniovertebral junction.
Similar content being viewed by others
Introduction
Hypoplasia of the atlas as a cause of cervical stenosis at the level of C1 is a rare congenital anomaly of the craniovertebral junction. It can occur in isolation or in association with systemic anomalies. Situs inversus is a rare condition in which there is left-right reversal in position of the thoracic and abdominal viscera. We describe a case of cervical myelopathy caused by hypoplasia of the atlas with situs inversus totalis.
Case report
A 56-year-old man had a 10-year history of progressive bilateral numbness of the hands and disturbance of gait, which had gradually progressed and had extended to the lower extremities bilaterally. On admission, he was unable to walk without aid and his hand coordination was impaired. He also had urinary frequency and urinary incontinence. His past medical history included aortic stenosis, for which he had undergone aortic valve replacement at age 52.
He was of short stature, with a height of 151 cm (below the mean−2 SD). He had pain in his left upper extremity and severe occipital neuralgia on extension of the neck. Muscle tone was increased in all four extremities. Motor examination revealed weakness of the musculature in the upper extremities. Hyperreflexia was noted throughout both upper and lower extremities, with bilateral Hoffman's and Babinski signs. Sensory examination revealed decreased light touch, vibration sensation, and proprioception in all four extremities.
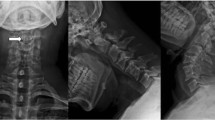
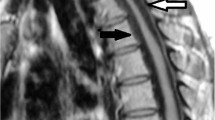
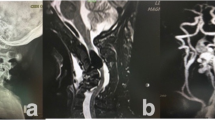
Computed tomography (CT) of the thorax and abdomen disclosed dextrocardia and situs inversus in the abdomen (Figure 1). Plain radiographs of the cervical spine revealed marked narrowing of the spinal canal at the level of the atlas, with a retrodental space of 8 mm. CT of the cervical spine revealed hypoplasia of the atlas and ossification of the posterior longitudinal ligament (OPLL) at the levels of C3–C4 (Figure 2). Magnetic resonance imaging revealed hyperintense change in the spinal cord on T2-weighted images suggesting edema due to spinal cord compression by the hypoplastic posterior arch and OPLL (Figure 3a).

Computed tomography. (a) Dextrocardia is observed. (b) Situs inversus of the abdomen is noted

Midsagittal CT reconstruction of the cervical spine reveals marked stenosis of the spinal canal at the level of the atlas. Ossification of the posterior longitudinal ligament at C3–C4 level is also seen

(a) Sagittal T2-weighted magnetic resonance imaging of the cervical spine obtained before the operation revealing constriction of the dural sac at the level of the atlas and hyperintense change in the spinal cord. (b) Sagittal T2-weighted magnetic resonance imaging obtained after laminectomy of the atlas and laminoplasty of C3–C7 demonstrating that the posterior bony compressive elements have been removed, though hyperintense change persists within the spinal cord
The patient underwent laminectomy of the atlas and laminoplasty of C3–C7 (Figure 3b). The patient's severe occipital neuralgia disappeared and some improvement in neurological symptoms such as numbness and spasticity of the extremities, clumsiness of both hands, and urinary incontinence was noted within 3 weeks. By 6 months after surgery, his sensory disturbance and muscle weakness had resolved almost completely.
Discussion
Knowledge of embryological development is essential for understanding the origin of hypoplasia of the atlas. Chondrification of the posterior arch of the atlas begins at the pedicles, during the 6th week of embryogenesis, and ends in the midline during the 4th month. This cartilaginous arch ossifies by 3–4 years of age.1 Hypoplasia of the atlas could be caused by premature fusion of the cartilaginous neurocentral synchondrosis, which occurs between the 6th week and 4th month of gestation, suggesting failure of chondrogenesis and early ossification of the neural arches.
The clinical signs and symptoms of mechanical constriction at the subforaminal space between the occiput, atlas, and axis are neck or occipital pain with transient weakness of the limbs, which is caused by ischemia in the territory of the vertebrobasilar artery on extension of the neck,2 as noted in our patient. Clinical manifestations are characteristically noted somewhat late in adulthood despite the congenital nature of this anomaly. Hypoplasia of the atlas is generally believed to only rarely cause myelopathy, unless spondylotic change in the lower cervical spine occurs. Decreased range of motion at the lower cervical levels caused by spondylosis is thought to be of importance in causing increased movement of the atlas, with subsequent compression of the spinal cord.3 In our patient, radiological investigations revealed the presence of C3–C4 OPLL, which was also thought to have decreased the range of motion of the neck, with subsequent increased movement of the atlas.
Situs inversus totalis can occur as an isolated phenomenon or as one of the features of syndromes such as Kartagener syndrome, polyasplenia, and agnathia-holoprosencephaly-situs inversus. To our knowledge, association of it with hypoplasia of the atlas has not been reported previously. It is possible that the conditions noted in our patient are all within the spectrum of mesodermal malformations resulting from an early abnormality in the primitive streak or embryonic mesoderm.4 The period when the primitive streak develops is also that when the axis of symmetry is established.5 We speculate that an early abnormality in development might give rise both to hypoplasia of the atlas and situs inversus totalis as manifestations of mesodermal malformation.
References
Vangilder JC, Menezes AH . Craniovertebral junction abnormalities. Clin Neurosurg 1983; 30: 514–530.
Coria F, Rebollo M, Quintana F, Polo JM, Berciano J . Occipitoatlantal instability and vertebrobasilar ischemia: case report. Neurology 1982; 32: 303–305.
Phan N, Marras C, Midha R, Rowed D . Cervical myelopathy caused by hypoplasia of the atlas: two case reports and review of the literature. Neurosurgery 1998; 43: 629–633.
Russell LJ, Weaver DD, Bull MJ . The axial mesodermal dysplasia spectrum. Pediatrics 1981; 67: 176–182.
Smith DW, Bartlett C, Harrah LM . Monozygotic twinning and the Duhamel anomalad (imperforate anus to sirenomelia): a nonrandom association between two aberrations in morphogenesis. Birth Defects Orig Artic Ser 1976; 12: 53–63.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Tofuku, K., Koga, H., Yone, K. et al. Hypoplasia of the atlas causing cervical myelopathy with situs inversus totalis. Spinal Cord 45, 806–808 (2007). https://doi.org/10.1038/sj.sc.3102042
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102042
Keywords
This article is cited by
-
A unique case of right-sided Poland syndrome with true dextrocardia and total situs inversus
European Journal of Pediatrics (2013)
