
Abstract
Study design: Report of a rare case of an elderly patient with late onset of Arnold Chiari malformation type I with associated syringomyelia that was successfully treated with foramen magnum decompression.
Objective: To report this rare case along with a literature review.
Setting: Gifu, Japan.
Methods: A 69-year-old woman with a 4-year history of dull pain in her right arm was referred to the clinic. After physical and radiographical examinations, she was diagnosed with Arnold Chiari malformation type I with associated syringomyelia. A foramen magnum decompression by the removal of the outer layer of the dura mater was performed.
Results: At 2 years postoperatively, MRI revealed a decrease in the size of the syringomyelia. Her symptoms had also remarkably improved.
Conclusions: A rare case of symptomatic Arnold Chiari malformation type I with associated syringomyelia in an elderly woman was successfully treated with foramen magnum decompression by the removal of the outer layer of the dura mater.
Similar content being viewed by others
Introduction
In Arnold Chiari malformation type I, abnormal cerebrospinal fluid flow occurs and frequently results in syringomyelia.1, 2 Various surgical methods for treating neurologically symptomatic cases of syringomyelia associated with Arnold Chiari malformation type I have been reported.1, 3, 4, 5, 6, 7 Posterior fossa craniectomy (foramen magnum decompression), with1 or without plugging of the obex,3, 8, 9 has been one of the most commonly performed surgical procedures in the belief that it would ameliorate the abnormal cerebrospinal fluid flow. However, this surgical procedure has been primarily indicated for treating relatively young and middle-aged patients.1, 3, 4, 6, 10 Few reports are available on the late onset of symptoms associated with Arnold Chiari malformation type I in elderly patients and possible surgical treatments.8, 11 This report is of a very rare case of an elderly woman with late-onset Arnold Chiari malformation type I and syringomyelia that was successfully treated with foramen magnum decompression.
Case report
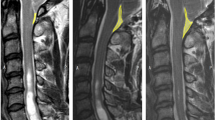
In May 2000, a 69-year-old woman was referred to the clinic. She had experienced a history of dull pain in her right arm for 4 years. Additionally, dorsalgia and bilateral leg pain radiating from her gluteal region appeared 1 year prior to her evaluation. Owing to the dorsalgia and leg pain, her gait became gradually disturbed. On her first visit to the clinic, the neurological examination revealed sensory disturbances in her right arm, trunk and thigh. Deep tendon reflexes were depressed in the right arm and exaggerated in both legs. Plain X-ray of the cervical spine showed moderate degenerative changes. MRI showed cerebellar tonsillar herniation into the foramen magnum and syringomyelia from the medulla oblongata to the T11 level (Figure 1). However, compression of the spinal cord due to spondylotic change or disc herniation at the cervical spine level was not observed. Therefore, she was diagnosed with symptomatic Arnold Chiari malformation type I with associated syringomyelia.

Preoperative T1-weighted MRI scan of the occipitocervical junction and the cervical spine. Sagittal section just at the midline of the spinal cord demonstrates syringomyelia from medulla oblongata to upper thoracic levels
Surgical procedure
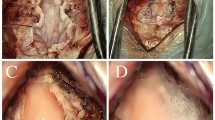
Foramen magnum decompression by the removal of the outer layer of the dura mater was performed, as reported by Isu et al6 in 1993. First, a suboccipital craniectomy and removal of the arch of C1 was performed. It is worth noting that in a suboccipital craniectomy, the occipital bone is removed far laterally.6 A cruciate incision was made in the outer layer of the dura mater. The outer layer was dissected from the inner layer and removed. Immediately after this removal, the inner layer of the dura mater began bulging and the cerebellar tonsil was pulsating. Therefore, the effectiveness of decompression at the foramen magnum was immediately ascertained.
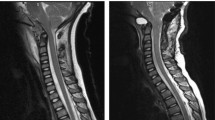
At 1 month postoperatively, the sensory disturbances in her right arm and both legs improved and her difficulty in walking disappeared. The dorsalgia and bilateral leg pain radiating from her gluteal region were remarkably reduced. No perioperative complications occurred. In the postoperative MRI, both the upper deviation of the cerebellar tonsil and a reduction in size of the syrinx were recognized (Figure 2). After a 2-year follow-up, her postoperative course has been excellent.

Postoperative T1-weighted MRI scan of the occipitocervical junction and cervical spine. Sufficient decompression at the foramen magnum, upper deviation of cerebeller tonsil and remarkable reduction in size of the syringomyelia are shown
Discussion
According to the literature, the clinical condition of this patient is doubly rare and worth reporting. First, because the Arnold Chiari malformation type I with associated syringomyelia initially manifested its symptoms at an advanced age, and second, because a satisfactory surgical outcome following foramen magnum decompression was achieved in an elderly patient.
There are several reports on symptomatic Arnold Chiari malformation type I associated with syringomyelia.1, 3, 8, 9, 10, 12, 13 Among these, a few authors presented cases with late onset of symptoms due to Arnold Chiari malformation type I-associated syringomyelia.8, 12 Moriwaka et al14 reported that the average age of onset of the first symptoms due to syringomyelia was 28 -years old and that syringomyelia due to an Arnold Chiari malformation showed a tendency to have a younger age of onset.
In the case reported here, both MRI and CT-myelogram revealed that there was no compression of the spinal cord due to degenerative changes in the cervical spine. Therefore, foramen magnum decompression was chosen to treat the patient, with the expectation that this procedure would improve the cerebrospinal fluid flow and alleviate her symptoms.
