
Abstract
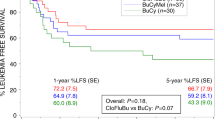
Infections during neutropaenia contribute still significantly to mortality and morbidity after high-dose therapy and autologous stem cell transplantation. Further acceleration of haemopoietic recovery seems impossible for biological reasons. Another approach to shorten neutropaenia could be to remove drugs from high-dose therapy protocols with strong contribution to immunosuppression and neutropaenia and unproven antineoplastic activity. In this retrospective matched-pair analysis, conventional busulphan/cyclophosphamide (Bu/Cy) high-dose therapy was compared to single-agent busulphan conditioning before autologous stem cell transplantation. This modification led to a significant shorter neutropaenic interval by protraction of cell decrease and to a significant mitigation of neutropaenia. After single-agent busulphan conditioning, leucocytes dropped below 1/nl at median 1.5 days later when compared to the patients from the busulphanBu/Cy control group (P=0.001). In a significant percentage of patients (n=6, 60%) leucocytes did not fall below 0.5 cells/nl at any time. In contrast, all patients from the Bu/Cy control group experienced deep neutropaenia (P=0.004). Thrombocytopaenia and requirement for transfusions of platelets or red cells were not influenced. Antineoplastic activity seemed to be preserved as determined by survival analysis. In conclusion, modification of high-dose regimen with the intention to shorten neutropaenia with preserved antitumour activity could be an approach to reduce infection-related morbidity and mortality and to consider economic necessities.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Wingard JR . Opportunistic infections after blood and marrow transplantation. Transpl Infect Dis 1999; 1: 3–20.
Kennedy MJ . Peripheral blood progenitor cell mobilization: a clinical review. Pharmacotherapy 1998; 18 (Part 2): 3S–8S.
Thomas ED, Blume KG, Forman SJ (eds). Hematopoietic Cell Transplantation, 2nd edn. Blackwell Science: Malden, 1999.
Kruger WH, Bohlius J, Cornely OA, Einsele H, Hebart H, Massenkeil G et al. Antimicrobial prophylaxis in allogeneic bone marrow transplantation. Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Haematology and Oncology. Ann Oncol 2005; 16: 1381–1390.
Marie JP, Vekhoff A, Pico JL, Guy H, Andremont A, Richet H . Neutropenic infections: a review of the French Febrile Aplasia Study Group trials in 608 febrile neutropenic patients. J Antimicrob Chemother 1998; 41 (Suppl D): 57–64.
Mossad SB, Longworth DL, Goormastic M, Serkey JM, Keys TF, Bolwell BJ . Early infectious complications in autologous bone marrow transplantation: a review of 219 patients. Bone Marrow Transplant 1996; 18: 265–271.
Kruger W, Russmann B, Kroger N, Salomon C, Ekopf N, Elsner HA et al. Early infections in patients undergoing bone marrow or blood stem cell transplantation – a 7 year single centre investigation of 409 cases. Bone Marrow Transplant 1999; 23: 589–597.
Kruger WH, Hornung RJ, Hertenstein B, Kern WV, Kroger N, Ljungman P et al. Practices of infectious disease prevention and management during hematopoietic stem cell transplantation: a survey from the European group for blood and marrow transplantation. J Hematother Stem Cell Res 2001; 10: 895–903.
Ball ED, Lister JD, Law P (eds). Hematopoietic Stem Cell Therapy, 1st edn. Churchill Livingstone: Philadelphia, 2000.
Clift RA, Buckner CD, Thomas ED, Bensinger WI, Bowden R, Bryant E et al. Marrow transplantation for chronic myeloid leukemia: a randomized study comparing cyclophosphamide and total body irradiation with busulphan and cyclophosphamide. Blood 1994; 84: 2036–2043.
Zander AR, Berger C, Kroger N, Stockschlader M, Kruger W, Horstmann M et al. High dose chemotherapy with busulfan, cyclophosphamide, and etoposide as conditioning regimen for allogeneic bone marrow transplantation for patients with acute myeloid leukemia in first complete remission. Clin Cancer Res 1997; 3 (Part 2): 2671–2675.
Anderson JE, Tefferi A, Craig F, Holmberg L, Chauncey T, Appelbaum FR et al. Myeloablation and autologous peripheral blood stem cell rescue results in hematologic and clinical responses in patients with myeloid metaplasia with myelofibrosis. Blood 2001; 98: 586–593.
Olavarria E, Kanfer E, Szydlo R, O'Brien S, Craddock C, Apperley J et al. High-dose busulphan alone as cytoreduction before allogeneic or autologous stem cell transplantation for chronic myeloid leukaemia: a single-centre experience. Br J Haematol 2000; 108: 769–777.
Acknowledgements
We thank Dr BP Jäger from the Department of Biostatistics for his advices and the nurses from the BMT unit for the excellent patient care.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kiefer, T., Krüger, W., Schüler, F. et al. The modification of high-dose therapy shortens the duration of neutropaenia by delay of leucocyte nadir. Bone Marrow Transplant 37, 1087–1091 (2006). https://doi.org/10.1038/sj.bmt.1705390
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705390