There is apparently only one other report, by Geroldi et al,11 of the successful surgical treatment of an elderly patient using foramen magnum decompression for Arnold Chiari malformation type I with associated syringomyelia. That case differs from the present one in that a cervico-spinal decompression was performed, although the surgical procedure was not precisely described. In the current case, because there was no observable compression of the cervical spinal cord, foramen magnum decompression by the removal of the outer layer of the dura mater6 was performed. Among the various methods for foramen magnum decompression, this method has several advantages. First, it is less invasive in comparison with other previously reported procedures. Second, the reported incident rate of readhesion is low, and third, the decompression effect is maintained for a long period because the inner layer of the dura mater is preserved.15 In addition, because this foramen magnum decompression procedure is extradural, there are no demonstrated risks of such postoperative complications6 as cerebrospinal fluid collection in the operative wound,4 pseudomeningocele10 or meningitis.9, 16 Therefore, the authors are convinced that this method is advantageous when performing a foramen decompression in an elderly patient.
In a report by Isu et al,6 the oldest patient who underwent this procedure was 54 years old. This patient presented with symptoms induced by a cervical lesion at 65 years of age. In elderly patients, cervical myelopathy is encountered frequently in clinical practice and is difficult to differentiate from other conditions by a physical examination and plain X-ray alone. The symptoms of Arnold Chiari malformation type I with associated syringomyelia vary and this clinical condition has no pathognomonic clinical sign.8, 17 In the current patient, the MRI scan from the occipitocervical junction down to the cervical spine was very useful in making a correct diagnosis. Moreover, the MRI scan revealed the postoperative reduction of the syringomyelia, which corresponded well with the alleviation of her symptoms. Awareness of symptomatic Arnold Chiari malformation type I-associated syringomyelia in elderly patients would help clinicians make correct diagnoses.
Conclusion
A rare case of Arnold Chiari malformation type I associated with syringomyelia was reported in an elderly woman, who presented with sensory disturbances and pain in her right arm, trunk and both legs. She was successfully treated by foramen magnum decompression by the removal of the outer layer of the dura mater.
References
Gardner WJ . Hydrodynamic mechanism of syringomyelia. J Neurol Neurosurg Psychiatry 1965; 28: 247–259.
Williams B . On the pathogenesis of syryngomyelia: a review. J Roy Soc Med 1980; 73: 798–806.
Logue J, Edwards MR . Syringomyelia and its surgical treatment – an analysis of 75 patients. J Neurol Neurosurg Psychiatry 1981; 44: 273–284.
Matsumoto T, Symon L . Surgical management of syringomyelia – Current results. Surg Neurol 1989; 32: 258–265.
Isu T, Iwasaki Y, Akino M, Abe H . Syryngo-subarachnoid shunt for syryngomyelia associated with Chiari malformation (type 1). Acta Neurochir (Wien) 1990; 107: 152–160.
Isu T, Sasaki H, Takamura H, Kobayashi N . Foramen magnum decompression with removal of the outer layer of the dura as treatment for syringomyelia occurring with Chiari I malformation. Neurosurgery 1993; 33: 845–849 discussion 849-850.
Goel A, Desai K . Surgery for syringomyelia: an analysis based on 163 surgical cases. Acta Neurochir (Wien) 2000; 142: 293–301 discussion 301-302.
Levy WJ, Mason L, Hahn JF . Chiari malformation presenting in adults: a surgical experience in 127 cases. Neurosurgery 1983; 12: 377–390.
Koyanagi I et al. Surgical treatment of syringomyelia with Chiari malformation—Effect of foramen magnum decompression. Spinal Surgery (Tokyo) 1991; 5: 43–49 (in Japanese).
Batzdorf U . Chiari I malformation with syringomyelia. J Neurosurg 1988; 68: 726–730.
Geroldi C, Frisoni GB, Bianchetti A, Trabucchi M, Bricolo A . Arnold-Chiari malformation with syringomyelia in an elderly woman. Age Ageing 1999; 28: 399–400.
Banerji NK, Millar JHD . Chiari malformation presenting in adult life. Its relationship with syringomyelia. Brain 1974; 97: 157–168.
Pidcock FS, Sandel ME, Faro S . Late onset of syringomyelia after traumatic brain injury: association with Chiari I malformation. Arch Phys Med Rehabil 1994; 75: 695–698.
Moriwaka F, Tashiro K, Tachibana S, Yada K . Epidemiology of syringomyelia in Japan–the nationwide survey. Rinsho Shinkeigaku 1995; 35: 1395–1397 (in Japanese).
Isu T . Surgical treatment for syryngomyelia associated with a Chiari malformation. Nippon Saigai Igakukai Kaishi 1995; 43: 788–797 (in Japanese).
Hoffman HJ, Hendrick EB, Humphreys RP . Manifestations and management of Arnold-Chiari malformation in patients with myelo-meningocele. Child's Brain 1975; 1: 255–259.
Depreitere B, Van Calenbergh F, Van Loon J, Goffin J, Plets C . Posterior fossa decompression in syryngomyelia associated with a Chiari malformation: a retrospective analysis of 22 patients. Clin Neurol Neurosurg 2000; 102: 91–96.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Takigami, I., Miyamoto, K., Kodama, H. et al. Foramen magnum decompression for the treatment of Arnold Chiari malformation type I with associated syringomyelia in an elderly patient. Spinal Cord 43, 249–251 (2005). https://doi.org/10.1038/sj.sc.3101675
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101675
Keywords
This article is cited by
-
Posterior Fossa Decompression Combined with Resection of the Cerebellomedullary Fissure Membrane and Expansile Duraplasty: A Radical and Rational Surgical Treatment for Arnold–Chiari Type I Malformation
Cell Biochemistry and Biophysics (2014)
-
Chiari I malformation associated with syringomyelia: a retrospective study of 316 surgically treated patients
Spinal Cord (2008)
